
Bimat
Generic 3ml bimat mastercard
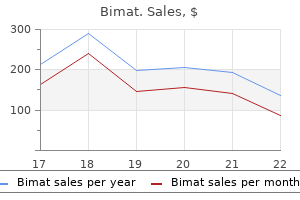
Among the most frequent procedures medicine 3x a day bimat 3 ml low price, as many as one in five patients were readmitted within 30 days. The lowest readmission rates were for procedures related to childbirth and the reproductive organs (Cesarean section, 2. Procedures with the highest readmission rates Table 2 lists procedures ranked by the highest readmission rates. Across all inpatient procedures, 30-day readmission rates reached a high of almost one in three patients for kidney transplant (29. All-cause 30-day readmissions ranked by the most frequent procedures* performed during the index stay, U. All-cause 30-day readmissions ranked by the highest readmission rates for procedures* performed during the index stay, U. Readmission rates by age and insurance status for selected procedures Figures 1?6 provide details on 30-day all-cause readmission rates for the six procedures from Table 2 that involved more than 100,000 index stays and had overall readmission rates of at least 15 percent. The highest readmission rate was seen for patients with an expected payer of Medicare (25. All-cause 30-day readmission rates for amputation of a lower extremity by age and insurance status, U. Readmission rates progressively were higher with advancing age, increasing from 13. All-cause 30-day readmission rates for debridement of a wound, infection, or burn by age and insurance status, U. Readmission rates were identical for patients with an expected payer of Medicare or Medicaid (20. All-cause 30-day readmission rates for heart valve procedures by age and insurance status, U. All-cause 30-day readmission rates for insertion, revision, replacement, removal of cardiac pacemaker or cardioverter/defibrillator by age and insurance status, U. The readmission rate was highest for patients with an expected payer of Medicaid (19. All-cause 30-day readmission rates for coronary artery bypass graft by age and insurance status, U. Overall, across select procedures with high volume (more than 100,000 index stays) and high readmission rates (at least 15 percent), the 30-day readmission rate consistently was higher for patients aged 65 years and older than for younger adults. In terms of payer, patients with Medicare and Medicaid coverage also consistently had higher readmission rates than patients with private insurance or those who were uninsured. These databases include reliable, verified synthetic patient identifiers that can be used to track a person across hospitals within a State. For 2010, readmissions data were available from 18 States: Alaska, Arkansas, California, Florida, Georgia, Hawaii, Louisiana, Massachusetts, Mississippi, Missouri, Nebraska, New Mexico, New York, South Carolina, Tennessee, Utah, Virginia, and Washington. These 18 States are geographically dispersed and account for 46 percent of the total U. The study population in this readmissions analysis file included discharges from community, nonrehabilitation, nonspecialty hospitals. Weights for national estimates were developed using poststratification on hospital characteristics (Census region, urban-rural location, teaching capabilities, bed size, and control/ownership) and patient age groups. Readmissions the 30-day readmission rate is defined as the number of admissions for each procedure for which there was at least one subsequent hospital admission within 30 days, divided by the total number of admissions from January through November 2010. That is, when patients are discharged from the hospital, they are followed for 30 days in the data. If any readmission to the same or different hospital occurs during this time period, the admission is counted as a readmission. No more than one readmission is counted within the 30-day period, because the outcome measure assessed is "percentage of admissions who are readmitted. In the case of admissions for which there was more than one readmission in the 30-day period, the data presented in this Statistical Brief reflect the characteristics and costs of the first readmission. Every qualifying hospital stay is counted as a separate index (starting point) admission. Thus, a single patient can be counted multiple times during the course of the January through November observation period. In addition, index admissions do not require a prior "clean period" with no hospitalizations; that is, a hospital stay may be a readmission for a prior stay and the index admission for a subsequent readmission. Excluded are long-term care, rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. This categorization includes patients who are dually eligible for Medicare and Medicaid under Medicare. For this Statistical Brief, categorization of readmission counts by expected payer was based on the index stay. Acknowledgments the authors would like to acknowledge the contributions of Marguerite Barrett and Minya Sheng for work on programming. The methods of the review and the results of the search are described, including sources and search terms used to identify relevant published research. They provide validated evidence of health from the point of view of the user or patient. They may be used to assess levels of health and need in populations, and in users of services they can provide evidence of the outcomes of services for the purposes of audit, quality assurance and comparative performance evaluation. They may also improve the quality of interactions between health professionals and individual service users. Furthermore, Lord Darzi?s report ?High Quality Care for All (2008) outlines policy regarding payments to hospitals based on quality measures as well as volume. Generic instruments comprise items intended to be relevant to the widest range of patient conditions and the general population. Preferencebased measures are also broad in content but additionally provide utilities or values regarding health (for use in, for example, cost-utility analyses of interventions). Condition-specific instruments are often more focused on a particular disease or health condition (for example, diabetes), a patient population (for example, older people), a specific problem or symptom (for example, pain), or a described function (for example, activities of daily living). For any given area of health, condition-specific instruments may have greater clinical appeal due to the inclusion of content specific to particular conditions, and the likelihood of increased responsiveness to interventions. It has been recommended that a combination of a generic or utility measure with a specific measure be used in the assessment of patient-reported health outcomes, on the grounds that the complementary content of the two types of measure, when combined, should assess a full range of aspects of health relevant to the particular population concerned. However, consensus is often lacking as to which instrument to use for specific purposes and contexts (Garratt et al. These include measurement issues, such as reliability, validity, responsiveness and precision, as well as practical issues, such as acceptability and feasibility. Measuring patientreported outcomes should clearly be a key component in assessing the effectiveness of this strategy. A vein or artery from elsewhere in the body (often one of the internal thoracic arteries, or the great saphenous vein from the leg) is used to form a graft, creating an alternative route around the damaged area. It involves the insertion of a catheter into a narrowed or stenotic section of a coronary artery, usually via a femoral artery; a balloon is then inflated to widen the stenosed area. A wire mesh tube or stent is often left in place to maintain the patency of the vessel; in suitable cases, medically coated or ?drug-eluting stents may be used to prevent restenosis and/or an inflammatory reaction to the stent. It may also be less effective in terms of quality-oflife and cost benefits if repeat revascularisation is required, and in patients with multi-vessel disease (Poulin et al. Structure of the report the methods of the review and the results of the search are described, including sources and search terms used to identify relevant published research. Supplementary searches included scanning the reference lists of review articles and others, checking instrument websites, where found, and drawing on other bibliographic resources. Quality of Life Research the National Institute for Health Research: Health Technology Assessment Programme, published research was also searched. Searches identified nearly 4,000 potentially relevant records; of these, 259 papers were retrieved and reviewed in full. When assessed against the inclusion criteria, 128 studies were included in the review (Table 1). The measure comprises 15 items encompassing physical, mental, and social well-being, with five graded responses for each item; there is no summed score. A set of preference weights elicited from the general population is used to generate a single index score between 0 and 1, where 0 is the worst (death) and 1 the best possible health.
Syndromes
- Endoscopic retrograde cholangiopancreatography (ERCP)
- Take advantage of other people to achieve his or her own goals
- Take the drugs your doctor told you to take with a small sip of water.
- Shortening of the forearm bones near the wrist
- If the movements are due to a disease, the disorder should be treated.
- Dry the ear thoroughly after exposure to moisture.
Buy 3 ml bimat free shipping
A neuroaxial anaesthetic technique was chosen through shared decision making with the patient medicine for runny nose buy generic bimat 3 ml on-line. Obstruction of Further pharmacological therapies included 1mg of Alfenanil, 1g of Paracetamol the airway is the major challenge in the neonatal period. International Journal of Obstetric Anesthesia Vol 15, Issue 2, April 2006: 115123 3. The foetus airway was exposed 1Lithuanian University Of Health Sciences Kaunas (Lithuania) and tracheal intubation was successfully achieved after a single attempt by the neonatologist and fetal extraction was completed. Patient was uneventfully extubated at the end of surgery and Case Report: A 19 year old primipara at 37 weeks of gestation were transfered discharged home on postoperative day 4. Multidisciplinary team (neurosurgeon, cardiologist, anaesthesiologist, obsterician) decided to do urgent caesarian delivery. Spina bifda is not an absolute contraindication for epidural or spinal anaesthesia but it could be less effective and more diffcult to perform (2). Regarding fetal complications, prematurity and a4%mortality rate are the main concern. Maternal hypoxia and hypercarbia can threat uteroplacental perfusion and 1 1 1 produce, even, fetal death. The anesthetic management leaded apron was placed at the level of the iliac crests, and the radiation feld was should focus on maintaining uteroplacental circulation, achieving profound kept away from the uterus. Fetal anesthesia is necessary in some was placed during the frst 5 minutes and, after, Remifentanil 0. Oxygen saturation remained february 2018 to november 2018 scheduled in our center to laser ablation of the above 98% all the time. Anesthetic technique and any maternal or Discussion: As far as we have found in literature, this is the frst case that describes fetal complications were recorded. Conclusion: these fetal procedures can range from minimal invasive punctions to full open fetal surgery. Providing anesthesia for these procedures is a challenge, 1 2 2 2 2 where care has to be taken for both mother and fetus. Close monitoring is necessary to detect and treat possible complications and to confrm phaechromocytoma in pregnancy the uneventful development of the underlying pregnancy. In follow-up for consultation of high-risk obstetrics, she maintains treatment with aspirin. Cardiology reported no contraindication for a vaginal Background: the incidence of phaechromocytoma in pregnancy is < 0. If left undiagnosed can lead to up to 30% maternal and1 delivery, although recommended avoiding a prolonged 2? Patients presenting for surgery during pregnancy pose a signifcant ventricular function were explained challenge to the anaesthetist. Patients must undergo a multidisciplinary evaluation, where the abdominal mass on routine health screening ultrasound. C-section increases the rate of was confrmed with elevated urine catecholamines at 14 weeks gestation. She hemorrhage, infection and thromboembolism, which increase myocardial ischemia. A rapid sequence induction using propofol, It is important to keep the patient stable, avoiding any stress or any situation which fentanyl and rocuronium was carried out. Measures that reduce postpartum hemorrhage uptrended to 145/77mmHg during tumour manipulation with episodes of ventricular are recommended, avoiding ergometrine due to the possibility of producing bigeminy. Pre-ligation fuid loading was guided by Flotrac readings using stroke coronary spasm. No inotropic support was required post tumour removal, Obstetric Anaesthesiology 109 and she was extubated uneventfully. Discussion: A combination of blood loss, anaesthetic related vasodilation and Anesthesia management in a pregnant patient with contracted plasma volume all contribute to exaggerated hypotension post tumour oropharynx hemangioma: case report ligation2 Large volume intravascular expansion prior to ligation can mitigate this. Pheochromocytoma and pregnancy: a and Reanimation Clinic Istanbul (Turkey), Ege University Faculty case report and review of anesthetic management. Background: Hemangiomas are benign vascular tumors that are composed of blood Learning points: Early diagnosis, adequate preoperative medical optimization, vessels with non-atypia endothelial cells. Oral cavity hemangiomas are observed multidisciplinary planning and meticulous intraoperative haemodynamic less than 1% (1). In this case report, we aimed to present our clinical experience management are all essential in ensuring a good outcome in this rare but dreaded regarding spinal anesthesia applied to patient with oral cavity hemangioma which condition. We fnd the Flotrac to be a good alternative and less invasive form of narrowed the oropharynx with uvula, soft palate, and intramuscular extension, for haemodynamic monitoring for such cases. For spinal anesthesia, 10 mg bupivacaine Heavy was injected by 25 G spinal syringe in the range of L -L spinal,4 5 woman with unruptured intracranial aneurysm the operation was performed. There are still no recommendations1 available for the anesthetic management, due to the scarcity of literature. Case Report: 38 weeks pregnant, 35 years old, 2G1P, proposed to elective caesarian. History of right posterior cerebral artery aneurysm, submitted to coil embolization 5 years before the pregnancy, asymptomatic. Epidural anesthesia was realized (L3-L4 median approach, with a 18G Tuohy needle and epidural space search with saline solution). There were no intercurrences during peri-operatory period, patient remained hemodynamically stable, with no neurological defcits. There1 is a lack of experimental or clinical data to confrm or disprove general or regional anesthesia in this context. Due to physiological changes of pregnancy, general anesthesia may be associated with more complications than regional anesthesia. Laryngoscopy and tracheal intubation are interventions which cause a signifcant rise in aneurysm transmural pressure, related to a risk of rupture of 0. Epidural anesthesia is a safe technique, if unintentional dural puncture does not occur (abrupt and intense intracranial pressure fall). In this case, the procedure was realized by an experienced anesthesiologist and underwent with no intercurrences. Epidural anesthesia was safe and effective, allowing a stable hemodynamic profle, good post-operatory analgesia and the possibility of early Discussion: Due to multinodular goiter, Y? Learning points: Anesthesia for elective caesarian in pregnant woman with References: intracranial aneurysm requires a multidisciplinary approach. Cavernous hemangioma of the uvula: report a rare case with should be adapted to the patient clinical status and anesthesiologist?s experience. Learning points: In our case with oropharynx hemangioma, because of the presence of rare soft palate and uvula, general anesthesia method was considered as high risk for the patient by considering all airway complications that may develop, especially bleeding, and the patient safety was provided by spinal anesthesia. Hypermagnesemia-Induced Cardiopulmonary Arrest Before Induction of Anesthesia for Emergency Cesarean Section. Learning points: Magnesium sulfate should be used with precaution in preeclamptic anaesthesia in Austria patients with renal failure. The secondary aim was to compare the 1Shupyk National Medical Academy of Postgraduate Education Kyiv anaesthesia practices with the current guidelines published by the American (Ukraine), 2Heart Institute ?inistry of Health of Ukraine, Shupyk Society of Anesthesiologists 2016 and by the Association of Anaesthetists of Great Britain and Ireland in 2013. Descriptive statistics and bivariate correlations were carried out a frequency of 3 to 10 cases per 100,000 childbirth. Epidural hospitalized with complains of severe compressive pain in the cardiac area with analgesia was offered universally, with a rate < 30% in 56 (86%) responding irradiation to the left arm and feeling of heaviness in the chest. At the acting intrathecal morphine and 18 (28%) respondents did not routinely administer hospitalization, fbrillation of the ventricles was recorded and resuscitation measures any intrathecal opioid. Wound infltration for acute postoperative pain control with cardioversion were performed. The results of the urgent coronary angiography was practiced in 2 (3%) responding units. Clopidogrel had been this suggests that the analgesic therapy with nalbuphine appears effcient, making cancelled 5 days before delivery. An epidural rate > 20% correlated signifcantly with the a healthy child by caesarean section under epidural anesthesia. Undiscovered coagulopathies are a [1] European Society of Cardiologists recommends coronary angioplasty as the possible reason for this fnding. In this case, the appointment of dual antiplatelet therapy for 4 weeks is Conclusions: this survey reveals that obstetric anaesthesia practices in Austria recommended.
Purchase bimat in india
This consideration has been incorporated into proposed intervention algorithms medicine bg purchase cheap bimat, such as those proposed by Botto et al. There is also variation in the choice of stroke risk schema 3,21,23,24 and in the selection and interpretation of data on the stroke risk associated with individual components of overall stroke risk. These definitions were largely determined by the information in the databases from which the various risk prediction schemas were derived. It is not clear whether the evolved definition had been further 3 validated,21 although ejection fraction has not been shown to predict stroke events in heart failure patients. Although the definition of age does not vary among the schemas, the reliability of the values assigned depends on the rigour of the applicable derivation and validation cohorts. The inconsistent definition of previous stroke has the potential to contribute substantially to variability among the risk schemas. However, they might be important in the calculation of the annual stroke risk, and to influence specific anticoagulation recommendations for patients at relatively low risk of stroke (0. Definitions of stroke risk factors in the Canadian Cardiovascular Society Atrial Fibrillation Guidelines update Factor Definition Congestive Heart Failure Documented moderate to severe systolic dysfunction; signs and symptoms of heart failure with reduced ejection fraction; or recent decompensated heart failure that required hospitalization irrespective of ejection fraction Hypertension Resting blood pressure > 140 mm Hg systolic and/or > 90 mm Hg diastolic on at least 2 occasions or current antihypertensive pharmacological treatment Age 65 Age? Acetylsalicylic acid was recommended for patients with vascular disease as the only risk factor. No antithrombotic therapy was recommended for patients with none of these criteria. It was postulated that thrombin generation triggered by exposure of blood to the artificial surface of the valve might have overwhelmed the local effects of dabigatran. In the preanticoagulant era it was estimated that 22% of patients with rheumatic mitral stenosis died from thromboembolic complications. The presence of a bioprosthetic heart valve or a history of valve repair is not an indication for long-term anticoagulation in the absence of other risk factors. The favourable profile of apixaban vs warfarin was preserved with respect to the primary efficacy outcome of stroke or systemic thromboembolism and with respect to the primary safety outcome of major bleeding. The serum concentration of creatinine, a by-product of the metabolism of creatine and phosphocreatine in skeletal muscle is, in steady state, a fairly reliable indicator of kidney function. Unfortunately, the use of serum creatinine level is limited by its indirect relationship to glomerular filtration. The production of serum creatinine is proportional to muscle mass (which is modified by factors such as sex, age, muscle mass, race, and nutrition), and the clearance of creatinine is influenced not only by glomerular filtration (ie, renal function) but also factors that influence the active secretion of creatinine in the proximal tubule (such as drugs like amiodarone and dronedarone). Multiple formulae have been developed to correct for creatinine production (ie, muscle mass), and provide a more accurate estimate of overall renal function. However, it is important to remember that altered glomerular filtration is not the only factor that can affect drug clearance in the presence of renal dysfunction. Changes in tubular function, and the volume of distribution, albumin concentration, and organic acid accumulation might all influence the risk of drug toxicity. First, it was derived in a limited number of patients (249; 96% male) in 1976 using nonstandardized creatinine assays. The introduction of standardized creatinine assays has resulted in a decline in the measured creatinine level. Although the original creatinine assay is no longer available for direct comparison, it is estimated that the use of values from standardized creatinine assays causes the Cockcroft-Gault formula to overestimate renal function by approximately 5%. However, despite the improved accuracy and precision of these newer equations, drug manufacturers have typically used the older Cockcroft-Gault eCrCl method when recommending medication dosage adjustments for patients with renal dysfunction. Renal function, hemoglobin, and hepatic function should be assessed on an annual basis for stable patients with preserved renal function. In addition, renal function should be monitored during the course of any intercurrent illness that might affect volume or renal status (eg, gastroenteritis, influenza, after surgery); or with the initiation of medications that have the potential to affect renal function (eg, angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, mineralocorticoid receptor antagonists, or nonsteroidal anti-inflammatory drug therapy). Specifically, up to 80% of circulating dabigatran, 33% of rivaroxaban, and 25% of apixaban is excreted renally, which results in differential accumulation in the drug concentration. Of those, 1474 were randomized to rivaroxaban 15 mg daily and the remainder were randomized to warfarin. Subgroup analyses did not demonstrate any difference in efficacy or safety outcomes between those with preserved renal function (eCrCl > 50 mL/min) who received the higher rivaroxaban dose (20 mg daily), and those with moderate renal impairment who received the lower rivaroxaban dose (15 mg daily). If 2 of the 3 criteria were met, the dosage of apixaban was reduced from 5 mg bid to 2. Most patients with moderate renal impairment (eCrCl 30-50 mL/min) continued to receive the higher (5 mg bid; 1063 patients) rather than the lower dose (2. Apixaban was superior to warfarin in reducing stroke or systemic embolism, major bleeding, and mortality irrespective of kidney function. Patients with moderate renal impairment (eCrCl of 30-50 mL/min) could be randomized to either dabigatran 110 mg bid or dabigatran 150 mg bid. European and American dosing recommendations state that apixaban and rivaroxaban can be administered to patients with an eCrCl > 15 mL/min. However, the evidence for this recommendation comes from pharmacokinetic studies in a limited number of patients. Focused 2012 update of the Canadian Cardiovascular Society atrial fibrillation guidelines: recommendations for stroke prevention and rate/rhythm control. Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Presence and duration of atrial fibrillation detected by continuous monitoring: crucial implications for the risk of thromboembolic events. Atrial fibrillation patients categorized as ?not for anticoagulation according to the 2014 Canadian Cardiovascular Society algorithm are not ?low risk?. The new Canadian Cardiovascular Society algorithm for antithrombotic therapy of atrial fibrillation is appropriately based on current epidemiologic data. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke: the Framingham study. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials [erratum in 1994;154:2254]. Validation of clinical classification schemes for predicting stroke: results from the national registry of atrial fibrillation. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on Atrial Fibrillation. Identifying patients at high risk for stroke despite anticoagulation: a comparison of contemporary stroke risk stratification schemes in an anticoagulated atrial fibrillation cohort. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. Antithrombotic therapy for atrial fibrillation: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidencebased clinical practice guidelines. Ejection fraction and outcomes in patients with atrial fibrillation and heart failure: the Loire Valley Atrial Fibrillation Project. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation Cohort study. Prophylaxis of recurrent embolism of intracardiac origin; protracted anticoagulant therapy on an ambulatory basis. Thromboembolism associated with auricular fibrillation; continuous anticoagulant therapy. Outcomes among valvular heart disease patients experiencing ischemic stroke or transient ischemic attack in Olmsted county, Minnesota. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Late incidence and determinants of stroke after aortic and mitral valve replacement. Risk of stroke in a cohort of 815 patients with calcification of the aortic valve with or without stenosis. Mitral regurgitation reduces the risk of stroke in patients with nonrheumatic atrial fibrillation. A comparative analysis between the porcine xenograft valve and Ionescu-Shiley bovine pericardial valve.
Cheap 3ml bimat mastercard
The field supports are intended to complement the quality improvement processes currently underway in your organization medications elderly should not take bimat 3 ml amex. Cancer Care Ontario has an advisory role to the Ministry of Health and Long-Term Care (referred to as ?the ministry?) pertaining to cancer and renal related matters. This will include reviewing the overall use of anesthesia for procedures, and the associated staffing complement. Procedures that are not gastrointestinal in nature are out of scope; this includes procedures related to the bladder, lungs, urethra, prostate and kidneys that may occur in the endoscopy suite. Stakeholders will be kept apprised of any changes to data submission requirements as they occur. Table 6 reflects membership of the Quality Management Partnership Colonoscopy / Endoscopy Expert Advisory Panel. Jill Tinmouth Lead Scientist, ColonCancerCheck Jul 2013 Present Clinical Lead, Quality Management Dr. Scott Shulman North East Oct 2014 Present Dr Lawrence Hookey South East Oct 2014 Present Dr. Naoki Chiba Waterloo Wellington Oct 2014 May 2015 Clinicians and Hospital Administrators Dr. Michael?s Hospital College of Physician and Surgeons of Ontario Wade Hillier Director at College of Physicians and Jul 2013 Present Surgeons of Ontario Regional Cancer Programs Tom McHugh Regional Vice President, Central East Jul 2013 Present Brenda Fleming Director, Southwest Oct 2014 Present 49 Jeff Booth Director, Erie St Clair Oct 2014 Dec 2014 Elizabeth Dulmage Director, Erie St. Nancy Policy Management and Evaluation, University of Apr 2013 Dec Baxter Toronto 2014. Staff Surgeon and Division Chief, Department of Surgery, Division of General Surgery, St. Quality Management Partnership Colonoscopy Apr 2013 Dec Morgan Clinical Lead (Chair) 2014. Professor, Division of Gastroenterology, Department of Medicine at McMaster University. Each index category is mutually exclusive and a given patient experience will be aligned to only one index category. Each index category has a specific weighted unit reflecting the cost of the procedures within the category. Some index categories can be paired with additional pricing adjustments for interventions. Adjunct procedures that are added to colonoscopy or gastroscopy index category procedures resulting in additional funding. Interventions can also be added to remaining index category procedures, however will not impact the funding rate the following table outlines the Index Category procedures and Interventions and the associated weighted unit/funding rate. Gastroscopy following a positive fecal occult blood test and negative colonoscopy. Canadian Association of Gastroenterology consensus guidelines on safety and quality indicators in endoscopy. The effect of surgical experience on results of esophagectomy for esophageal carcinoma. Analysis of administrative data finds endoscopist quality measures associated with postcolonoscopy colorectal cancer. Bleeding and perforation after outpatient colonoscopy and their risk factors in usual clinical practice. Fujiflm is constantly elaborating new opportunities to provide top quality products, At Fujiflm we are constantly innovating and creating excellent services and highly customised new solutions that address the practical needs of our business solutions in the world of endoscopy. This ensures that we not only meet the the focus at Fujiflm is frmly on holistic patient care highest quality requirements but also contribute which means that our service portfolio includes to the advancement of culture, science, industry expert technical assistance, a comprehensive range and technology as well as improved health and of hygiene products and individual consulting. At Fujiflm we are continuously developing new technologies, products and services that inspire and excite people everywhere and ofer the potential to expand the horizons of tomorrow?s businesses and Today Fujiflm operates in around 55 group lifestyles. One example is the combination of specialised applications, such as double balloon endoscopy and endoscopic ultrasound, in one complete system which would enable you to streamline your workfow. In addition, the continuous enhancement of imaging technologies ensures high precision and excellent quality. Our overarching aim is to help to improve the quality of life of people worldwide through the early detection and successful treatment of disease. Fujiflm?s renowned ColoAssist has been optimised for the 700 series colonoscopes and now includes the Flexibility Adjuster for easier insertion in addition to advanced force transmission and adaptive bending. In addition, Smart Bend the smart bending ability and the small bending radius make treatment of difcult-to-reach lesions easier. The procedure digitally selects three wavelengths of light and displays reconstructed images. Focussing on the characteristics of short wavelength absorption of haemoglobin (at 410 nm) combined with specifc white light spectral colours results in improved and accurate contrast imaging. The procedure digitally selects three wavelengths of the light and displays the reconstructed images. It features the Flexibility Adjuster with diferent levels of stifness as well as innovative Advanced Force Transmission and Adaptive Bending for improved manoeuvrability and more patient comfort. This is helpful when soft inserting the scope into segments such as the sigmoid colon and the transverse stif colon where the endoscope can more smoothly follow the intestinal tract. The fexible bending section has been designed to return more easily to its straight form after passing through the tight curves of the colon. The new design helps to simplify the cleaning process and also reduces the potential for accidental damage. The G7 grip is designed to have an easy and comfortable feel that optimises performance and minimises stress during clinical procedures. During transmission, the digital signal is much less afected by noise from outside, enabling advanced observation and diagnosis. The focus at the edges of an image has been improved, minimising distortion in observation of a lumen. It has a small bending radius and similar functionality to the routine gastroscope including all features. This allows the endoscope to approach the targeted observation point and lesion Observation point Observation point more easily and with less efort. The slim distal end also supports a soft transnasal insertion and reduces patient discomfort. Like the routine scope, it features the full range of functionalities including fexible adjustment even with the slim diameter of 11. Even areas that are hard to observe, such as 170 the reverse side of folds, can be visualised more easily. It is especially suitable for more challenging anatomies and paediatric use, where it can be applied in cases of stenosis, severe infammation, or anatomical adhesion. Lesions which are difcult to reach can be easily treated due to the smart bending ability as well as the small bending radius. The unique specifcations include ultraslim and smart bending types as well as the double balloon system. In addition, the specially designed round shaped forceps elevator reduces the risk of guidewire damage. The inner tube of the instrument channels uses an optimised material to enable a device to be inserted smoothly, supporting rapid device exchange. The two-balloon system is revolutionary, providing an unparalleled level of detail and is, to this day, the gold standard in examination of the small intestine. It enables blood or mucus to be aspirated while a therapeutic device is inserted, making hemostasis quicker. The large working channel is also designed for easier insertion and removal of a balloon catheter before and after dilation of stricture. Also, a onetouch type connector especially designed for the balloon air feed inlet on the endoscope is provided, making the preparation simpler. A water jet function is also incorporated for use in various treatment methods during endoscopy. Thanks to the anti-blur function, all captured images are documented in razor-sharp detail. During the archiving stage, the video processor automatically selects and saves the cleanest image.
Buy bimat on line amex
Initial fitting should include a can be used to assist application and Ensure style is appropriate demonstration of how to put on and remove minimise damage medications 1 gram best bimat 3 ml. Clear Garments should be replaced every three silicone coated band at top verbal and written instructions should be to six months, or when they begin to lose edges given on errors of fit that may be discovered elasticity. Young or very active patients fixation mechanism eg after first wearing, and on how to care for may require more frequent garment waist fastening/half the garment (Box 33). Allergens include Garment application this can be assisted by wearing household fabric dye, latex and nylon. If an allergy is gloves rubber gloves whilst smoothing the garment suspected: Glide on applicator Emollients may damage compression treat contact dermatitis appropriately Silk slippers garments. Ensure emollient is absorbed use garments without latex Anti-slip mat before donning garment or use products use garments with high cotton content, Metal applicator frames approved by the garment manufacturer. However, the finer finish of check that the patient is concordant with circular knit hosiery may make it more garment wear, that the garment has not cosmetically acceptable. A variety of aids is Tolerability of high levels of compression available for easing application of may be enhanced by layering garments. Layering compression garments additional garment layer can help to the practice of layering compression manage exacerbations of their condition. Two layers of garment may be able to manage to apply garment produce a higher pressure on the two layers of a lower compression garment. The When layering two garments, it is second layer is likely to add about 70% of recommended that a flat knit garment is the pressure it would when applied alone75. Risk reduction Patients should be advised to wear compression garments when performing high risk, repetitive activities. Although there is no robust evidence that long sitting while travelling, eg by aeroplane, increases or precipitates lymphoedema, patients should exercise caution and wear a compression garment if they are at risk of or have lymphoedema. These garments applies can be adjusted by altering how may be custom made or ready to wear. They can be used to classified as providing medium contain swelling in patients with moderate compression (25-30mmHg), while lower or severe lymphoedema of the upper or pressures are used on the head. However, lower limb and the torso, and are useful self there is no recognised agreement on the management tools. Leotard or bodice style garments may be useful for patients with truncal oedema and flat knit construction is preferable. Anatomically contoured foam padding inserted into compression pantyhose or shorts can be used in female genital lymphoedema. Groin swelling is often accompanied by tissue thickening, and may occur in combination with lower limb lymphoedema; oneor twolegged closed gusset pantyhose angled across the groin with foam chip stasis pads may be helpful. Gentle resistance exercise stimulates muscle pumps Types of exercise: and increases lymph flow; aerobic exercise start with low to moderate intensity exercise increases intra-abdominal pressure, which paralysed limbs can be moved passively 76 walking, swimming, cycling and low impact aerobics are recommended facilitates pumping of the thoracic duct. Patients should be encouraged not for patients who have difficulty with mobility, to sleep in a chair and to go to bed at night to joint function or joint movement. It is thought that elevation acts by maximising venous drainage and by decreasing capillary pressure and lymph production. Patient has: Poor concordance Depression Loneliness and isolation Poor coping with treatment According to severity of. Assess why depression consider48: Improve communication Access patient support Provide patient. Patients with advanced disease may not be able to tolerate a full programme of assessment are modified and individual treatments are and treatment, but require a palliative selected to ease specific symptoms (Box 37 approach in which assessment techniques and Table 9). Lymphatic grafting and lymph Removal of redundant tissue after successful Patients for surgery need to be selected node transplantation require microsurgical conservative therapy carefully (Box 38) and counselled to ensure techniques, and show promising results in Proximal lymphatic realistic expectations of likely outcome. However, the patients with long-standing breast cancer Lymphangiosarcoma postsurgical morbidity of reduction related lymphoedema. In tissue and is considered only if the limb has some cases, surgical reduction may be not responded to standard conservative considered for lymphoedema of the eyelid therapy. Liposuction has also been Megalymphatics: large, dilated incompetent lymph vessels that anastomoses and lymphatic or venous used for primary and secondary leg allow lymphatic reflux vessel grafting, or lymph node transplantlymphoedema with promising results91. Other treatments A variety of other treatment modalities may Benzopyrones be used to treat lymphoedema; many Benzopyrones are based on a variety of require further evaluation (Box 39). Two main groups of drug have been used in There is little evidence to support the use the treatment of lymphoedema: of these drugs in lymphoedema1,95. It involves the Other treatments that have been used for the treatment to draw conclusions about their efficacy in application of narrow strips of elastic tape to of lymphoedema, mainly in lymphoedema. The same conclusion has the affected area, and can be used in breast cancer patients, that been reached about flavonoids. Coumarin combination with compression garments or all require further evaluation, has been most widely trialled, but the most bandaging. It is thought to improve muscle include: recent study reported no significant effect95 function and lymph flow98 and may have a cryotherapy and the drug has been withdrawn in role to play in the treatment of midline and transcutaneous electrical Australia because of liver toxicity. However, improve lymph flow and reduce limb volume higher doses of thiazides or loop diuretics in the short-term99,100. Further research is (eg furosemide or bumetanide) can reduce required to establish whether benefits can be body potassium levels with long-term use demonstrated in randomised trials and in the and may cause muscle weakness, promote long-term. Occasionally, Low level laser therapy has shown potential short courses may be of benefit in chronic for the treatment of lymphoedema, oedema of mixed aetiology, and in older particularly of the upper limb, where it has patients in whom enhanced lymphatic reduced limb volume and tissue hardness101. Benzo-pyrones for reducing that may help to clear the central and controlling lymphoedema of the limbs. Antibiotics/antiin humans to confirm that variations in inflammatories for reducing acute inflammatory episodes in lymphoedema of the limbs. Focus demonstrated that a combination of exercise Document: Lymphoedema bandaging in practice. Position volume of lymphoedematous limbs79, Document: Understanding compression therapy. Template for Practice: compression hosiery in and may be proven beneficial in some groups lymphoedema. Clinical use of inflammatories for reducing acute inflammatory episodes in indirect lymphography in different forms of the leg edema. Lymphology1998; development methods, and their use in clinical guideline 31(3): 119-27. Lymphoedema diagnose lymphoedema amongst breast cancer survivors: 6Framework Journal2003; 1: 10-18. Managing leg ulcers: a review of clinical Effect of conservative treatment on pain in lymphoedema. J Med Genet of best practice:Minimising pain at wound dressing-related 1985; 22(4): 274-78. Int J Low Extrem Wounds sentinel lymph node biopsy versus axillary lymph node dissection 2002; 1(3): 202-8. Lymphoedema after treatment of breast evaluation, and treatment of overweight and obesity in adults. Brussels, Belgium: of lower limb lymphoedema following treatment for International Diabetes Federation; 2005. In: European Wound Management Association and deep breathing on secondary arm lymphedema. Microsurgical techniques for lymphedema lymph drainage to compression therapy for breast cancer related treatment: derivative lymphatic-venous microsurgery. Eur J Nucl Med Mol Imaging2003; 30(2): of a new, more simplified physiotherapy technique for lymphatic 202-6. In: Twycross R, Jenns K, lymphedema: long-term results following microsurgical lymph node Todd J (eds). Diagnosis and management of randomised, prospective study of a role of adjunctive pneumatic primary chylous ascites. The risk of genital edema after women with lymphedema after treatment for breast cancer. Eur J Clin parallel-group clinical trial comparing multilayer bandaging Pharmacol1977; 11(6): 435-38. Cancer2000; 88(12): management in resource-poor settings relevance for lymphatic 2832-37. Practical guidance on lymphoedema trial of hyperbaric oxygen therapy in patients with chronic arm bandaging of the upper and lower limbs.
Laminaria. Bimat.
- Are there safety concerns?
- Dosing considerations for Laminaria.
- What is Laminaria?
- Preparation ("ripening") of the cervix in women, such as during childbirth or procedures.
- Are there any interactions with medications?
- How does Laminaria work?
- Weight loss, high blood pressure, cancer prevention, heartburn, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96544

Purchase bimat amex
Pei Y 7r medications discount 3ml bimat mastercard, Cattran D, Greenwood C: Predicting chronic renal insufficiency in idiopathic membranous glomerulonephritis. Hannedouche T, Albouze G, Chauveau P, Lacour B, Jungers P: Effects of blood pressure and antihypertensivetreatmentonprogressionofadvancedchronicrenalfailure. Ruggenenti P, Perna A, Zoccali C, Gherardi G, Benini R, Testa A, Remuzzi G: Chronic proteinuric nephropathies. Hannedouche T, Chauveau P, Kalou F, Albouze G, Lacour B, Jungers P: Factors affecting progression in advanced chronic renal failure. Nakano S, Ogihara M, Tamura C, Kitazawa M, Nishizawa M, Kigoshi T, Uchida K: Reversed circadian blood pressure rhythm independently predicts endstage renal failure in non-insulin-dependent diabetes mellitus subjects. Toth T, Takebayashi S: Factors contributing to the outcome in 100 adult patients with idiopathic membranous glomerulonephritis. Ravid M, Brosh D, Ravid-Safran D, Levy Z, Rachmani R: Main risk factors for nephropathy in type 2 diabetes mellitus are plasma cholesterol levels, mean blood pressure, and hyperglycemia. Locatelli F, Alberti D, Graziani G, Buccianti G, Redaelli B, Giangrande A: Prospective, randomised, multicentre trial of effect of protein restriction on progression of chronic renal insufficiency. Standards of Medical Care for Patients with Diabetes Mellitus, Position Statement. The Diabetes Control and Complications Trial Research Group: the effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. Microalbuminuria Collaborative Study Group, United Kingdom: Intensive therapy and progression to clinical albuminuria in patients with insulin dependent diabetes mellitus and microalbuminuria. Ohkubo Y, Kishikawa H, Araki E, Miyata T, Isami S, Motoyoshi S, Kojima Y, Furuyoshi N, Shichiri M: Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: A randomized prospective 6-year study. National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents: Update on the 1987 Task Force Report on High Blood Pressure in Children and Adolescents: A working group report from the National High Blood Pressure Education Program. Randomised trial of old and new antihypertensive drugs in elderly patients: Cardiovascular Mortality and Mrobidity in the Swedish Trial in Old Patients with Hypertension-2 Study. Ruggenenti P, Remuzzi G: Angiotensin-converting enzyme inhibitor therapy for nondiabetic progressive renal diseas. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. Yusuf S, Sleigh P, Pogue J, Bosch J, Davies R, Dagenais G: Effects of an angiotensin-convertingenzymeinhibitor,ramipril,oncardiovasculareventsinhigh-riskpatients. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: A randomized controlled trial. Manttari M, Tiula E, Alikoski T, Manninen V: Effects of hypertension and dyslipidemia on the decline? Tonolo G, Ciccarese M, Brizzi P, Puddu L, Secchi G, Calvia P: Reduction of albumin excretion rate in normotensive microalbumiuric type 2 diabetic pateints during long-term simvastatin treatment. Buemi M, Allegra A, Corica F, Aloisi C, Giacobbe M, Pettinato G: Effect of fluvastatin on proteinuria in patients with immunoglobulin A nephropathy. Albertazzi A, Di Liberato L, Daniele F, Battistel V, Colombi L: Efficacy and tolerability of recombinant humanerythropoietintreatmentinpre-dialysispatients:Resultsofamulticenterstudy. Perna A, Remuzzi G: Abnormal permeability to proteins and glomerular lesions: A meta-analysis of experimental and human studies. Decker T, Kofoed-Enevoldsen A, Norgaard K,Borch-Johnsen K, Feldt-Rasmussen B, Jensen T: Microalbuminuria:Implications formicroand macrovasculardisease. Jensen T, Borch-Johnsen K, Kofoed-Enevoldsen A, Deckert T: Coronary heart disease in young type 1 (insulin-dependent) diabetic patients with and without diabetic nephropathy: Incidence and risk factors. McKenna K, Thompson C: Microalbuminuria: A marker to increased renal and cardiovascular risk in diabetes mellitus. National High Blood Pressure Education Program Working Group Report on Hypertension in Diabetes. Consensus development conference on the diagnosis of coronary heart disease in people with diabetes. American Optometric Association Consensus Panel on Diabetes: Care of the Patient With Diabetes Mellitus (ed 2). Proceedings of a consensus development conference on standardized measures in diabetic neuropathy. Morbidity and Mortality: 1998 Chartbook on Cardiovascular, Lung, and Blood Diseases. Schillaci G, Reboldi G, Verdecchia P: High-normal serum creatinine concentration is a predictor of cardiovascular risk in essential hypertension. Ljungman S, Wikstrand J, Hartford M, Berglund G: Urinary albumin excretion?A predictor of risk of cardiovascular disease. A prospective 10-year follow-up of middle-aged nondiabetic normal and hypertensive men. Agewall S, Wikstrand J, Ljungman S, Fagerberg B: Usefulness of microalbuminuria in predicting cardiovascular mortality in treated hypertensive men with and without diabetes mellitus. Plan and operation of the third national health and nutrition examination survey, 1988?1994. Ezzati T, Wakesberg J, Chu A: Sample design: Third national health and nutrition examination survey, 1988?1994. Coresh J, Astor B, McQuillan G: Calibration and random variation of the serum creatinine assay as critical elements of using equations to estimate glomerular filtration rate. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Published 2010 Cover design: Dorcas Gelabert Breathing in America: Diseases, Progress, and Hope Edited by Dean E. Kiley, PhD Professor of Medicine Director of the Division of Lung Diseases Tufts University School of Medicine National Heart, Lung, and Blood Institute Chief, Division of Pulmonary, Critical Care and Sleep Medicine Landon S. Professor of Medicine (Emeritus) Columbia University College of Physicians & Surgeons viii Foreword Respiratory issues affect millions of Americans, robbing them of their health, happiness, and even of life itself. Moreover, tobacco smoke kills more Americans in one year than all the wars our nation fought during the last century. Congress has recognized the importance of respiratory health and has embarked on programs to make a difference. We have strengthened the Centers for Disease Control and Prevention, granted the Food and Drug Administration the ability to regulate tobacco, improved pollution control through the Environmental Protection Agency, and funded tuberculosis programs throughout the world because we realize that in order to control tuberculosis at home, we need to control it worldwide. Americans are living longer and healthier and, for the most part, breathing easier. Some previously untreatable diseases, such as respiratory distress of the newborn?once a leading cause of infant mortality?now have treatments; others have cures within their grasp. Research is essential for the United States to remain a world leader in the development of health advances. Research improves our nation?s productivity, increases employment, and improves the? More progress must be made, both in understanding disease processes in order to develop cures and in bringing these advances to everyone. I congratulate the American Thoracic Society on this book, which highlights many of the advances that recent research has brought about and demonstrates the value of working together to improve the lung health of Americans. Mike Crapo United State Senator, Idaho ix Preface Breathing in America: Diseases, Progress, and Hope brie? It describes who is vulnerable to developing these diseases, what it is like to have them, and their burden on society. And, most importantly, it explains where we are in understanding the disease processes, how close research is to developing new tests and treatments, and what still needs to be done. Nearly a decade ago, the European Respiratory Society sought to identify variations in lung diseases across different European nations. In 2003, it published the European Lung White Book, a report that helped to increase awareness of the high toll of lung diseases. The Forum for International Respiratory Societies, which is composed of organizations including the American Thoracic Society, the European Respiratory Society, the Asociacion Latinoamericana del Torax, the American College of Chest Physicians, the Asian Paci? The American Thoracic Society agreed to undertake this project for the United States. The American Thoracic Society frequently receives inquiries from the media, patients, and the public at large regarding speci? To address these inquiries, staff members thought that a short review of respiratory diseases would be helpful. There have long been advocates within the American Thoracic Society for a publication that covered the topics now found in Breathing in America: Diseases, Progress, and Hope.
Effective bimat 3ml
Already after two months of observation medicine qhs order bimat 3 ml with mastercard, patients) induction of anesthesia: dexmedetomidine 0. The placebo group rats continued to show signifcant depressive comparable by sex, age, initial blood pressure, initial heart rate, position on the behavior compared with sham operated rats. Treatment with pyruvate also led to operating table and localization of the brain tumor. A rapid axonal stretch injury triggers secondary Kocaeli (Turkey) axonal changes that can vary in extent and severity. Within hours to days after the primary injury, biochemical changes will lead to the loss of axonal function. The Background and Goal of Study: Propofol can act as a pro or anticonvulsant most vulnerable areas are the brainstem, thalamus, parasagittal white matter of the agent in a dose-depended fashion. Propofol at higher doses act as anticonvulsant, cerebral cortex, and corpus callosum. However, this rise can be much more pronounced useful tool for better understanding of the pathophysiology and development of with larger doses of propofol. The objective of the present study was to develop a simple different dose regimens of propofol (low dose: <1mg/kg, high dose: >1mg/kg) on reproducible, reliable model that will cause widespread white matter damage the duration of the seizures, the required energy for the seizures, and the seizure without additional skull fractions and contusions. Patients were evaluated in two rotation device was used to turn the head rapidly from 0 to 90 in the coronal plane. Conclusions: Higher doses of propofol in induction of anesthesia can lead to a Comparing the effect between continuous more progressive rise in seizure threshold over the course of electroconvulsive infusion and intermittent bolus of rocuronium for therapy than lower doses of propofol. Results and Discussion: the incidence of involuntary movement and spontaneous repiration were measured as signifcantly lower in group I (5. Intraoperative dexmedetomidine 1Benisuef University Hospital Benisuef (Egypt) infusion rate and incidence of perioperative complication was analysed based on anaesthetic charts and surgical dictations. Effective, evidenceapproved by Institutional Review Board (2016114) and written parental consent was based prevention strategies for its occurrence are not currently described. Patients were for ependymoma and 2 for medulloblastoma) were managed with intravenous randomly assigned into one of two groups; the frst group received conventional dexmedetomidine. The mean irradiation time and sedation time was 118 46 general anaesthesia only (40 participants) (conventional anaesthesia group) minutes and 270 66 minutes, respectively. All patients received supplemental and the second group received conventional general anaesthesia with extra oxygen through nasal cannula. No patients required emergency invasive airway administration of intraoperative magnesium sulphate 30 mg/kg as loading dose over management. Intravenous sedation was commenced with loading dose of 10 minutes then maintenance dose 10 mg/kg/hour (40 participants) (Mg sulphate dexmedetomidine (6 ?g/kg for 10 minutes) and boluses of ketamine and fentanyl. Cognitive assessment for both groups was done preoperative and 1 week Dexmedetomidine infusion rate was subsequently changed between 0. The primary outcome was the incidence of Train-of-Four stenosis or occlusion between May 2003 and August 2017 was performed. In univariable logistic regression, gender, rocuronium overdose, Results and Discussion: A total of 211 cases were suitable for analysis (lower=65, and T1 appearance time showed statistical signifcance. T1 1Kansai Medical University Hirakata city (Japan), 2Center for appearance time also may be helpful to predict residual blockade in clinical practice. We defned these 3 levels of sedation as ?deep?, ?moderate?, and ?light?, propofol effect site concentration and the measured respectively. In reality, various issues corrupt time-independency leading during between ?deep and ?moderate?. This can result in conficting information ?moderate and ?light level was observed in 7 participants. Pumps were programmed with spindle wave indicated that moderate to light sedation by midazolam might induce Schnider model for propofol and Minto model for remifentanil. Adding a lag term improved the Materials and Methods: Retrospective review between 2010 and 2018. Anaesthesiological parameters were analysed, blood Airway Attenuates Systemic and Cerebral Hemodynamic Response loss and blood transfusion rate were measured. Conclusions: the results obtained in our institution resemble the published data1. Factors Related to Blood Loss During Fronto-Orbital perioperative complications was evaluated. In 15 (19%) patients time trial including 50 adult patients who underwent elective craniotomy. There was a trend of shorter intensive care unit stay in group, respectively (P=0. To do so, blood pressure Anaesthesiology Groningen (Netherlands) is lowered below the lower autoregulation limit. We hypothesized that controlled hypotension does not impair the outcome of the patients. At the surgeon?s request, estimate baseline levels of biomarkers of neuropsychiatric diseases. In 2017 controlled hypotension was performed whenever hemostasis proved to be diffcult. The purpose of the current abstract is to describe the initial a hypotension group (n=28; mean age 35?12 years) and a control group (n=28; technical and laboratory fndings. Groups were comparable with respect to age, gender, and Materials and Methods: All patients? However the hypotension group showed a signifcantly anaesthesia are invited to participate. Patient characteristics, medical hypotension group there was a 300ml higher blood loss (p=0. Sensory block height is measured at 10 minutes after to a higher rate of hemiparesis (9 vs. Nevertheless, signifcantly more patients with permanent routine laboratory analyses. Type of local anaesthetic used had a signifcant effect on the extent of measure to restrict intraoperative bleeding. As a precaution, it should be applied as block (isobaric bupivacaine T6, hyperbaric bupivacaine T8, hyperbaric prilocaine short and as little pronounced as possible. In collaboration clinical algorithm in patients undergoing spinal surgery with our laboratory, analyses of monoamine neurotransmitters and steroids has started. Adequate intraoperative cerebral blood fow and oxygen supply is one of the inciting causes Berezovskis R. To evaluate cognitive function, Montreal position under standard general anesthesia. Patient?s cognitive function was controlled underwent spinal tumor resection, 1 transpedicular fxation, 1 microdiscectomy. All the other intraoperative measurements Results and Discussion: In the study were included 22 patients (male-13, like mean arterial blood pressure, heart rate, peripheral oxygen saturation, end female-9, age 50+/-16,23 years). No other interventions were necessary as rScO2 be independent to sex (p=0,65), blood loss (0,331), hemoglobin (0,483), hematocrit came back to the baseline values. Conclusions: 45 % of patients showed decreased postoperative cognitive function after spinal neurosurgery in prone position. Role of brain monitoring in cerebral hypoperfusion 1Hospital Del Mar Barcelona (Spain), 2Universitat Autonoma de early detection Barcelona Barcelona (Spain) Background and Goal of Study: Sedation outside the operating room should Cavalcante S. Dexmedetomidin leads to a superfcial sedation, it interruption permits volunteers. After baseline recording, propofol infusion was started using target a vigil state patient, verbal command responding. After dexmedetomidin Pharmacokinetic data were recorded using the Rugloop program. After ten minutes the patient was completely 400?242s in men and 394?90s in women. Seven patients presented apnea, patient returned to pre-surgery neurologic parameters and aneurism embolization defned as 0 breaths/1 minute. Measurement Uncertainty is not to determine a true value as closely as possible, but to permit assignment of an interval of reasonable values to the measurand.

Cheap generic bimat canada
All supplementation should be individualised and based on regular monitoring and assessment of adherence treatment 12th rib syndrome cheap 3ml bimat visa. This is due to inhibition of vitamin K dependent carboxylase and can be reversed by administering vitamin K. Serum or plasma concentrations represent only a small proportion of total body vitamin E, which is largely found in cell membranes. Serum levels will vary according to levels of the carrier lipoproteins; to overcome this vitamin E concentrations can be expressed in relation to serum lipid levels, which requires a fasting blood sample. The water soluble vitamin E supplements have no advantage over fat soluble versions, as long as the supplement is taken with pancreatic enzyme preparations. Absorption of vitamin K from the gut depends on bile salts and pancreatic lipase secretion stimulated by dietary fat. It is an essential cofactor in the post-translational conversion of glutamyl (Glu) to y carboxyglutamyl (Gla) residues. Major Gla-proteins (active) include prothrombin, osteocalcin and other bone metabolism-related proteins. The presence of circulating Gla-proteins in their undercarboxylated forms is the most sensitive indicator of vitamin K defciency but it appears that different vitamin K dependant proteins have different vitamin K requirements. Undercarboxylated osteocalcin is the most sensitive indicator of vitamin K status of the bone and is the frst Gla-protein to occur in the undercarboxylated form in defcient states. Routine supplementation of In Europe, using a modifed Delphi process, consensus water-soluble vitamins is unnecessary unless there could not be agreed for recommending routine sodium is documented evidence of poor dietary intake or 88 supplementation in all infants. High-energy formula Sodium supplements may be given to infants in the form and protein hydrolysate formula have a higher sodium of sodium chloride solution added to expressed breast content and therefore the variable sodium content should milk, infant formula or infant fruit juice drinks, and to be taken into consideration. Sodium status is further diluted fruit squash for toddlers or as oral rehydration compromised if the infant is pyrexial or has excessive supplements (e. Sodium losses through diarrhoea or stoma output following 88,106 supplements are usually given as salt tablets for older surgery for neonatal gastrointestinal complications. Sodium supplemented sports drinks may contribute to distal intestinal obstruction syndrome. Calcium defciency results in demineralisation of the skeleton leading to osteopenia. Calcium supplements should be prescribed if dietary intake is below the recommended intake. Before commencing bisphosphonate therapy for low bone mineral density calcium intake and vitamin D status must be optimised. Plasma or serum zinc is the most widely used assessment method although their sensitivity and specifcity are poor. Levels should be tested in Serum magnesium concentrations are a poor indicator of the fasting state as there are diurnal variations and levels total active ionised magnesium levels. The associated with the use of frequent and prolonged most reliable method for diagnosing marginal zinc courses of high dose aminoglycoside antibiotics. Table 12: Recommendations of zinc supplementation for correction of defciency Age Zinc sulfate monohydrate: 125mg (45mg zinc) tablets (Solvazinc?) Child under 10kg? However ferritin is also an acute phase reactant and is elevated in acute and chronic infection and infammation. There have been concerns about supplementing with iron as many bacteria require iron for replication and respiration and iron can increase the virulence of bacteria. There was no signifcant effect on sputum iron, pulmonary exacerbation score or sputum microbiome. An optimal dose boulardii therapy, so care should be taken in and timing of antioxidant supplementation has yet to immuno-compromised patients and in those with be determined. Consideration should also presence of echogenic or dilated bowel loops on the be given to sodium supplementation. The need for additional sodium should be be associated with a number of complications such as assessed on an individual basis. If the infant has received conservative management, breast milk or standard infant formula is recommended. Following surgical intervention the choice of enteral tube feed is determined by stoma position, the extent of small bowel resection and parental preference for breast or formula milk. Breastfeeding or giving expressed breast milk has multiple benefts and should be encouraged as the frst choice of feed following surgery. Breathing patterns alter in order to and regular dietetic input is therefore vital. In practice the use of prokinetic agents may be of some assistance, and modifying the timing, rate Nutritional advice should be individualised to meet and duration of feed may be helpful. Some gastrostomy changes in nutritional requirements and dietary tubes can be used for gastric venting (removal of air). They are complex and the nutritional needs for pregnancy in women with often of multifactorial aetiology. Poor nutritional status has been shown to compromise post-transplant survival322?325 and is a risk factor for post-transplant complications. Extra energy some people consideration for transplantation is often a requirements are dependent on the intensity, duration motivating factor to try to improve their nutritional status. In the majority of cases post-transplant energy salt tablets may need to be considered. A reduction in dietary energy intake of dehydration and renal problems were anecdotally and healthier eating practices may be required to reported. There is a risk of drug-nutrient interactions due to complex post-transplant medication regimens? Encourage exercise to promote optimal in particular grapefruit juice needs to be avoided as it nutritional status and well being. Other post-transplant complications that may require nutritional intervention include hypertension,? Ensure adequate hydration and sodium intake osteoporosis, hyperlipidemia,331 diabetes, nephrotoxicity pre, during and post exercise. Distal intestinal obstruction syndrome is also common in the early post-operative period and early medical intervention is essential. In addition, severe osteoporosis is considered a relative contraindication to Cystic fbrosis-related diabetes is the most common colung transplantation. Cystic fbrosisrepeat scans every one to fve years depending on the related diabetes is associated with deterioration in result and presence of risk factors. Particular attention should be given to achieving a normal nutritional status (see section 3. Weight bearing exercise for 20 minutes two to three times per week is recommended. The exact aetiology is unknown although it control improves nutritional status and pulmonary 354 is thought to be associated with altered intestinal fuid. A intake and a similar fnding for fbre has previously been detailed dietary review should be conducted and advice noted in a previous study. However uncharacteristic or protracted improvement in nutritional status, need for liver symptoms or failure to respond to treatment must trigger transplant or death. In addition cholestasis and inadequate bile of gastrografn in the caecum by colonoscopy is acid secretion are associated with fat malabsorption. Avoidance of dehydration is to the management of patients with end-stage cirrhosis important to prevent future episodes occurring and which include: ensuring protein intakes do not exceed advice on maintaining an adequate fuid intake should 1. Maintenance of optimal weight and nutritional liver) and focal or multilobular biliary cirrhosis, with most status is the mainstay of nutritional intervention cases presenting in childhood or the early teenage years. Focal biliary cirrhosis leads to multilobular biliary cirrhosis and portal hypertension in around 5?15 percent? A recent study has condition where the stomach contents pass back up shown a reduction in pulmonary exacerbations and less into the oesophagus through the gastro-oesophageal of a decline in lung function, in addition to signifcant junction. Oesophagitis is also associated with iron defciency anaemia due to low level chronic blood loss from the infamed lower oesophagus. Effect of a newborn screening compared to a historical cohort from dietary intervention on growth and energy expenditure the same centre.
Generic 3 ml bimat free shipping
As I looked in the mirror treatment herniated disc buy generic bimat 3ml on line, I was convinced that the new me would be sexy rather than conservative, carry the attitude of a seasoned professional, and give me the confidence to perform better. My face will not be framed by baldness, or by the carefree hair of a twentyyear-old, but by the mature, commanding head of hair I was meant to have at this point in my life. A successful transplant process is really much, much more than just checking in and out of a doctor?s office for surgery, and then driving off in your convertible. Undergoing the consultations, surgery, and waking up to the possibilities of a new head of hair is a complex conversation you need to have with yourself, your hair-transplant doctor, and your stylist. Using myself as a guinea pig, I am going to give you a first-hand account in the following pages of just what to expect, what to watch out for and plan for as you go from bald to bold. This isn?t a haircut where you can afford to take a chance, and then re-do it three months later if it didn?t work out. I?ve heard it?s not all that bad, but I just don?t like hospitals or doctor?s offices, or the idea of wearing a surgical mask on the top of my head. And as the new hair grows in, would it be like spring flowers, where every day there is a bit more difference, more growth? Would I find myself staring at my new hair for hours in the bathroom mirror at 3:00 A. They say that after a week you can?t even tell the difference any more, but when would I be satisfied? The road ahead is long, and it?s very important that I make the right decisions at each step of the way, but now I have a vision. A vision of my personal successes, of my daughter being proud of her good-looking dad, of no more 3:00 A. Panagotacos and three more-than-capable nurses having the back of my head cut and all the hairs therein?3,800 of them?transplanted on the top of my head. Shouldn?t I 128 Marco?s Story be running back and forth to the bathroom to count each individual new hair, charting its hour-to-hour growth progress? Truth be known, long after that little cocktail had worn off, my memory of the day long surgery revolved around the question of whether or not I had hallucinated eating a really yummy bowl of Chinese soup with Dr. For example, the night before my operation, I had a lot more than the next day?s lunch on my mind. We?ve all had butterflies before a trip to the doctor, and some of us before a trip to the barber, but the night-before-the-hair-transplant butterflies are unique. About friends who want to tell you all kinds of stories about transplants and pain?don?t listen to ?em. There are lots of folks out there who will tell you all kinds of crazy things about post-transplant pain?everything from itchiness to blood squirting out of the tops of their heads. If you try hard enough, you?ll find someone with just the right horror story to send you into nightmares for weeks before your transplant. I don?t know if these so-called friends are some new breed of super-wimps or if they just drum up these tales to watch you squirm, but take it from me?you don?t need the advice. The actual process of having a transplant is one of the most relaxed, worry-free, painless stages of life?s hair experience. It?s done on-site in a doctor?s office and usually takes about six to eight hours you come in at 8:00 A. It?s like going to work, but instead of sitting at an ergonomically unsound desk worrying about next quarter?s figures, you spend the day on a special surgical chair, stoned out of your mind, surrounded by great-looking nurses. They asked me some standard questions, showed me some pictures, made a few jokes and then the process got under way. The nurse then proceeded to completely numb the back of my scalp with the same kind of injections a dentist uses. Under the influence of ?the cocktail all I felt was the lightest pressure?maybe as if I had on a hat that was one size too tight. The next part of the operation requires the removal of the donor hairs, which is an inch wide strip of scalp. The doctor removes the strip from the hair-rich region on the back of your head where you?ll never miss it. It?s from that strip of scalp that the hairs are extracted for transplanting into your cap. The skin is quickly stitched back together while the nurses begin working vigorously under the microscopes to remove individual follicular units for transplant. When people talk about ?pain, the donor area is usually the part of the procedure they are referring to . In my case, and in most cases, there will be a slight feeling of tightness or maybe an itching feeling 130 Marco?s Story for about a week where the skin is stitched back together. This very superficial discomfort entirely disappeared the second the nurses took the stitches out a week after the surgery. The scar, if noticeable at all, is and unobtrusive fine line, and completely hidden by your natural hair. As the nurses removed the 3,800 or so hairs from the extracted skin and turn them into little follicular unit grafts, Dr. Second, they were placed in a shape that was carefully created to mimic a natural hairline for a man my age, rather than the hairline of a teenager (although I admit I?d still like to see what I?d look like with the hairline of my early twenties). Third, and in my opinion the most impressive, the individual grafts were placed at angles to mimic natural cowlicks, waves and parts. That means that instead of 3,800 hairs growing pell-mell out the top of my head like a punk rock zombie, my hair will have shape and character, just like the natural hair we are born with. Although I?m sure I had an incredible won-ton meal somewhere during that procedure, the next thing I remembered was that beautiful and tolerant nurse gently shaking me awake. Without moving, I opened my left eye and carefully looked about for any lingering pain that might have been waiting at the threshold of consciousness, but none was there. I chuckled when, in the rear-view mirror, I caught a glimpse of the peach fuzz growing out of the top of my head in a style that was pleasantly similar to the buzz cuts that Tony the Barber used to give me in New Jersey when I was eight or nine. When you get home from your transplant, make sure you come home to exactly the environment in which you need to recover. For me that meant sending my daughter over to her friend?s for the night, and stocking the refrigerator with pasta, chicken soup and a variety of foods I?d prepared in advance. I rented twenty-four hours worth of the latest releases at the local video store, and bought two gallons of coffee ice cream with walnuts. Panagotacos had given me another ?pill cocktail to get me through the night, along with about eight pain pills to subdue any residual discomfort. My wife Janet had to work late, so the house was completely empty, leaving me nothing to do but take another ?pill cocktail and sleep it off. That bed felt like the mist of heaven as I smiled myself into a deep, healing sleep. Over the next few weeks I made some of the most profound discoveries about the hair growth process of my entire career as a stylist. My daughter came home, I returned the videos, got tired of pizza for every meal, and resumed everyday life. Two days after the procedure I returned to light duty as a stylist, performing cuts. Although I had eight pain pills in the medicine cabinet I never felt the need to take any of them (although every single client to whom I mentioned the pills made a ploy, an offer, or a plea for even one of the happy cap132 Marco?s Story sules). For me the pain had been greatly overestimated, and in hindsight seemed almost like a trivial worry. The most important thing to remember during that first week is to keep using the antibiotic ointment they give you. There are no reasons for taking any chances with that new crop of hair of yours, so grease yourself up like a championship engine and you?ll be all right. Panagotacos believes in providing those new little hairs with plenty of fertilizer. Rogaine is credited with growing hair on totally barren heads, so imagine what it can do for those 3,800 or so new seedlings. Propecia is a drug that prevents hair loss, and after the stitches are out, one tablet a day helps you keep the hair you have. In addition to the antibiotic ointment, the Rogaine, and the Propecia, I also bought a beret in case the new hair grew in funny. What a hair transplant does that isn?t so funny, is that it all falls out after the first few weeks. It takes four to six months for the transplanted hair follicles to begin to grow new hairs on a permanent basis. A week after I had the transplant, friends doubted whether I had undergone the procedure at all.

Generic 3ml bimat free shipping
Two of the studies enrolled men with predominantly mild to moderate vertex hair loss (n=1553) symptoms pancreatitis cheap 3 ml bimat mastercard. Hair counts were assessed by photographic enlargements of a representative area of active hair loss. Investigator assessment was based on a 7-point scale evaluating increases or decreases in scalp hair at each patient visit. In comparison, 6% of men treated with placebo demonstrated an increase in hair growth, 19% were rated as having no change and 75% were rated as having lost hair when compared to baseline. Other Results in Vertex Baldness Studies A sexual function questionnaire was self-administered by patients participating in the two vertex baldness trials to detect more subtle changes in sexual function. However, no significant difference was seen in the question on overall satisfaction with sex life. In general, the difference between treatment groups continued to increase throughout the 5 years of the studies. Drug/Laboratory Test Interactions Finasteride had no effect on circulating levels of cortisol, thyroid-stimulating hormone, or thyroxine, nor did it affect the plasma lipid profile (e. Finasteride does not appear to affect the cytochrome P450-linked drug-metabolizing enzyme system. In mice at a dose of 25 mg/kg/day (184 times the human exposure, estimated) and in rats at a dose of? No evidence of mutagenicity was observed in an in vitro bacterial mutagenesis assay, a mammalian cell mutagenesis assay, or in an in vitro alkaline elution assay. Administration of finasteride to pregnant rats on gestational days 6-20 at doses ranging from 100? Pregnant rats produced male offspring with decreased prostatic and seminal vesicular weights, delayed preputial separation, and transient nipple development when given finasteride at? No abnormalities were observed in female offspring exposed to any dose of finasteride in utero. No developmental abnormalities have been observed in first filial generation (F1) male or female offspring resulting from mating finasteride-treated male rats (80 mg/kg/day; 488 times the human exposure) with untreated females. No evidence of malformations has been observed in rabbit fetuses exposed to finasteride in utero from days 6-18 of gestation at doses up to 100 mg/kg/day (1908 times the recommended human dose of 1 mg/day, based on body surface area comparison). The in utero effects of finasteride exposure during the period of embryonic and fetal development were evaluated in the rhesus monkey (gestation days 20-100), a species more predictive of human development than rats or rabbits. In a study of finasteride 1 mg daily in healthy men, a median decrease in ejaculate volume of 0. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate the frequency or establish a causal relationship to drug exposure. New reports of drug-related sexual adverse experiences decreased with duration of therapy. Of the total cases of prostate cancer diagnosed in this study, approximately 98% were classified as intracapsular (stage T1 or T2). Continued use is recommended to sustain benefit, which should be re-evaluated periodically. Remember, this leaflet does not take the place of careful discussions with your doctor. Doctors believe male pattern hair loss is due to heredity and is dependent on hormonal effects. Results of clinical studies: For 12 months, doctors studied over 1800 men aged 18 to 41 with mild to moderate amounts of ongoing hair loss. Of these men, approximately 1200 with hair loss at the top of the head participated in additional extension studies, resulting in a total study time of up to five years. In general use, the following have been reported: breast tenderness and enlargement; depression; allergic reactions including rash, itching, hives and swelling of the lips and face; problems with ejaculation; testicular pain; and, in rare cases, male breast cancer. Therapeutic regimen is often cent changes in medication; hospitalizations or new stresses; dichallenging and requires multiple combinations of topical, etary habits; and general personal and family medical conditions. By doing this, loose telogen hairs are removed, and removal of more than 10% of hairs indicates exSemin Cutan Med Surg 37:247-253 2018 Frontline Medical Communications cess shedding. Examining the differences between left and right parietal, frontal, and occipital scalp can give further clues to the disease. Terminal-to-vellus hair ratio by 29 years of age, in 13% by 49 years, in 19% by 69 years, and of less than 3:1 and lack of other pathologic signs are indicative of in 25% among those over 69. Prevalence appears to for complete blood count, metabolic panel, ferritin, zinc, and vibe lower among women of Asian descent. Additional ity in frontal and vertex areas, and gradual thinning of hair density testing is relative to the patient?s history but can include more exon the central scalp. Patients frequently relate an increased sunburn tensive thyroid evaluation, microsomal antibodies, and antinuclear in those thinned areas. HowTopicals ever, scalp seborrhea and seborrheic dermatitis may be associated A summary of topical treatments is presented in Table 1. Loss of scalp hair density is progressive but slow, and usually there are no areas of complete baldness. The resulting anagen phase is prolonged while telobination of a patient?s medical and family history, trichoscopy, gen is shortened and miniaturized follicles are enlarged, resulting laboratory evaluation, and potential biopsy to further examine the in increased hair counts and weight. A randomized placebo-controlled trial demonstrated 1Department of Dermatology, Cleveland Clinic Foundation, Cleveland, Ohio. Topical treatments for female pattern hair loss Mechanism of Action Dosage Side Effects Topical minoxidil K+ channel opener with anti2% solution; 5% solution; 5% Hair shedding during the frst 2-8 weeks, scalp infammatory, antiandrogenic foam pruritus, faking, facial hypertrichosis properties Zinc pyrithione Releases zinc ion, inhibits 5? There is no evidence regarding safety recommend 5% minoxidil for its effect on hair regrowth and higher profle during pregnancy or breastfeeding. During the initial treatment period of 2 to 8 Zinc pyrithione is another antimicrobial shampoo used for sebweeks, there can be transient increase in shedding, of which paorrheic dermatitis. It is also a skin antioxidant and has been demonpruritus, faking, and facial hypertrichosis, which are more likely strated to inhibit 5-alpha reductase in vitro. The patient is supposed to lather the shampoo and leave Others it on for 5 minutes before rinsing off. Limited data are available for Several other less used topical therapies exist, including 17? Systemic treatments for female pattern hair loss Mechanism of Action Dosage Side Effects 5? Dutasteride is superior to fnasteride in inhibiting conversion of testosterone to dihydrotestosterone due to blocking type 1 and 2 of Oral contraceptives 5-alpha reductase. Starting dose is usually 50 5-alpha reductase inhibitors mg per day and is increased as needed by 50 mg per month as Finasteride is a type 2 5-alpha reductase inhibitor that works by tolerated, until dosage reaches 200 mg per day. A Vol 37, December 2018, Seminars in Cutaneous Medicine and Surgery 249 Treatment of female pattern hair loss with combination therapy menopausal women and 50 mg/day for postmenopausal women. Interventional treatments A summary of interventional treatments is presented in Table 3. This was termed paradoxical hypertrichosis and is hypothesized to occur when the laser fuence is suboptimal for thermolysis but suffcient for stimulating hair growth by acting on hair follicle stem cells or follicular keratinocytes and thus accelerating mitotic rate. Based on review of the published studies, we of cosmetic coverage, and/or anti-androgenic therapy is employed. Side effects include pain at injection site, on 34 women and found increases in hair count and density after swelling, bruising, and rarely headaches, all of which are mild and 6 months of treatment. However, lactone (25 mg) demonstrated decrease in severity of hair loss and 3 monthly sessions followed by sessions at 6-month intervals has shedding in 100 women. If using the microneedling stamp, linear movement over combination with minoxidil or fnasteride. Protective effect of zinc on keratinocyte activation markers induced by interferon or nickel. Inhibition of 5 alpha-reductase >10% increase in hair count compared with the control side; howactivity in human skin by zinc and azelaic acid. The effects of minoxidil, 1% pyrithione zinc and In our practice, we generally prescribe 5% minoxidil daily with a combination of both on hair density: a randomized controlled trial. Blume-Peytavi U, Kunte C, Krisp A, Garcia Bartels N, Ellwanger U, Hoffmann personal-choice shampoo. Comparison of the effcacy and safety of topical minoxidil and topical alfatraregrowth is unsatisfactory, additional recommendations include a diol in the treatment of androgenetic alopecia in women. Topical application of the Wnt/beta-catenin microneedling with and without minoxidil (Figure 2). Towards a consensus on how to diagnose and ism: four cases responding to fnasteride. Lack of effcacy of fnasteride in postclinico-laboratory fndings and trichoscopy depending on disease severity.