
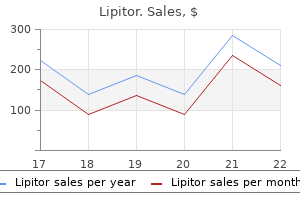
Lipitor
Buy lipitor 20 mg low price
L u m i n a l t r a c t d i s e a s e i s t h e m o s t c o m m o n References manifestation cholesterol test results non fasting buy 10mg lipitor with visa. Update on cytomegalovirus frequently observed luminal syndromes, usually infections of the gastrointestinal system in solid 1 characterized by ulcerative lesions. Curr Gastroenterol common symptoms in immunocompetent patients with Rep 2012;14:334-42. A 45-year-old woman presented with chronic intervening mucosa from sigmoid to cecum (Figure 1-3). There were numerous Physical examination revealed oral ulcers but no genital lymphocytes and large number of neutrophilic ulcer. No organism, granuloma nor intranuclear multiple discrete deep round ulcers with normal inclusion body seen in lamina propia. Figure 1-3: Multiple discrete deep round ulcers (to muscularis propia) with intervening normal mucosa along sigmoid to cecum Diagnosis: are suggestive of Behcet?s disease. While the longitudinal Intestinal Behcet?s disease ulcers and segmental/diffuse lesions suggest Crohn?s disease. Histopathological finding showed 1 aphthous ulcers, genital ulcers, uveitis, and skin lesions. Disease occurs along the ancient Silk Road References with highest prevalence in Turkey. Development and vessels is less frequent, although it can be life validation of novel diagnostic criteria for intestinal threatening. She had been well until a edematous and mild erythema of the mucosal folds at month before, she had mucous bloody diarrhea without transverse colon. Colonoscopy found continuous plasma cells infiltration at lamina propia with focal granular and friable mucosa from lower rectum to cryptitis and crypt abscess compatible with ulcerative colitis. Figure 1-2: Granular and friable mucosa at rectum, sigmoid and descending colon Figure 3: Edematous and mild erythema of mucosa Figure 4: Normal colonic mucosa at ascending colon at transverse colon Diagnosis: 3 pseudopolyps, erosions and ulcers. The granular Ulcerative colitis; granular pattern appearance is manifested by changes in light reflection during colonoscopy. It involves the rectum in about 95% of cases and may extend proximally in a symmetrical, References circumferential, and uninterrupted pattern to involve 1. The role of colonoscopy in the edema/loss of the usual fine vascular pattern, granularity differential diagnosis of inflammatory bowel of the mucosa, friability/spontaneous bleeding, disease. He was diagnosed with ulcerative colitis for 3 pseudopolyps along colon (Figure 1-4). Inclusion body and acid fast bacilli earlier, he developed bleeding per rectum and were negative. A 55-year-old man presented with significant a workup of primary tumor, he underwent colonoscopy. Computed tomography of the abdomen the endoscopic finding showed submucosal mass at showed a 5 cm heterogenous mass with mild lower rectum (Figure 3). Biopsy showed round cell tumor enhancement at pelvic cavity near the right external iliac which exhibited nest and sheet pattern. Figure 1-2: Heterogenous enhancing mass at right pelvic cavity near right external iliac artery Figure 3: Submucosal mass at rectum, 2. Endoscopic resection has the role for small nodule less 2 Discussion: than 10 millimeters in diameter. Carcinoid and other neuroendocrine colonoscopy in patients without specific rectal tumors of the colon and rectum. Physical Hilar cholangiocarcinoma usually presented in an examination revealed icteric sclera. It demonstrated a perihilar hypoechoic used for an evaluation of perihilar cholangiocarcinoma. A lymph node measuring 9x9 mm in diameter as shown in recent observational single-centered study reported that Figure 1. Bloody tissue was obtained, smeared on glass cholangiocarcinoma was 83% (25/30), however the slides and sent for pathological examination. Hepatogastroenterology hilar cholangiocarcinoma when other modalities have 2011;58:1862-5. A 58-year-old male patient presented with Diagnosis: painless jaundice for 1 month. His past history was significant for subtotal colectomy from colon cancer Discussion: 9 years ago. Linear considered potentially resectable and surgical specimen endoscopic ultrasonography vs. Pancreato1 biliary malignancy diagnosed by endoscopic ultrasonography in absence of a mass lesion on 2 2 transabdominal imaging: prevalence and predictors. The accuracy of endoscopic ultrasound, endoscopic retrograde cholangiopancreatography, computed tomography, and transabdominal ultrasound in the detection and staging of primary ampullary tumors. Upper endoscopy revealed an exophytic A recent large retrospective study reported an overall mass at mid esophagus as shown in Figure 1. This was consistent with T4 undergone minimally invasive esophagectomy; from 71 esophageal cancer. Staging of endoscopic ultrasound in preoperative staging accuracy of endoscopic ultrasound based on of esophageal cancer: results from a referral pathologic analysis after minimally invasive center for early esophageal cancer. Unfortunately, as shown in Figure 1, the duct through major papila due to enlarged and distorted ampullary tumor was so large, causing distortion of the ampulla. Figure 1: Demonstrated a fungating ampullary tumor Figure 2: Demonstrated a hypoechoic ampullary tumor Figure 3: Demonstrated a guide-wire in the common bile Figure 4: Demonstrated a guide-wire in the common duct. A 59-year-old male patient presented with Discussion: abdominal distention and significant weight loss for 10 kgs Finding the cell type of carcinomatosis peritonei in 2 months. It revealed yield as plenty amount of fluid may dilute concentration multiple peritoneal nodules and omental cake as shown of cells. Cytopathology demonstrated However, in some situation, the target lesions located mucin and multiple clusters of poorly differentiated deeply in the abdomen and thus it is quite difficult for adenocarcinoma consistent with signet ring cell the percutaneous approach to obtain tissue. Endoscopic ultrasound -guided paracentesis of ascitic fluid: a morphologic study with ultrasonographic correlation. Figure 1: Demonstrated an omental cake and lymph nodes in the abdomen Case 6 Suparat Khemnark, M. At that time, 2% ethoxysclerol was successfully injected into the rectal ethoxysclerol was injected into the rectal varices. Unfortunately, he again then doubt that if the endoscopic finding of rectal subdeveloped another episode of rectal bleeding. Diagnosis: Post-ethoxysclerol injection rectal varices References without stigmata of recent bleeding 1. Endoscopic ultrasonographic evaluation of the rectum in cirrhotic portal hypertension. Figure 1: Demonstrated a hypoechoic mass underneath the sub-epithelial rectal lesion. A 71-year-old female patient presented with Discussion: abdominal pain for 9 months. Over the last 2 months, In patient with indeterminate biliary stricture she developed jaundice. Cholangiogram revealed distal biliary stricture role in order to identify the nature of stricture. A and a plastic biliary stent was subsequently placed retrospective study published confirmed this fact as it across the stricture. Endoscopic ultrasound and fine-needle aspiration of unexplained bile duct strictures. Figure 1: Demonstrated periductal lymph nodes surrounding distal common bile duct. An 85-year-old male patient was recently have a common bile duct stone as these tests provided diagnosed as colon cancer with liver metastasis. Ultrasonographic images showed a hyperechogenic References material in common bile duct as shown in Figure 1. E U S a n d M R C P s e e m t o b e t h e m o s t appropriate tests in patients with intermediate risk to Figure 1: Demonstrated a hyperechoic structure with posterior acoustic shadow in distal common bile duct. This was consistent with distal common bile duct stone Case 9 Tanassanee Soontornmanokul, M. Three days Discussion: after the procedure, a markedly distended gall bladder Cystic duct obstruction is the main cause of causing a hydrop gallbladder was noted. Technical and clinical success rate were Good cystic fluid was observed (Figure 5).
Order 20 mg lipitor fast delivery
The differences between the study groups were evaluated were nausea and other complication grocery list cholesterol lowering foods buy lipitor 40 mg cheap, orthostatic tolerance in the 1 postoperativest using the Bonferroni-adjusted Mann-Whitney U test and p<0. Primary spread of caudal blockade in children References: anatomical perspective 1. It also remains to be explained why there is very little difference in initial cranial spread Background and Goal of Study: Austerity in Greece has slowed down despite using a low or a high volume caudal injection (0. The goal of this audit was to goal of the study is to explore if there exists an anatomical explanation that can benchmark pain management in ?Paidon Agia Sofa?, the largest Greek paediatric explain why the initial injection of local anaesthetic only reaches the thoraco-lumbar hospital and inform the need of introducing an acute pain service. Our hypothesis was that the lumbar spinal Materials and Methods: the audit included more than 1/3 of the overall hospitalized cord enlargement (tumenescence) may constitute the anatomical barrier that limits children and incorporated data from a single day. The corresponding axial slice completely surrounded their current hospital stay and were further explored: 57,79% of them belonged by bone and cartilage was assessed for three areas: 1. Among the cases with position of the lumbar tumenescence was found to coincide with the thoracolumbar unsure/ inadequate analgesia despite taking analgesics (26. Conclusions: the increased resistance due to the presence of the lumbar Conclusions: Wardbased pain management is effcient for most of the cases. More than a quarter of the patients who require analgesics would probably beneft from a more intense pain management plan. Pain prevalence in hospitalized children: a prospective cross-sectional survey in four Danish university hospitals. Pain in hospitalized children: a prospective cross-sectional survey of pain prevalence, intensity, assessment and management in a Canadian pediatric teaching hospital. Recently, the satisfactory control of post-operative pediatric pain has seen resurgence of interest as medicine seeks alternatives to narcotics. However Background and Goal of study: the aim of the study was to assess the effcacy the secondary benefts of this care (reduction in anxiety and patient costs) also bear of caudal dexamethasone with bupivacaine 0. Postoperatively Results and Discussion: the improvement and duration in quality pain control patients were assessed for analgesia and side effects. Children rated high levels and prolonged duration of post-operative analgesia was observed from pain relief at 3. Conclusion: Caudal dexamethasone may safely improve and prolongs postConclusions: We found discharging patients home with good pain control on the operative analgesia for sub-umblical surgical procedures in children. We started included 137 paediatric patients undergoing liver transplantation between April rapid sequence induction with 0. After the application of cricoid pressure we gave additional 1mg/ stage kidney disease; and use of preoperative renal replacement therapy. Endotracheal intubation was quickly done with defned according to the Kidney Disease: Improving Global Outcomes guidelines 7. Endoscopy lasted 2 and a half hours but the toothbrush after liver transplantation. Statistical analyses were performed by using Fisher?s couldn?t be removed endoscopically. We added 10mg rocuronium and then the exact test, Mann-Whitney Utest and multivariate logistic regression analysis. Then she started breathing spontaneously and was analysis revealed that Child-Pugh score B or C (odds ratio, 2. High Child-Pugh score, a large amount of intraoperative blood loss and a gastrointestinal tract: a retrospective study of 1294 cases. Scandinavian journal of large postoperative positive fuid balance were independently associated with the gastroenterology, 2017. Learning points: It is important to prevent aspiration in the foreign body ingestion procedures. We therefore describe our single-centre experience with this simple Background and Goal of Study: the use of centrally inserted central venous technique for major neonatal surgery and the perioperative period. Data were extracted from the electronic anaesthesia and intensive care Materials and Methods: this retrospective study was performed using data unit records. Relationship between demographic, clinical and hematologic variables was time of surgery of which 84,8% had laparotomy and 15,2% thoracotomy were investigated. Identifcation of patients who may require revision intervention and increased Conclusion: Continuous caudal anaesthesia with intermittend peridural morphine awareness on catheter infection may improve success rate and decrease the is a feasible anaesthetic technique for major neonatal surgery with the potential likelihood of complications and hazards. Retrospective analysis of 166 central line placements Acknowledgements: the author would like to acknowledge the assistance of in children Tanja Rappel with data extraction. Materials and Methods: the entries from 2016, 2017 interventions Pediatric Kamal M. Background: Epidural analgesia is the standard and reliable technique of 68% of time the right internal jugular vein was used followed by the subclavian and perioperative pain relief in patients undergoing abdominal and thoracic surgeries. In 63% the vein was It?s use in paediatric age group is not being widely practiced because of concerns cannulated from the frst attempt. In one patient 10 attempts for higher chances of dura puncture and neurological complications as they have were made at different sites. In 22% a straight wire was used instead of a J informed parental consent were taken. Analysis showed that cannulation attempts and diffculties were more frequent surgery, neurological disorder, coagulopathy, local infection or sepsis and allergy with decreasing weight, especially below 5 kg. Under general anaesthesia, in left lateral patients were non-advancement of the J wire and malposition of the needle after position, congruent epidurals were inserted using linear/hockey probe (8 to13 disconnection from the syringe. Also when a cathlon was used instead of a needle no optimum ligamentum favum and anterior dura complex views by para median syringe was necessary. Further confrmation of epidural space was done by loss of resistance to saline and Conclusions: As expected the most challenging patients proved to be the youngest. Procedure time, number of bone contacts or needle redirections, number of 5 kg it is better to use a straight wire. A cathlon catheter instead of a needle can attempts and procedure related complications like dura puncture, bloody tap were reduce malpositioning due to syringe disconnection. Results: Real time ultrasound guided epidural placement was performed in 9 infants in lower thoracic and upper lumber interspaces. Seven out of 9 required single needle insertion attempts, while 2 and 3 attempts were needed in one patient each. Two patients had no bone contact, while 4 had single bone contact and 3 had it twice. No needle redirections were required in 2 patients, single redirections in 2 patients and 2 redirections in 4 patients. Discussion and Conclusion: Ultrasound helps in identifcation of interlaminar space, ligamentum favum, dural complexes and needle tip. Jayme Santos Neves Serra (Brazil), 2Disciplina high risk of perioperative complications. We reviewed patients with congenital heart diseases who had undergone general anesthesia at Kitasato University Hospital between Background: Sugammadex can be used for immediate reversal of neuromuscular January 2016 and August 2018 and ranged in age from 0 to 12 years. Although its use is extensively procedures, anesthesia methods, airways management, intraoperative elapsed described in adults for elective and emergency purposes, sugammadex is still time, perioperative complications such as cardiovascular events, and outcomes an off-label alternative in the neonatal and pediatric populations. Perioperative complications were observed in 16 Case Report: A 30 weeks 2/7 premature female neonate with 1060g was scheduled cases (17. Focusing of department, pediatric surgery and anesthesia was induced and maintained with dexmedetomidine, S-ketamine otolaryngology have a larger number of noncardiac surgery cases, and the frequency and fentanyl. Despite appropriated anesthetic doses for providing hypnosis and of perioperative complications in pediatric surgery was the highest (68. Then, it was of perioperative complications in noncardiac surgeries for pediatrics with congenital decided to administer rocuronium. However, after apnea, she became impossible heart diseases indicated that the frequency of perioperative complications are same to be ventilated or oxygenated, presenting with increased abdominal volume, or slightly higher when compared with previous reports. While the surgeon was preparing for an emergency diseases group had a higher frequency of perioperative complications, such as gastric decompression, it was given a high dose of sugammadex with atropine. In spite of all the expected and inherent challenges of the procedure, the consideration of treated or untreated cardiovascular disease. In addition, clinicians fstula was ligated and the esophagus was successfully reconstructed. Enteral should consider both circulation and airway management as important factors. However, there are no data available about the effcacy and safety of Niigata (Japan) the drug in this age group. In addition, for example, in patients with pulmonary artery stenosis (such as in Tetralogy of Fallot) with no venous blood Anesthetic management in pediatric patients with access or in whom a venous catheter is not available due to an extravascular leak congenital long qt syndrome undergoing left cardiac suffering an anoxic spell, swift intravenous catheterization for fuid and medication administration is needed.
Discount lipitor 20mg line
Classifying the six patients according to the most advanced polyp histology cholesterol cell definition buy lipitor 20 mg without a prescription, one patient had a negative colonoscopy (no polyps found), one patient?s polyps were hyperplastic, one had a tubular adenoma, two had advanced neoplasia (tubulovillous adenomas) and one had adenocarcinoma. Overall, many difficulties were anticipated and addressed in the development of the training program; ultimately, the project was affected most directly by challenges in encouraging family physicians to refer patients to the program. As health human resource strategies continue to evolve, it is believed that lessons learned from experience make an important contribution to the knowledge of how non-traditional health services can be organized and delivered. Background: Previous researchers have shown that non-medical Endoscopists can perform lower gastrointestinal endoscopy as safely and effectively as medical staff. Aim: To determine differences in the yield of diagnosis for significant disease during upper gastrointestinal endoscopy performed by nurse and medical Endoscopists and to measure patient discomfort, satisfaction, and attitudes towards future endoscopy. Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 96 Patients: this two part study included 3009 patients in a retrospective analysis and 480 in a prospective study. Methods: the first part of the study assessed indications for endoscopy, diagnoses, and procedures performed by medical and nurse Endoscopists. In a second prospective study, 480 patients were included to determine the association between Endoscopist type and sedation, patient anxiety, discomfort, satisfaction, and attitudes towards future sedation. Results: No patient refused endoscopy by either a nurse or medical Endoscopist and there were no complications in either group. Nurses performed 1487 procedures and reported fewer endoscopies as ?normal than medical staff (p=0. Multivariate analysis showed that male sex, older age, inpatient status, dysphagia, and gastrointestinal bleeding, but not Endoscopist type, were all associated with significant disease. In relation to discomfort and satisfaction, a similar proportion of patients received sedation in both groups (p=0. Conclusion: Experienced nurses perform routine diagnostic gastroscopy safely in everyday clinical practice and with as little discomfort and as much patient satisfaction as medical staff. Subsequent studies have reported that nurses can be trained to the same technical skill level as their medical counterparts with regards to adequate completion of procedures, diagnosis, treatment and patient safety [54]. The training for a nurse Endoscopist is based on the training of the medical model but has additional training attached. Trainees need to Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 97 understand appropriate techniques of patient preparation, the mechanics of the procedure and its indications, limitations and complications. Each trainee should complete a minimum of 100 procedures in one year and can demonstrate intubation skills in at least 50 per cent of procedures. The trainees are required to be competent in the techniques of hot biopsy, polypectomy and treatment of colonic bleeding. In addition trainees need to be family with balloon dilation of strictures and techniques to stop bleeding and treat angiodysplastic lesions. In addition online discussions with members from the entire community were undertaken during 2009 and 2010. A minimum benchmark for annual screening examinations is set at 300 colonoscopies. A population-based study from Canada found that the risk of complications such as perforation and bleeding was increased threefold with colonoscopists who performed fewer than that threshold of 300 colonoscopies per year. The 2010 paper refers to colonoscopists, which encompasses advance health practitioners nurses, as opposed to gastroenterologists alone. They emphasise that in the long term an experienced multi-skilled nurse or other professional working at an advanced practitioner level would be able to assist with colonic surveillance and diagnostic programs. The position statement also reiterates that ongoing support once training has been undertaken is fundamental for Nurses and advanced health practitioners [56]. United States the recommendations from the American Society for gastrointestinal endoscopy [57] were: the performance of flexible Sigmoidoscopy for colorectal cancer screening by nonphysician Endoscopists is supported when intensive training occurs by a certified Endoscopist. There are insufficient data to support non-physician Endoscopists to perform colonoscopy and upper endoscopy. It should be noted that an analysis was only undertaken of published literature from the United States of America and excluded international evidence (pg. Working within endoscopy the post holder will identify the need for and request further investigations as appropriate and advise on further investigations as required. The post holder would provide regular endoscopy sessions and on a flexible basis so as to cover unfilled lists. The post holder will provide professional leadership by personal example and ensure the delivery of a high quality, patient centred service across Endoscopy services. The post holder will undertake the clinical validation of the endoscopy waiting lists. The nurse Endoscopist will act as the clinical expert and professional resource to the multiprofessional team, patients and carers within their specialist service. This will include the management of a caseload of patients, as appropriate, including specialist clinics. His / her own working practice should be developed to a level whereby they can directly or indirectly influence all aspects of care and management of patients within the speciality. The post holder will ensure the delivery of high quality, clinically effective care, prioritising and utilising research and collaborating with colleagues in everyday practice. The role involves clinical leadership, working in partnership to enhance professional standards of care across the speciality. Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 99 1. Clinical decision making skills and legal accountability must be understood together with the principles of precarious liability. Be an active member of the endoscopy users group and have responsibility for designated audits. Regularly update the Clinical Lead and Directorate Manager of progress against the action plan. Support the clinical lead/clinical governance lead in collection and analysing the Endoscopist quality and safety data and ensure anonymised data is fed back to individual Endoscopists. Work collaboratively with colleagues to develop effective documentation, pathways, protocols and guidelines for care. Include in this report incidence of hospital deaths within 30 days of an endoscopic procedure and all non-elective operations required within 8 days following the endoscopic procedure. Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 102 Appendix 5: Data Collection Methodology the data collection for admitted patients was undertaken by the Health Statistics Centre. Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 103 Procedure block codes were not available at the time of initial analysis. Table: List of procedural block codes utilised in activity count Procedure Block code Procedure Block Description 0850 Oesophagoscopy 0851 Endoscopic administration of agent into lesion of oesophagus 0852 Removal of foreign body from oesophagus 0853 Other application, insertion or removal procedures on oesophagus 0856 Destruction procedures on oesophagus 0861 Other excision procedures on oesophagus 0862 Dilation of oesophagus 0870 Application, insertion or removal procedures on stomach 0874 Destruction procedures on stomach 0882 Endoscopic dilation of gastric stricture 0890 Other procedures on stomach 0891 Exploration of small intestine 0892 Application, insertion or removal procedures on small intestine 0903 Other procedures on small intestine 0904 Rigid sigmoidoscopy 0905 Fibreoptic colonoscopy 0906 Application, insertion or removal procedures on large intestine 0908 Destruction procedures on large intestine 0909 Biopsy of large intestine 0910 Rigid sigmoidoscopy with excision 0911 Fibreoptic colonoscopy with excision 0914 Other excision procedures on large intestine (excluding 32029-00) 0925 Other procedures on large intestine Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 105 Overview of the planned introduction of nurse endoscopy in Queensland Nursing and Midwifery Office, Queensland 106 -. T-applications ?P roctoscopy ?A nd m any oth ersurgical applications ((gastrectom y,neurosurgery, etc). ThThiis ss shhaappe re reessulltts is in en eaassy orientation of the capsule axis along the centralaxis of sm all intestine andso helps propelthe ccaappssuulle foe forrw aw arrddeeaassiillyy. The lens is tightlyfixedto the hhoollddeerrsso to thhaattiittddooeessnnt?tggeett dislocatedanytim. S ilverO xide prim arybatteries are used(Zinc/A lkaline E lectrolyte/S ilver O xide). S uch a batteryhas a even ddiisscchhaarrgge ve voollttaaggee,ddiissppoossaabblle ae anndd doesn?tcause harm to the body. The advantages are that it is possible to search any database created, perform statistical analysis, and avoid the need for hand-written or typed reports. Around the world, a considerable number of endoscopy record systems have been developed but there has been no standardization of the terminology used. As a result, a golden opportunity has been lost for sharing and comparing data collected from different centers. Classen in Munich in 1991, it became apparent that this important problem needed resolution. Crespi and included a number of experts from Belgium, France, Germany, Hungary, Italy, Spain and the United Kingdom. Additionally, the three major endoscope manufacturers (Fujinon, Olympus and Pentax) and the publisher Normed-Verlag were invited to join the committee as it was imperative that industry should be involved in this work as they were developing their own systems and compatibility between these was regarded as vital if the opportunities for sharing data were to be optimized. It was also important that these companies be involved in discussing other aspects, such as image capture, storage and transfer. At this time, the work was reviewed and modified and the Committee was constituted as the Working Party for this report for the World Congresses of Gastroenterology and Digestive Endoscopy. The major aim of the project was to devise a "minimal" list of terms that could be included within any computer system used to record the results of a gastrointestinal endoscopic examination.
5 mg lipitor mastercard
Last 6 months of clinical notes from requesting provider the following information was used in the development of this document and is provided as background only cholesterol values high buy 5mg lipitor free shipping. Background Lymphedema is a chronic progressive disorder of the lymphatic system characterized by interstitial accumulation of protein rich fluid. This occurs when lymphatic transport is reduced causing lymphatic stasis and subsequent protein accumulation within tissues. Accumulation of protein and fluid in the tissues triggers an inflammatory response and swelling that eventually leads to fibrosis. Primary lymphedema is rare and results from congenital anatomic abnormalities of the lymphatic system such as lymphatic hypoplasia or dysfunction of lymphatic valves. Secondary lymphedema on the other hand, is more common and may result from disease, trauma, surgery, or radiation therapy. In the United States, the most common cause of secondary lymphedema is malignancy and its related treatment, particularly in breast cancer patients treated with axillary surgery and/or radiation therapy (Warren 2007). This big variation in reported incidence of lymphedema is due to lack of a standardized assessment and differences in diagnostic criteria. Lymphedema may cause limb swelling, heaviness, pain, pitting of the skin, tightness, inflammation, reduced mobility, and impaired 2011 Kaiser Foundation Health Plan of Washington. Back to Top Date Sent: 3/24/2020 139 these criteria do not imply or guarantee approval. Accurate assessment of lymphedema may facilitate earlier diagnosis and monitoring of treatment response. Physical measurements used include limb circumferential assessment with a tape measure, and limb volume measurement using water displacement or optoelectrical perometry (also known as infrared volumetry). Limb circumference is used to calculate volume by assuming either cylindrical or truncated cone geometry. It thus indirectly measures the limb volume and may be confounded by changes in muscle and fat mass. Water volumetry or displacement, in which the limb is lowered in a water tank, has been considered by many as the reference method for determining limb volume. It is a reliable method and provides a way of including volumetric measurements of the hand or foot in the total limb volume measurements. However, water displacement cannot distinguish changes due to fat or muscle from extracellular fluid accumulation. The Perometer is an opto-electrical device that has a square frame in which the extended extremity is placed. The frame emits infrared light and slides up and down scanning the patient?s extremity and recording cross sectional information every 3 mm. Limb volume is then calculated based on the assumption that the cross-section is an ellipse or circle. Many investigators consider perometry the modern gold standard for the assessment of limb volume. It is however, bulky in size, not available in most clinics, and cannot be used for bedridden patients. In more challenging cases radiologic imaging studies as lymphoscintigraphy, magnetic resonance imaging, or computerized tomography may be necessary to diagnose lymphedema (Sander 2002, Warren 2007, Jain 2010, Czerniec 2010, Smoot 2011). While circumference and volume measures are reliable measures for changes in limb volume, they are not specific to lymphedema. It attempts at measuring lymph volume directly and detecting early increase in the extracellular fluid at a subclinical stage of lymphedema before it is manifests as a change limb volume. Current flows along the path of least resistance through the body and thus follows tissues with the highest water content. Tissues as fat and bone act as insulators, while electrolyte body fluids conduct electrical current and as the fluid increases, impedance to current flow decreases, i. At low frequencies, cell membranes are non-conductive and current passes only through the extracellular fluid, while at high frequencies, the current passes through cell membranes in addition to the extra-and intracellular fluids. However, the reviewers indicated that most of the diagnostic studies involved patients with breast cancer. They noted that based on the evidence from the studied reviewed, there does not appear to be a gold standard for grading or measuring the severity of lymphedema. Articles: the search revealed a recent comprehensive review on the diagnosis and treatment of 2011 Kaiser Foundation Health Plan of Washington. Back to Top Date Sent: 3/24/2020 140 these criteria do not imply or guarantee approval. Comparison of diagnostic accuracy of clinical measures of breast cancer-related lymphedema: Area under the curve. The use of bioimpedance lymph analysis does not meet the Kaiser Permanente Medical Technology Assessment Criteria. Back to Top Date Sent: 3/24/2020 141 these criteria do not imply or guarantee approval. Blepharoplasty for the following diagnoses may be considered medically necessary for an affected upper or lower lid without meeting visual loss criteria: 1. Does not have unstable myasthenia gravis or a thyroid condition (No concerns about stability raised by Neurology for myasthenia gravis patients and normal thyroid lab if patient has pre-existing thyroid disease) 5. Visual field less than 20 above central fixation 1998Kaiser Foundation Health Plan of Washington. Back to Top Date Sent: 3/24/2020 142 these criteria do not imply or guarantee approval. The upper eyelid position interferes with the fit of eye prosthesis in the socket. Blepharoplasty of the lower lids for excessive skin that does not correct a functional issue is considered cosmetic under the member benefit. Background this service is covered when it is medically indicated and determined not to be for cosmetic. The Medicare coverage language includes the identification of how to determine medical necessity. In order to determine coverage, the clinical history submitted by the requesting physician should include the reason for the surgery and the identification of the procedure to be done. Back to Top Date Sent: 3/24/2020 143 these criteria do not imply or guarantee approval. Criteria | Codes | Revision History Codes Blepharoplasty 15820, 15821, 15822, 15823 Brow Lift 67900 Blepharoptosis 67901, 67902, 67903, 67904, 67906, 67908, 67909 1998Kaiser Foundation Health Plan of Washington. Back to Top Date Sent: 3/24/2020 144 these criteria do not imply or guarantee approval. Last 6 months of clinical notes from requesting provider &/or specialist (Orthopedics/podiatry). Copies of last 12 months of x-rays of involved area the following information was used in the development of this document and is provided as background only. Background Electrical stimulation has been used as treatment for nonunion of fractures since the early 1950?s with a reported success rate of 80-85%. Bone Stimulators are covered in Kaiser Permanente plans that include coverage for durable medical equipment. The criteria for coverage had previously been part of the Durable Medical Equipment Formulary. Because of the renewed attention on this mode of treatment by Kaiser Permanente orthopedists, the referral management staff requested that clearer criteria be developed for reviewing coverage requests (1/97). The healing process is delayed in approximately 10% of the 6 million fractures that occur annually in the United States. A portion of these delayed unions do not heal by 9 1997 Kaiser Foundation Health Plan of Washington. Back to Top Date Sent: 3/24/2020 145 these criteria do not imply or guarantee approval. Criteria | Codes | Revision History months after fracture and are categorized as non-unions (Hadjiargyrou, 1998). Electrical stimulation has been found to offer a reasonable means of treatment for nonunion that have failed to respond to previous bone grafting over an extended period of time. The effective use of electrical stimulation devices requires an understanding of the various principles and concepts employed by the four types of stimulators currently available. While the exact mechanism of electrically-induced osteogenesis is uncertain, current theories indicate that several factors probably are involved, and more than one mechanism may be responsible. Ultrasound, a form of mechanical energy that is transmitted through and into biological tissues, has a variety of diagnostic and therapeutic clinical applications. Research on the use of ultrasound to accelerate the healing of fractures has been done largely using animal models.
Lipitor 20 mg fast delivery
The newer sensors were also more reliable than the original sensors cholesterol medication doesn't work order lipitor overnight, but measurement taken by two new sensors differed from one another by more than 20% about one-fourth of the time. However, the authors did not discuss the impact of these changes on health outcomes. The evidence is insufficient to determine the effect of continuous glucose monitoring on improving health outcomes. Adult population There is less published empirical evidence in the adult population and no high-quality studies on accuracy. The best available study (Yogev) was on pregnant women with type 1 diabetes (not on patients with uncontrolled diabetes). In this sample, continuous glucose monitoring detected hyperglycemia that was not detected by self-blood glucose monitoring in all 34 patients and nocturnal hypoglycemia in 26 (76%) patients. Recommendations to change insulin treatment were made for 24 out of the 34 (70%) patients. However, the authors did not present data on how the change in recommendations affected maternal or neonatal outcomes. Articles: the Medline search yielded 52 articles, some of which were reviews or opinion pieces, were on technical aspects of glucose monitoring or had outcomes unrelated to the accuracy of the glucose monitor. Another was a case series with 28 patients and appeared to be relatively weak methodologically (e. Back to Top Date Sent: 3/24/2020 263 these criteria do not imply or guarantee approval. Criteria | Codes | Revision History monitor in the analysis, did not discuss management changes following use of the monitor) (Salardi, 2002). The remaining 3 studies, one of which was a randomized cross-over trial, were critically appraised: Diabetes Research in Children Network (DirecNet) Study Group. Continuous subcutaneous glucose monitoring improved metabolic control in pediatric patients with type 1 diabetes; A controlled crossover study. One was specifically on diabetic patients needing dialysis and included only 8 patients. The remaining study, which studied pregnant women with type 1 diabetes, was critically appraised: Yogev Y, Chen R, Ben-Haroush A. Continuous glucose monitoring for the evaluation of gravid women with type 1 diabetes mellitus. Use of the continuous glucose monitoring system to guide therapy in patients with insulin-treated diabetes: A randomized controlled trial. The study evaluated both device accuracy compared to self-monitoring of glucose measurements and impact on short-term glycemic control. In 47 patients, 95% of paired sensor-home monitoring data points over nine days were in Clarke error grid regions A (clinically accurate) or B (acceptable). In addition, compared to a control group (n=44) that used devices but did not receive display information, there was a statistically significant improvement in glycemic control (more time in target glucose range, less time in hypoglycemic and hyperglycemic ranges). Another remaining issue is the 15-30-minute lag time between interstitial glucose readings and blood glucose levels when the blood glucose is rising or falling quickly. This was a randomized controlled trial with 91 patients and was critically appraised: Garg S et al. Improvement in glycemic excursions with a transcutaneous, real-time continuous glucose sensor. An issue identified was the 15-30-minute lag time between interstitial glucose readings and blood glucose levels when the blood glucose is rising or falling quickly. Back to Top Date Sent: 3/24/2020 264 these criteria do not imply or guarantee approval. Criteria | Codes | Revision History Navigator was tested in an inpatient setting in adults. Significant reductions in HbA1c over 13 weeks were also found in small case series with children who were managed with the FreeStyle Navigator. The available evidence is insufficient to evaluate the impact of real-time continuous glucose monitors on detection of hypoglycemic episodes, larger sample sizes and longer follow-up are required. The use of continuous glucose monitoring in the management of diabetes does not meet the Kaiser Permanente Medical Technology Assessment Criteria. There is insufficient evidence to determine whether use of the 7-day real-time continuous glucose monitoring systems leads to better patient-oriented health outcomes (e. There was a relatively large trial by the Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Group (2008) that used change in the HbA1c as a surrogate outcome for diabetes control. Even when taking the average of four sensors worn simultaneously (an impractical approach for everyday use) results vary from the true plasma glucose value by 25 50% almost 20% of the time when patients 2001 Kaiser Foundation Health Plan of Washington. Back to Top Date Sent: 3/24/2020 265 these criteria do not imply or guarantee approval. Criteria | Codes | Revision History true blood glucose values were less than 70 mg/dL. Additionally, most studies show no or only trivial improvement in HbA1c, that is not sustained overtime. Articles: No studies were identified that addressed patient-oriented health outcomes. Assessment of patient-led or physician-driven continuous glucose monitoring in patients with poorly controlled type 1 diabetes using basal-bolus insulin regimens: a 1-year multicenter study. The accuracy benefit of multiple amperometric glucose sensors in people with type 1 diabetes. A randomized clinical trial to assess the efficacy and safety of real-time continuous glucose monitoring in the management of type 1 diabetes in young children aged 4 to <10 years. See Evidence Table the use of continuous glucose monitoring in the diagnosis of diabetes does not meet the Kaiser Permanente Medical Technology Assessment Criteria. Real Time Continuous Glucose Monitoring in type 1 diabetes: A Systematic review and Individual Patient Data Meta? Multicentre randomized controlled trial with sensor-augmented pump vs multiple daily injections in hospitalized patients with type 2 diabetes in China: Time to reach target glucose. Back to Top Date Sent: 3/24/2020 266 these criteria do not imply or guarantee approval. Back to Top Date Sent: 3/24/2020 267 these criteria do not imply or guarantee approval. For Non-Medicare Members There is insufficient evidence in the published medical literature to show that this service/therapy is as safe as standard services/therapies and/or provides better long-term outcomes than current standard services/therapies. Back to Top Date Sent: 3/24/2020 268 these criteria do not imply or guarantee approval. For Non-Medicare Members Cosmetic Surgery is performed to reshape normal structures of the body in order to improve appearance in the absence of a specific functional improvement. Reconstructive Surgery is performed to restore bodily function or to correct a deformity resulting from disease, injury, trauma, birth defects, congenital anomalies, infections, burns or previous medical treatment, such as surgery or radiation therapy. Reconstructive surgery is reasonable and necessary to improve the functioning of a malformed body part. Have been refractory to systemic treatment for bacterial infection control with oral or parenteral antibiotics. Back to Top Date Sent: 3/24/2020 269 these criteria do not imply or guarantee approval. If the procedure is being performed following significant weight loss, in addition to meeting the criteria noted above, there should be evidence that the individual has maintained a stable weight for at least six months. If the weight loss is the result of bariatric surgery, procedure should not be performed until at least 18 months after bariatric surgery. Not covered when performed in conjunction with abdominal or gynecological procedures (e. Not covered to minimize the risk of hernia formation or recurrence See individual links below for the following potentially cosmetic procedures:. Vein Procedures the following are considered cosmetic in nature and non-covered under members contact:. Canthoplasty (?outer eyelid lift surgery If requesting this service, please send the following documentation to support medical necessity:. However, some procedures may be medically necessary when certain clinical criteria have been met. This document has been created to provide guidance to physician?s reviewers when reviewer requests to cover potentially cosmetic services. Back to Top Date Sent: 3/24/2020 270 these criteria do not imply or guarantee approval. Criteria | Codes | Revision History Revision Description History 11/01/2015 Changed Medicare links 05/03/2016 Added definitions for Cosmetic vs.
Dog-Tree (American Dogwood). Lipitor.
- Are there safety concerns?
- Headaches, fatigue, weakness, fever, chronic diarrhea, loss of appetite, malaria, treating boils and wounds, and other conditions.
- How does American Dogwood work?
- What is American Dogwood?
- Dosing considerations for American Dogwood.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96525
Buy lipitor 5 mg on line
A code from category K65 Catheterisation of heart must not be assigned in addition to codes in category K63 Contrast radiology of heart as catheterisation is implicit within these codes cholesterol chart mmol cheap lipitor 20mg. Examples: Coronary arteriography using two catheters performed during the same radiology/theatre visit with a left ventriculography under percutaneous image control K63. Certain specific blood vessels are excluded from this chapter and are classified in other body system chapters. For ?other specified and ?unspecified procedures on named arteries that cannot be classified at specific fourth-characters within categories L66 and L71, the. Example: Percutaneous transluminal atherectomy of common femoral artery under image control L71. A site code must be assigned in addition when the artery is listed as an inclusion term. Where the artery is not specifically referred to within the code description or inclusion, even if the origin is known, do not assign a code from these categories. A code from categories L65?L72 must be used instead with the addition of a site code from Chapter Z where available. Due to the vast number of arteries in the human body, it is not possible to allocate categories for specific operations on every named artery, down to the smallest branch. This allows the classification of a major part of arterial surgery into a relatively small number of discrete anatomical groups. These codes must be supplemented by a code from categories L76, L89 or O20, to indicate the type and number of stents or stent grafts inserted, as indicated by the Notes at category or code level. When a stent has been inserted and the number and type of stent is unknown, the default code is L76. When a stent graft has been inserted and the number and type of stent is unknown, the default code is O20. When angioplasty and insertion of stent or stent graft are performed at the same time and individual codes are available for the angioplasty and for the stent/stent graft insertion, only the code for the stent/stent graft insertion is required, because the angioplasty is implicit within the stent/stent graft insertion code. Example: Bypass of segment of aorta by anastomosis of aorta to common femoral artery L21. A code from Y53 Approach to organ under image control must be assigned in addition. However, if the stent is left in situ following the lithotripsy in order to facilitate the passage of fragments of the calculus, then the stent insertion would require coding in addition to M31. If a patient is catheterised for urinary retention (which may have been present on admission or developed during the admission) the insertion of the urethral catheter and its subsequent removal would not be considered a routine part of care and both the insertion and removal of the catheter must be coded. If a urethral catheter is inserted routinely, but following removal the patient is unable to void urine, this indicates that the patient is in urinary retention. The reinsertion of the urethral catheter, and its subsequent removal following reinsertion, would not be considered a routine part of care and both the reinsertion and subsequent removal of the catheter must be coded. Two days after surgery the patient develops postoperative urinary retention that requires catheterisation. Vaginal procedures carried out to support the outlet of the female bladder, for example, stress incontinence, must be classified to Chapter M. Where pieces of prosthetic mesh have become exposed the clinician can repair this by oversewing the mesh with vaginal epithelium. Dilation and curettage (D&C) and hysteroscopy can be performed for diagnostic or therapeutic purposes: however, there are often occasions where this can be a combination of the two. For example, a uterine curettage can be performed to provide a tissue sample for diagnostic purposes, but it is also hoped the removal of this tissue will have some therapeutic benefits. A hysteroscopy will always be carried out in a hospital setting by a gynaecologist. Each different type of delivery must be recorded with the most serious being sequenced first. The definition of a normal delivery is the process of giving birth without mechanical intervention with a vertex (top of the head) presentation. Elective caesareans performed when the patient is in labour are likely to have similar risks to the mothers as emergency caesarean deliveries. Patient goes on to have an emergency lower caesarean section with delivery of a live female infant R18. Neville Barnes, even though that type may be normally used for a mid forceps delivery, the coder must ascertain that this is in fact the case. In these cases a code from category R32 Repair of obstetric laceration must be assigned in addition, to classify the repair of the perineal tear. Codes from Chapter S can be used to enhance various codes from other body system chapters. This is indicated by the note at the relevant categories in the body system chapters and at the beginning of Chapter S. Where the same type of phototherapy is administered more than once during a consultant episode, assign the relevant code from category S12. Other types of skin graft (skin grafts using material not harvested from patient. Examples: Full thickness skin graft to left canthus, graft harvested from skin of right shoulder C11. When other procedures have taken place then the debridement must be coded in addition to these other procedures (the sequencing will depend on the main procedure performed). Where skin graft and skin debridement have been performed, the skin graft must be selected as the primary code as this is the main procedure performed. Resuture of skin this is a further repair of a wound which has previously been sutured. If the joint is released, this must be coded to category W78 Release of contracture of joint. If the clinician states that they performed a block dissection it is correct to assign a code from category T85 Block dissection of lymph nodes, irrespective of the number of nodes removed. The standard to only code diagnostic imaging procedures in an outpatient setting or if the patient has been admitted solely for the purpose of a procedure/intervention only applies to codes in categories U01?U21 and U34?U37 and categories R36-R43. Coding diagnostic imaging using codes from Chapter U Codes in the range U01?U21 and their extended categories U34?U37 are only for use in an outpatient setting, or if a patient has been admitted solely for the purpose of a diagnostic imaging procedure/intervention. Diagnostic imaging of one body area using one method of imaging When one body site alone is scanned and this can be indexed to a code range from U01 U18, U35 or U37 assign the following codes:. Codes from Y97 Radiology with contrast must always be assigned after the codes for the specific scan and before codes from Y98 Radiology procedures. Y97 Radiology with contrast: Codes within category Y97 must only be assigned if it is stated in the patient?s medical record that the imaging procedure has been performed using contrast media. The ?body areas referred to in the codes in category Y98 relate to the following nine anatomical regions of the body. Pelvic region (including all organs in genitourinary system, sacral spine and groin). It is the responsibility of the clinician to provide this level of detail in the source document. Where different methods of radiological imaging are carried out, each method must have a code from Y98 Radiology procedures assigned. It is therefore permissible for more than one code to be assigned from category Y98 Radiology procedures on the same episode of care. Care must be taken when assigning codes for procedures which are performed using a fluoroscopic approach and contrast fluoroscopy scans, as the latter is simply a diagnostic image of a body area. These subsidiary codes must be used if radiopharmaceutical imaging substances are used during a nuclear medicine imaging procedure. Nuclear medicine imaging procedures available in the main body system chapters are B16. Codes from categories Y93, Y94, Y97 and Y98 must not be assigned in addition to the nuclear medicine imaging codes contained within the body system chapters. Where a different agent to thallium is used a code from categories Y93 Gallium-67 imaging or Y94 Radiopharmaceutical imaging must be assigned in addition. Myocardial/Cardiac perfusion scans are carried out in two phases: a stress test and a rest They must be assigned on each consultant episode in which the patient is undergoing rehabilitation. Where a patient receives rehabilitation assessment (X60) and rehabilitation delivery (U50 110 Diagnostic Imaging, Testing and Rehabilitation U54) within the same admission, only one code is required, with that code being from U50 U54, as it is assumed the assessment would have been carried out before the rehabilitation commenced. Examples: Emergency admission for intracapsular fracture neck of femur, treated with closed reduction and fixation using dynamic hip screw.
Buy lipitor no prescription
Are intra-gastric adjustable balloon system [34] Lopez-Nava G test your cholesterol with a simple photo buy cheap lipitor 5 mg line, Bautista-Castano I, Jimenez-Banos A, Fernandezsafe? Dual Intragastric Balloon: Single ambulatory center [28] Genco A, Cipriano M, Bacci V, et al. Intragastric balloon or diet vs intragastric balloon followed by another balloon: a prospective diet alone? Intragastric balloon treatment for [36] Kotzampassi K, Grosomanidis V, Papakostas P, Penna S, Eleftherobesity: prospective single-center study? Please check availability of the product with your local sales representative or your local customer service. Tip Length Catheter Length Number Description (mm) (F) / (mm) (mm) (cm) M00530800 Ultratome Short Nose 20 5. Balloon Length Catheter Size Working Channel Number Description (mm) (cm) (F) / (mm) (mm) M00567330 Max Force Dilation Balloon 4 2 5 / 1. Large storage trays are recommended unless they are to be reprocessed in an Olympus Medivator Machine, into which the large storage trays will not fit. SpyGlass Probes have been validated to 20 cycles of reprocessing without degradation of image. The true number of procedural uses, however, will depend on how the SpyGlass Probe is handled. The 3-Joint Arm with Clamp (M00546070) is useful if the account does not want to purchase the Travel Cart as it allows the account to mount the arm to another cart or table. Length (cm) Number Description Shape (F) / (mm) Barb to Barb M00532870 Advanix Stent Duodenal Bend 7 / 2. Length (cm) Number Description Shape (F) / (mm) Between Pigtails M00532160 Advanix Stent Double Pigtail 7 / 2. Length (cm) Number Description (F) / (mm) Barb to Barb M00539200 Flexima Stent 7 / 2. Catheter Length Recommended Guidewire Number Description (F) / (mm) (cm) (in) / (mm) M00540120 Flexima Nasal Stent 6 / 2. Length (cm) Number Description (F) / (mm) Barb to Barb M00533610 Percuflex Amsterdam Stent 7 / 2. Length (cm) Colour Number Description (F) / (mm) Barb to Barb Code M00532010 C-flex Pigtail Stent 7 / 2. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00537350 Advanix Pancreatic Stent Kit No Pigtail 4 / 1. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00537460 Advanix Pancreatic Stent Kit No Straight 4 / 1. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00536740 Advanix Pancreatic Stent No Pigtail 3 / 1. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00537100 Advanix Pancreatic Stent Yes Pigtail 5 / 1. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00536000 Advanix Pancreatic Stent No Straight 3 / 1. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00536080 Advanix Pancreatic Stent No Straight 3 / 1. Length Number Description Leading Barb Shape (F) / (mm) (cm) M00536450 Advanix Pancreatic Stent Yes Straight 5 / 1. Stiffer stent material compared to 5F pigtail and 5F straight stents with No Leading Barb. Length Length Diameter Length Number Description (mm) (mm) (cm) (cm) (F) / (mm) (cm) M00516900 WallFlex Partially Covered Esophageal Stent 18 23 / 23 10. Number Description (mm) (mm) (cm) (mm) M00514270 Polyfex Esophageal Stent 16 20 9 12 M00514280 Polyfex Esophageal Stent 16 20 12 12 M00514290 Polyfex Esophageal Stent 16 20 15 12 M00514300 Polyfex Esophageal Stent 18 23 9 13 M00514310 Polyfex Esophageal Stent 18 23 12 13 M00514320 Polyfex Esophageal Stent 18 23 15 13 M00514330 Polyfex Esophageal Stent 21 25 9 14 M00514340 Polyfex Esophageal Stent 21 25 12 14 M00514350 Polyfex Esophageal Stent 21 25 15 14 Packaged one per box Recommended Guidewire:. Balloon Length Catheter Diameter Working Length Guidewire Number (mm) (cm) (F) / (mm) (cm) (in) / (mm)** Units M00554500 30 10 14 / 4. Length Dream Tip Number Description (in) / (mm) (cm) Style Units M00556101 Dreamwire Standard. Length Dream Tip Number Description (in) / (mm) (cm) Style Units M00556001 Hydra Jagwire Standard. Length Number Description (in) / (mm) (cm) Tip Style Units M00556481 Jagwire Stiff Shaft. Length Number Description (in) / (mm) (cm) Tip Style Units M00556902 Jagwire Jag Tail. Length Number Description (in) / (mm) (cm) Tip Style Units M00556191 NaviPro Standard. Length Number Description (in) / (mm) (cm) Tip Style Units M00550090 Amplatz Super Stiff Guidewire. Length Number Description (in / (mm) (cm) Tip Style Units H965180011 Wallstent Super Stiff Guidewire. Bands / Number Description (mm) (mm) Ligating Unit Units M00542250 Super 7 Band Ligator 2. Working Channel Length Number Description (F) / (mm) Gauge (mm) (mm) (mm) (cm) Units M00560150 Injection Gold Probe Catheter 7 / 2. Working Channel Length Number Description (F) / (mm) (mm) (cm) Units M00560070 Gold Probe Catheter 7 / 2. Extension Length Length Number Description Design (mm) Gauge (mm) (mm) (mm) (cm) Units M00518151 Interject Sclerotherapy Needle Contrast 1. Extension Length Length Number Description Design (mm) Gauge (mm) (mm) (mm) (cm) Units M00518111 Interject Sclerotherapy Needle Clear 1. Working Length Channel Number Description Gauge (mm) (mm) (mm) (cm) (mm) Units M00511731 Optiflo Hemostasis Catheter 23 0. Working Length Working Channel Number Description Stiffness (mm) (mm) (cm) (mm) Units M00561821 Small Oval Medium Stiff 13 2. Working Length Working Channel Number Description Stiffness (mm) (mm) (cm) (mm) Units M00562691 Small Oval Flexible 13 2. Working Length Working Channel Number Description Stiffness (mm) (mm) (cm) (mm) Units M00562471 Extra Small Oval Flexible 11 2. Working Length Working Channel Number Description Stiffness (mm) (mm) (cm) (mm) Units M00562301 Small Oval Stiff 13 2. Working Length Working Channel Number Description Stiffness (mm) (mm) (cm) (mm) Units M00561221 10 mm Rounded Stiff 10 2. Working Length Working Channel Number Description Stiffness (mm) (mm) (cm) (mm) Units M00562531 Extra Small Oval Flexible 11 1. Working Length Working Channel Number Description (mm) (cm) (mm) Units M00515031 Radial Jaw 4 Hot Biopsy Forceps 2. Working Length Working Channel Colour Number Description (mm) (cm) (mm) Code Units M00513383 Radial Jaw 4 Standard Capacity 2. Working Length Working Channel Colour Number Description (mm) (cm) (mm) Code Units M00513303 Radial Jaw 4 Large Capacity 2. Working Length Working Channel Colour Number Description (mm) (cm) (mm) Code Units M00513343 Radial Jaw 4 Jumbo 2. Working Length Working Channel Colour Number Description (mm) (cm) (mm) Code Units M00513443 Radial Jaw 4 Gastropediatric 1. Working Length Working Channel Colour Number Description (mm) (cm) (mm) Code Units M00510101 Multibite Multiple Sample Biopsy Forceps 2. G-Tube, Right Angle box 5 Length Low Profile Button Replacements Order Length Colour Number Description (cm) Code Units M00568260 18Fr (6. Length Working Channel Number Description (mm) (cm) (mm) Colour Code Units M00515181 Radial Jaw 4 Standard Capacity 1. Sheath Length Number Description (mm) (mm) (cm) Units M00516001 Cellebrity Cytology Brush 2. Working Length Basket Opening Sheath Number Description (mm) (cm) (mm) Material M00513200 ZeroTip Airway Retrieval Basket 0. Indications, contraindications, warnings and instructions for use can be found in the product labelling supplied with each device. Information for the use only in countries with 2017 Boston Scientifc Corporation applicable health authority product registrations. From diagnosis and therapy to documentation, reprocessing, and maintenance, Olympus supports professionals in day-to-day hospital operations with solutions developed hand-in-hand with experts in the feld of gastroenterology. These technologies have been proven in numerous clinical studies to enhance diagnostic and therapeutic quality, save resources, and help to provide greater comfort to patients. Unique, clinically proven technologies, outstanding service, full traceability, and a focus on patient outcomes learn more about the clinical and economic benefits of working with Olympus in this brochure.
Purchase lipitor 5mg fast delivery
These other symptoms are mainly pruitus (66%) hdl cholesterol lowering foods purchase lipitor online now, irritation (25%) and dry scalp (59%). Can give light colored hair, an Tegrin orange tint and treated skin may become more sensitive to sunlight. Treatment Strategies: Synthetic Vs Natural Treatment of dandruff can be done mainly by three ways based on its mechanism of action these include keratolytic, antimicrobial and anti-proliferative agents. It has been observed that only shampooing and keratolytic treatments like salicylic acid is mainly beneficial in patient with milder dandruff condition as it will remove a considerable amount of flakes. These medications are pyrithione zinc, selenium sulfide, Ketoconazole and ciclopirox etc. There are a slew of medicated shampoos that are offered to dandruff sufferers, but many of them contain chemicals or drugs that have risks of their own. Presently in market most common anti-dandruff shampoos are composed of either selenium sulfide or zinc pyrithione. Both selenium sulfide and zinc pyrithione are known as cytostatic agents, which reduces the growth of the outermost layer of skin, in this case on the scalp. The main problem with this therapy is that, they can be very irritating to some people?s skin, and therefore result in making the original dandruff problem worse instead of better. Many synthetic antifungal preparations like coal tar, salicylic acid, miconazole, selenium sulfide, ketoconazole, zinc pyrithione have been tested against many fungal species which causes dandruff, but the frequent infections and the recurrences have made the therapy costlier. Most of the herbal plants or their constituents are made to rubbed on the hair in order to remove dirt and, and it is conceivable that most plants used by man have at some time been tried on the hair. The following are the tabular representations of the outcome of extensive literature survey showing, scientific name, common name (Hindi name), parts used of the plants and their using pattern in hair care with references. There are several research has been showing that, study of natural antifungal especially against Malassezia, Candida albicansare rare and therefore, not much was reported on the same, worldwide. There are several botanicals such as Piper betle, Hibiscus rosa-sinensis, Lawsoniainermis, Datura metal, Mangifera indica, Nyctanthesarbor-tristis, Camellia sinensis, Vitex negundo, Citrusaurantifolia which have been claimed to have antidandruff activity in traditional hair care for the treatment of Dandruff but scientific validation for most plants is lacking. People in India are using botanicals in hair care differently (extracts and oil) and their complex combinations with other ingredient like honey, sugar, milk, water etc. Anti-dandruff activity of ethanolic extract of Sapindus mukorossi seed coat and ficus racemosa fruit peel and in silico protein interaction studies. A simple alopecia scoring system for use in colony management of laboratory-housed primates. Clinical and dermatoscopic patterns of alopecia areata: a tertiary care centre experience. Assessing therapeutic effectiveness of scalp treatments for dandruff and seborrheic dermatitis, part 2: the impact of gender and ethnicity on efficacy. Seborrheic dermatitis: etiology, risk factors, and treatments: facts and controversies. Dandruff / seborrhoeic dermatitis is characterized by an inflammatory genomic signature and possible immune dysfunction: transcriptional analysis of the condition and treatment effects of zinc pyrithione. Effect of ketoconazole 1% and 2% shampoos on severe dandruff and seborrhoeic dermatitis: clinical, squamometric and mycological assessment. Structure of the Hair Chemical Composition of Hair Hair Growth Hair Loss Disorders of the Hair Disorders of the Scalp Hair and Scalp Analysis Copyright 2011 Cengage Learning. The term crowning glory aptly describes the importance placed on hair, how good we feel when our hair looks great, and just how distressing a bad hair day really can be. All professional hair services must be based on a thorough understanding of the growth, structure, and composition of hair. Cosmetologists should study and have a thorough understanding of the properties of the hair and scalp because: You need to know how and why hair grows and how and why it falls out in order to be able to differentiate between normal and abnormal hair loss. Although we no longer need hair for warmth and Epidermis or outer layer of the skin protection, hair still has an enormous impact on our psychology. Hair root Hair follicle A mature strand of human hair is divided into two parts: the hair root and the hair shaft. The Sebaceous or hair root is the part of the hair located below oil gland the surface of the epidermis (outer layer of the skin). The hair shaft is the portion of the hair Arrector pili that projects above the epidermis (Figure 11?1). Hair follicles are distributed all over the body, with the exception of the did you know? The follicle extends Have you heard the expression downward from the epidermis into the dermis (the inner layer of ?You are what you eat? Sometimes more than a healthy diet does not always one hair will grow from a single follicle. Some people refer crash dieting and anorexia can to the dermal papilla as the mother of the hair because it contains cause hair loss, lackluster hair, the blood and nerve supply that provides the nutrients needed for and unhealthy scalp conditions. The arrector pili muscle is the small, involuntary muscle in the dairy products are good sources base of the hair follicle. Strong emotions or a cold sensation cause of these amino acids, as are food it to contract, which makes the hair stand up straight and results combinations such as peanut in what we call goose bumps. It consists of a single overlapping layer of transparent, scale-like cells that look like shingles on Hair Cuticle a roof. The cuticle layer provides a barrier that protects the inner structure of the hair as it lies tightly against Cortex the cortex. It is responsible for creating the shine and Medulla the smooth, silky feel of healthy hair. To feel the cuticle, pinch a single healthy strand of hair between your thumb and forefinger. Next, hold the end of the hair strand with one hand, and then pinch the strand with the thumb and forefingers of your other hand. Part 2: General Sciences Chapter 11 Properties of the Hair and Scalp 221 11 Copyright 2011 Cengage Learning. A lengthwise cross-section of hair shows that although the hair cuticle scales overlap, each individual cuticle scale is attached to the cortex (Figure 11?3). Swelling the hair by applying substances such as haircolor raises the cuticle layer and opens the space between the scales, which allows liquids to penetrate into the cortex. A healthy hair cuticle layer protects the hair from penetration and prevents damage to hair fibers. Oxidation haircolors, permanent waving solutions, and chemical hair relaxers must have an alkaline pH to Figure 11?3 penetrate the cuticle layer, because a high pH swells the cuticle and Hair cuticle layer. It is a fibrous protein core formed by elongated cells containing melanin pigment. The elasticity of the hair and its natural color are the result of the unique protein structures located within the cortex. The changes involved in oxidation haircoloring, wet setting, thermal styling, permanent waving, and chemical hair relaxing take place within the cortex (Figure 11?4). It is quite common for very fine and naturally blond hair to entirely lack a medulla. Chemical Composition of Hair Hair is composed of protein that grows from cells originating within the hair follicle. As soon as these living cells form, they begin their journey upward through the hair follicle. As these newly formed cells mature, they fill up with a fibrous protein called keratin. After they have filled with keratin, the cells move upward, lose their nucleus, and die. By the time the hair shaft emerges from the scalp, the cells of the hair are completely keratinized and are no longer living. The protein is made up of long chains of amino acids, which, in turn, are made up of elements. They are essential to services such as wet setting, thermal styling, permanent waving, and chemical hair Disulfide Sulfur Sulfur bond relaxing (see Chapter 20, Chemical Texture Services). The three types of side bonds are hydrogen, salt, and disulfide bonds (Figure 11?6).