Metoclopramide
Metoclopramide 10mg amex
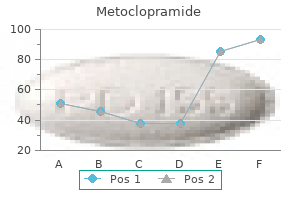
The lead time has a major efect on quanti health systems ties required for safety stocks gastritis diet cure buy generic metoclopramide. In virtually all supply systems, adjustment is necessary for losses caused by The quantifcation method must be chosen in light of the wastage and thef. Quantifcation estimates can be cross-checked by com The consumption method, which uses data on medicine bining diferent methods. No matter which method is consumption, gives in many instances the most accu used, a gap may exist between the initial estimates of rate prediction of future needs. The quantif pharmaceutical supply systems rely primarily on the cation process itself may help justify an increase in the consumption method. To be reliable, the consump budget, but ofen the quantifcation estimates must be tion data must come from a stable supply system with a adjusted and reconciled to match available funds. The relatively uninterrupted supply and a full supply pipe choice between manual and computerized quantifca line. Consumption data may or may not refect rational tion may be dictated by circumstances, but the process prescribing and use of medicines or actual demand for is much easier with computer assistance. This nel and time requirements depend on the quality and method requires reliable data on morbidity and patient accessibility of source data and on the type and scope of attendances (visits to health facilities) and uses standard quantifcation. The goal is to maintain the most cost-efective balance between service levels and Quantifcation is the frst step in the procurement pro inventory costs. In general terms, quantifcation is the process used to determine how much of a product is Major options for quantification required for the purpose of procurement. Proxy consumption method ity, storage space capacity, and capacity to deliver services. Service-level projection of budget requirements Ofen, the terms quantifcation and forecasting are used interchangeably. For purposes of this chapter, forecasting The consumption method uses records of past consump refers to the projection of future needs beyond the next tion of individual medicines (adjusted for stockouts and purchase order. Quantifcation involves The morbidity method estimates the need for specifc estimating the quantities of specifc medicines or supply medicines based on the expected number of attendances, items needed for a procurement. Most quantifcation exer the incidence of common diseases, and standard treatment cises also estimate the fnancial requirements to purchase patterns for the diseases considered (see Section 20. The quantifcation methods described in this 20-1 describes the morbidity method used when a program chapter are normally used to quantify needs for an annual is scaling up. They are not usually used to The proxy consumption method uses data on disease calculate routine order quantities in an established supply incidence, medicine consumption, demand, or use, and/ system that uses scheduled purchasing (periodic orders) or or pharmaceutical expenditures from a standard supply perpetual purchasing (orders placed whenever need arises). The number of patient-months of medicines that can be expected to be consumed from January to April is n(n + 1) P 10 + 20 + 30 + 40 = 100 patient-months. Still, this method may be the best alternative ent types of health facilities in a standard system to project in the absence of suitable data required for the consump medicine costs in similar types of facilities in the target sys tion or morbidity-based method. This method does not estimate quan method is also useful for cross-checking projections made tities of individual medicines. Service-level projection of budget requirements produces Relative predictive accuracy of quantification a rough estimate of fnancial needs for pharmaceutical pro methods curement and not the quantity of products. The method relies on two assumptions: (1) that the standard system Quantifcation of pharmaceutical requirements is inher (used for comparison) and the target system are comparable ently imprecise because of the many variables involved. Despite its limitations, this method In many instances, the most precise method for quan can be useful in predicting medicine costs in a new system tifying pharmaceutical usage is the consumption-based or in a system in which no data are readily available. Table approach, provided the source data are complete, accurate, 20-1 summarizes the applications and limitations of the four and properly adjusted for stockout periods and anticipated major quantifcation methods. This method does not normally address the appropriateness of past consumption patterns, which may or may not correspond with public health pri 20. Tus, irrational medicine use may be perpetuated by total reliance on the consumption method. In many countries, assembling avoid stockouts, emergency purchases, and overstocks valid morbidity data on more than a defned set of diseases and to maximize the efect of procurement funds. The is very difcult; therefore, some needs will be overlooked consumption method is the frst choice, cross-checked to in the quantifcation. Data on patient attendance are ofen assess the appropriateness of usage and demand patterns. Despite proxy consumption method, or both, may need to be these constraints, this method may remain the best alterna applied for an initial quantifcation, switching to the con tive for planning for procurement or for estimating bud sumption method when reliable data can be compiled or get needs in a supply system or facility in which a limited the program has stabilized. Both budget Proxy consumption is the method generally used if neither requests and cuts are frequently prepared without reli the consumption-based nor the morbidity-based method is able estimates of actual needs. This method is most likely to yield accurate pro with rational, well-documented quantifcation. Although jections when used to extrapolate from one set of facili consumption-based quantifcation is the best guide to ties to another set that serves the same type of population probable expenditures, the morbidity-based method in the same type of geographic and climatic environment. Proxy consumption is useful for checking and another country, the results will be only a rough estimate justifying either consumption or morbidity methods. Even when target and standard facilities are closely When budget requirements do not need to be justifed by matched, quantifcation estimates are suspect, because it is specifying order quantities, the service-level method can a big leap to assume that disease incidence, utilization pat be used as an alternative. As local health problems become clear, a to establish funding requirements for procurement and morbidity-based method can be used to project require to develop the initial procurement list. In most situations, ments in the short and medium term, until the regular the consumption-based method is not feasible, and some supply system can resume services. Country Study 20-1 combination of morbidity-based and proxy consumption describes quantifcation for a cholera epidemic. Comparing actual medicine consumption with theoretical Developing procurement quantities for scaling-up programs: need: In most functional supply systems, the regular pro Scaling up is the term used to describe an incremental curement quantifcation is based on past consumption. Patient-months can be used theoretical demand based on public health priorities is a to estimate needs for scaling up, where one patient useful practice. The morbidity-based method provides month is the quantity of a product needed to treat one the most informative comparison, but simply comparing patient for one month. The total number of patients consumption data from diferent systems is worthwhile treated over an incremental period of time in patient because signifcant diferences in medicine use can help months is ofen used in this situation for estimating identify irrational prescribing patterns or persistent needs for chronic conditions. A quan national specialists collected and analyzed data on dis tifcation was carried out to determine pharmaceutical ease incidence and current treatments and developed a supply needs to treat cholera patients. The morbidity method was used to ment through hospitals, clinics, and community health calculate supply needs based on current epidemiological workers were to be covered. The medicines to be included were not accompanying graph illustrates the projected annual sup clear, because average treatment practices were not ply costs for both calculations. Note the huge diference known and standard treatment guidelines had not yet in total costs of the alternative treatment regimens. A team collected data from sample medicine costs were more than two times higher with patient charts and focused surveys to determine current current treatment practices, with the excess almost exclu treatment practices. Fairly accurate used the comparative cost information in educational morbidity data were readily available, reported weekly by activities to improve prescribing practices. However, as in of the availability of medicines in health facilities and most countries in the initial phases of implementing warehouses at any given time.
Buy metoclopramide pills in toronto
If a suppliers problems In addition gastritis weight gain generic metoclopramide 10 mg line, the procurement manager should indicate are sufciently grave, it can be barred for a two-year period in the tender document itself how suppliers ofers will be and then be forced to prequalify again. This step shows all suppliers the importance of Some procurement ofces use a point system, assign the various requirements specifed in the tender. Figure ing values to performance criteria such as those shown in 21-2 shows an evaluation matrix introduced by Papua Annexes 21-1 and 21-2. The relative weights of each cate New Guinea to assess the potential suppliers for pharma gory vary; for example, in some situations, the lead time ceutical tenders. In countries with strong cating that the procurement committee may reject any or regulatory control of the pharmaceutical market, product all bids. Rejection of all bids is justifed when no efective quality may be given a low weight, because all registered competition exists or bids are not substantially responsive. Tese discuss general conditions in Rating systems ofer two options for ranking applica the contract that will be signed with successful bidders tions: in one, a minimum passing score is used; in the and any special conditions applicable to the current pro other, suppliers are ranked from top to bottom overall, curement (see Chapter 39). Ratings will always be subjective to some extent, Specifc pharmacopoeial standards should be listed for so to ensure impartiality, the entire procurement commit each product; if any of a range of standards is adequate tee, or at least a multiperson team, should be responsible for (British Pharmacopoeia, U. This provides a required for a subset of products, this requirement concise description of each product and the quantity should be indicated on the schedule of requirements required, along with any technical specifcations unique (see below), but a generic statement of packaging and to that item. If it can be printed with sufcient space for labeling applied to all products should be included in the suppliers to enter ofers, having suppliers use this space general technical specifcations. Sufcient ing (contents and language) and package inserts can be space should be provided so that the supplier can enter included in the technical specifcations, unless specifc all relevant information, including the name of the origi requirements exist for a subset of products. If diferent instruc component, the basic unit (tablet, capsule, vial, bottle), tions apply to certain products, they should be stipulated the package size, and the number of packages needed. Some tenders list both the total number of packages 21 / Managing the tender process 21. The Receiving and opening tender offers tender should specify whether the listed package sizes are the only ones acceptable; some procurement agencies To ensure confdentiality and to avoid accusations of price request ofers on all package sizes available. It can also be helpful menting the date received and the person who received the in making sure that all parties are referring to the same bid. The unopened bids should be stored in a locked, secure item when clarifying issues with client facilities or with area until the closing date. For therapeutic category analysis, a supple also be entered into the procurement management informa mentary code can be used to assign each drug product to tion system to track the response to tenders. With At the specifed date and time, the bids should be formally a computerized system, developing a catalog is simple; opened, with at least one member of the procurement com updating a product catalog manually is more difcult, mittee and bidder representatives (if they choose to be pres but the efort may be worthwhile to save time in compil ent) in attendance. Details such as the bidders name and address, and required documentation such as bid 21. If the bid security has not been deposited, an imme The most important aspect of adjudication is that it is an diate disqualifcation usually results. Collating offers for adjudication Preparing during the open period The frst step in collating ofers is to determine which ofers, The length of the open period (time between the invitation if any, are nonresponsive to tender conditions. Suppliers that to tender and the closing date) typically varies from four to have not met the basic requirements related to bidder quali eight weeks. A longer open period lengthens the total lead fcation, medicine description, strength, pack size, qual time for obtaining pharmaceuticals but may also increase ity requirements, and delivery date are nonresponsive. The procurement agency required information has not been provided, the bid is non should prepare for receipt of documents, collation, and responsive. If the tender documents require the suppliers adjudication during the open period. If clarifcation is needed in an adjudication report to allow side-by-side comparison because of a mistake or omission in the tender package, it of the ofers. Nonresponsive bids should not be entered into should be provided to all participating bidders. Similarly, if the collated adjudication report, but the problems should be one supplier is given approval to ofer a product or pack documented in writing for review by the procurement com age that is similar to but not the same as that listed in the mittee. If the primary/secondary supplier system is ered in the adjudication, the adjudication report should sep used, equal care is needed in selecting secondary suppliers, arate ofers eligible for the local preference margin, so that because they will automatically be used if the primary sup they can be fairly compared with ofers that are not eligible. Spreadsheets are now commonly used to simplify the col Written bid evaluation criteria should be applied rigor lation of information and the preparation of an adjudication ously and without exception. In addition, specialized procurement sofware is awarded to the lowest bidder that has the capacity to sup available that automates all of the processes related to col ply products that meet the standards required (considering lecting bids, collating ofers, and ranking them according local preference, if applicable). Figure 21-3 datory unless the lowest bidder has not performed in prior illustrates an adjudication report prepared by a specialized procurements. Delivered price, which includes landed cost, overheads, and proft margin, is more common and is an The authority to adjudicate tenders and award contracts adequate standard for comparing costs. Letters of credit are should be confned to the procurement committee (or gov normally not used to pay local suppliers; other mechanisms, ernment tender board). Procurement ofce staf should such as deferred payment, may be benefcial and should be assemble information for the tender board or procurement considered if stated in the evaluation criteria and in instruc committee and make technical recommendations, but they tions to bidders. When the health procurement agency sells should not have a vote in the contract decision. For exam and transparent, with written rules for the process, including ple, if health facilities are given thirty days to pay, then thirty evaluation, award, any special criteria, and the appeal period to-sixty-day payment terms to suppliers can help cash fow. For restricted tenders that do not the required date, then the efect of a shortage must be con involve split contract requirements, this process can be sidered in light of the cost of alternative treatments or of a quick. The procurement committee reviews the collated bid special air shipment to cover the interim period. Disqualifcation of such as a local preference margin calculated by adding a per low bidders should be documented and become part of the centage to the value of foreign bids, before they are compared tender record. Although pricing is the accepted a tender evaluation committee is formed for ranking the means of granting local preference, some countries have bids according to standard evaluation criteria, and then more explicit requirements to grant local companies prefer beginning the postqualifcation supplier evaluation process. This When the postqualifcation analysis has been completed, approach, however, can put the procurement ofce at risk of the procurement committee meets to review the recom having to accept lower local standards of service or product mendations of the tender evaluation committee and deter quality. In any event, all procurement agencies should use mine whether the lowest evaluated bid should receive the supplier performance as the basis for purchasing decisions. If not, the next-lowest evaluated bid is considered, Some programs try to maintain as broad a supplier base and so forth. Some countries sarily well protected, and the laws of that country may not allow an appeal period during which rejected suppliers may safeguard the goods. This fact does not alter the fact that request reconsideration by the tender board. The appeal the seller should be responsible for ensuring that the goods process varies greatly according to national regulations; the arrive. No guarantee exists that the courts of the country time to resolve appeals according to law may be less than a selected will agree to adjudicate any case that arises, but if week or many months, but ideally, the appeal period should the choice has been a commonsense one, it will probably be be no more than one month, to avoid delays in procure respected. Ultimately, the other bidders should be notifed and An alternative is to indicate some other body to settle given information about the winning bid. In commercial contracts with some countries, the chamber of commerce may be asked to act as arbitrator. Finding a suitable arbitrator who is When tender awards are made, contracts must be estab fair, sufciently expert in the feld concerned, and trusted by lished with successful bidders (see Chapter 39). A list of all contracts awarded, specifying for each item the One word of warning: international disputes are ofen supplier, price, and total value, should be made available to not efectively settled by the courts, or even by arbitration. The supplier can change its name, address, domi primary/secondary system, the secondary supplier is con cile, and legal or corporate form and be out of reach of the tacted immediately. Even between industrial depending on the volume, local competitive bidding may be ized countries with a long history of personal-injury litiga the preferred method. Almost all procurement laws and regulations are based on previous laws developed in and for the country, although 21. With more people and goods moving from The procurement ofce is responsible for monitoring per one country to another, questions about which system of formance and compliance with contract terms by suppliers law applies ofen arise. The ofce must Department of Tanzania signs a contract to buy medicines actively track suppliers lead time, delivery status, compli from France, will the agreement fall under Tanzanian law ance with contract pricing and terms, shelf life, and pack or French law
Discount metoclopramide 10 mg on line
The United States Government Global Health Initiative Strategy 1 (4) Innovate for results: Introducing gastritis diet ���� order metoclopramide with a mastercard, evaluating and, where appropriate, scaling up new interventions and approaches that have shown promise in small studies. This increase is comparable with progestagens, have been increasingly used in combination the effect on breast cancer of delaying menopause, since with oestrogens. Studies were identified from review articles, literature searches, and users was greater for women of lower than of higher weight discussions with colleagues. There was no marked variation in the studies were invited to take part in the collaboration. All results according to hormonal type or dose but little collaborators were then sent a list of studies and key references information was available about long durations of use of and were asked if they knew of additional studies, published or any specific preparation. Of the 63 eligible studies identified, original data were *Collaborators and analysis and writing committee listed at end of contributed by 51, 49 published1-49 and two unpublished. Prospective studies were included by Total 22189 (42%) 45181 (42%) means of a nested case-control design in which four controls Natural menopause 18755 37623 were randomly selected for each woman with breast cancer and Bilateral oophorectomy* 3434 7558 similar data were sought for each case and control. The method Hysterectomy before menopause 5539 (11%) 12368 (11%) of selecting controls has been described elsewhere. Consistency and comparability of data Table 1: Distribution of cases and controls according to Many consistency checks were made. Apparently inconsistent, menopause category implausible, or missing data were clarified and, where possible, rectified by correspondence. Women reported to be perimenopausal and Details of the study design, methods of data collection, and those who had undergone hysterectomy without bilateral the participants in each study included in previous reports by the oophorectomy before the natural menopause were also classified Collaborative Group have been summarised elsewhere. If less than 2 years had elapsed between the date of within 12 months of the diagnosis of breast cancer (or of last contact and the date of diagnosis/pseudodiagnosis, variables pseudodiagnosis for controls). Where possible, the preparation used most by diagnosis/pseudodiagnosis, who were assumed to be each woman was ascertained and women were grouped premenopausal. Information on tumour spread was available for 21 Use of these simple stratified O1E values in preference to more studies1,4,7,13,14,16,17,21,25,28,33-35,37-39,43,45,46 (and two unpublished studies), complex mathematical models sacrifices a little statistical power and for those, women with invasive breast cancer were further but has the advantage of avoiding assumptions about the precise classified according to tumour localisation (localised to the breast forms of any relations in the data. The stratified O1E values, or spread beyond the breast), by means of criteria described together with their variances and covariances, yield both elsewhere. Relative-risk and age at menopause were defined as consistently as possible estimates were obtained from O1E values by the one-step across studies. All cyclically at around the time that her breast cancer was diagnosed relative risks are presented without further modification, but (or at pseudodiagnosis for controls) and, if not, her age when when more than two groups were compared, the variances were cyclical ovarian function was likely to have ceased. Women who estimated by treatment of the relative risks as floating absolute were reported to be still menstruating at the date of risks. Women were classified as post valid comparisons between any two exposure groups, even if menopausal if a natural menopause or cessation of menstruation neither is the baseline group. Any comparison between groups because of bilateral oophorectomy or irradiation of the ovaries must take the variation in each estimate into account. Women reported to be perimenopausal and those To ensure that women in one study were compared directly who had undergone hysterectomy without bilateral with similar women in the same study, all analyses were routinely oophorectomy before the natural menopause were classified in stratified by study, by centre within study, and by fine divisions separate categories. Most of the women were premenopausal (40%) or postmenopausal (42%); a small proportion were perimenopausal (2%), and 11% had undergone hyster ectomy without bilateral oophorectomy before the natural menopause (table 1). Of postmenopausal women, 84% had had a natural menopause and 16% bilateral oophorectomy. The median age at natural menopause was 50 years; 77% of women reported that their age at menopause was between 45 and 54 years. The median age at bilateral oophorectomy was 44 years (between the ages of 35 and 49 years in 68%). The relation *Relative to premenopausal women, stratified by study, age at diagnosis, parity, and the age a woman was when her first child was born. The position of the square indicates the value of the relative risk, For women of a given age, age at menopause also and its area is inversely proportional to the variance of the defines their time since menopause, and so the relation of logarithm of the relative risk, thereby providing an indication of breast cancer risk with time since menopause is the the amount of statistical information available for that particular inverse of its relation with age at menopause (figure 1b). The precise stratification and method used to calculate variances are specified than premenopausal women of the same age and for each plot. This trend did not carried out in North America or Europe, although 21 differ significantly between women with a natural countries are represented. The risk of breast cancer in perimenopausal oophorectomy (46%) than among controls who had women relative to that of premenopausal women of the experienced a natural menopause (22%). A womans year of birth of these women was 1925 and the median relative weight can also confound such a relation, since year of diagnosis/pseudodiagnosis was 1985. Since the trends according use was 48 years, and 96% of users started use before age to time since menopause are similar for natural 60. The median age at last use was 53 years, and 92% of menopause and bilateral oophorectomy, these are not users stopped use before age 65. Figure 5 shows the results by duration of use separately for to the median year of diagnosis of breast cancer. These three indices are more years before diagnosis/pseudodiagnosis, there was correlated, so if the risk is directly related to any one no significant overall increase in the relative risk of breast factor it may be indirectly related to the others. Information about the hormonal constituents Last use within 5 years before diagnosis includes current users. None of these breast cancer according to the type or the dose of factors changed the pattern or the magnitude of the oestrogen used mostly and no evidence of marked results shown in figure 5. This finding may be due There was no marked variation in these main findings to chance, especially since the category showing the across different studies (data not shown). In figure 6 the highest relative risk (oestrogen and other, or other), is a consistency of these main findings is examined for various heterogeneous group that includes users of various subgroups of women, even though analyses restricted to unrelated compounds, none of which is individually the particular subgroups may, by chance alone, yield cause of the raised relative risk. Three Information on the extent of tumour spread was available different assumptions were made about their possible age for 9668 (54%) of the postmenopausal women with at menopause: first, that it was the same as the median breast cancer. These menopause is such an important confounding factor, relations did not differ significantly between women with inclusion of women with unknown values in the main a natural menopause and women with a bilateral analysis would be inappropriate. The increase in the the cessation of cyclical ovarian hormone production at relative risk of breast cancer among current or recent users the menopause. Although circulating oestradiol was greater for women of low than for those of high concentrations are an order of magnitude lower in relative weight. The reduction in circulating hormone cancer, the large amount of information assembled for this concentrations at the menopause therefore seems to lead collaboration allowed detailed analysis of the relation within 5 years to a reduction in the relative risk of between this risk and the timing of menopause. For example, there was some evidence have low oestradiol concentrations after the menopause. They constitute chance alone, show significant associations and others about 18% of the study population and their inclusion would not. The data included represent about 90% of the available Failure to stratify by body-mass index could also lead to epidemiological evidence on the topic.
Cheap metoclopramide 10 mg overnight delivery
Its inspired countries and reminded them that they have the capacity to generate local solutions while meeting international benchmarks gastritis diet advice cheap 10mg metoclopramide mastercard. According to Millar, We have a long way to go to reach elimination and we have to stay focused to reach that deadline, or this will all have been for nothing. Effects: Visual impairment, blindness Source: Adapted from the Community Eye Health Journal. The prevalence of trachoma based on existing information, recent population-based prevalence surveys. The availability of sufficient program resources to continue treatment until such time as elimination is achieved. All components must be addressed in order to successfully apply for the drug donation and sustainably eliminate blindness from trachoma. Making plans to inform and gain the support of the community to be treated through appropriate health education and social mobilization activities. Shares information (programmatic and technical) about developments in trachoma control 4. Number of districts for which baseline mapping is completed Baseline prevalence surveys Output 1 2. Number of surveyors and analysts trained for survey Output 2 trained collection 1. Number of steering committee members actively Effective programme engaged in decision making Output 3 management structure 2. Number of implementing agencies actively mapping established and maintained trachoma 3. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Consistent, high u Training resources for: quality outputs u Standardized guidelines u Planning 3. Data security and u Scientific oversight u Training accessibility u Data stewardship u Fieldwork 4. MoH ownership of u Data quality control u Results data and results u Technology (web & mobile) 5. Exhibit 19 Global Trachoma Mapping Project Results, October 2015 Mapping Goal: Total: 1,805 districts Mapping Mapping incomplete complete due to insecurity Total Districts 1531 296 Districts in Africa 1,176 153 Districts in Mediterranean, 355 143 Asia, Pacific, and South America Source: Global Trachoma Mapping Project. Elimination Reduction to zero of the incidence of a specified disease in a defined geographical area as a result of deliberate efforts; continued intervention measures are required. In the case of trachoma, elimination would be the reduction of cases of blindness from trachoma to zero. Eradication Permanent reduction to zero of a specific pathogen, as a result of deliberate efforts, with no more risk of reintroduction. Implementing Implementing agencies worked at national or subnational levels to ensure agency that the infrastructure, trained staff, transport and supervision were in place to deliver training and mapping. Implementing partners were responsible for creating budgets for mapping activity and seeking approval from Sightsavers and the technical team. Kappa statistic Cohens Kappa is a statistical coefficient that measures agreement between two sets of measurements for categorical items. Mass drugthe administration of drugs to entire populations to control, prevent, or administration eliminate a disease. Population-basedthe gold standard for estimating the prevalence of trachoma within a prevalence survey target population. The most commonly used population-based survey design for trachoma prevalence estimation is cluster random sampling. It stands for Surgery, Antibiotics, Facial cleanliness, and Environmental improvement, which are methods used in combination for trachoma elimination. It clearly documents the project requirements, milestones, deliverables, and end products that are expected. Tetracycline A broad-spectrum polyketide antibiotic, often administered as a topical ointment used to treat active trachoma. It was the drug of choice for treating active trachoma until the discovery of azithromycin. Trachoma Atlasthe Atlas aims to consolidate published and unpublished data at the district level and provide up-to-date country maps of trachoma distribution on an open-access platform. Vector-borne Vectors are living organisms that can transmit infectious diseases between transmission humans or from animals to humans. As early as 1796, physicians recognized the efficacy of using cowpox to protect against smallpox infection. John Clinch introduced the smallpox vaccine in Trinity, a small coastal town in Newfoundland, Canada. A heat-stable, one-dose vaccine was developed for smallpox and40 administered en masse cheaply and effectively. The arrival of the vaccine heralded the beginning of41 worldwide vaccination and prevention efforts, but distrust in the vaccination and high indigenous population prevalence stifled coverage. As a result, smallpox was eradicated throughout much of the developed world, but pockets of the disease persisted in developing countries and in underserved populations, especially indigenous peoples. The smallpox eradication campaign celebrated its eradication41 goal on May 8, 1980 at the 33rd World Health Assembly. Though onchocerciasis primarily affects rural populations, in Africa,44 the disease has been found to cause serious socio-economic problems; populations have in the past abandoned fertile land along the rivers whilst persons with unsightly lesions have been socially marginalized. After working exclusively on vector control for many years using larvicide (killing black flies that carry the parasite), in 1987 Merck & Co. However, it determined the disease could be controlled to the point that it would not pose a risk to public health. Little was invested in developing new tools for disease control, and heavy reliance was been placed on the distribution of Mectizan. According to Basanez et al, annual [Mectizan] regimes are not considered sufficient to achieve local elimination of parasite populations, unless very high therapeutic coverage (more than 80 percent of the total population) is achieved for at least 25 years without loss of treatment efficacy. The disease is characterized by emergence of the worm, up to a meter long, from lesions on the legs or arms after a year of incubation and mating inside the abdomen. Guinea worm disease usually is not fatal but causes extreme pain at the lesion site and, in some50 cases, permanent disability. Their strategy was to work with ministries of health to52 prevent the spread of disease by providing health education and helping maintain political will in affected areas. Specific interventions aimed at increasing access to safe drinking water and health education and community-involvement. After a village was identified to have Guinea worm,53 an individual was designated to supply monthly reports of Guinea worm cases. In 2015, only 22 cases of Guinea worm were reported (in Chad, Ethiopia, Mali, and South Sudan). Insecurity continues to be a problem for the Guinea worm campaign in areas of South Sudan and Mali. The three areas of focus are grouped under the acronym due to their interrelatedness and importance to international development and global health as a whole. Despite this, integrating strategies to18 address both has proven difficult, as most organizations address only one of the two.
Diseases
- Pelvic dysplasia arthrogryposis of lower limbs
- Leukoplakia
- Creeping disease
- Disorder in the hormonal synthesis with or without goiter
- Mucopolysaccharidosis type II Hunter syndrome- severe form
- Microphthalmia
Buy metoclopramide 10 mg without prescription
Key to the history is a detailed description of pain including onset gastritis diet ideas order metoclopramide visa, precipitating and palliating features, quality, radiation, severity and timing. A pain diary can be helpful to elucidate pain pattern and features and there are many available online (See. The general approach to the workup of pelvic pain in transgender men is similar to that for non transgender women. An anatomic approach to history gathering that considers urological, gynecologic, gastrointestinal, musculoskeletal, and psychological components is critical. Specific etiologies may be multifactorial, such as post-surgical adhesions with or without gastrointestinal symptoms, or endometriosis and/or pelvic floor muscle dysfunction. It is also critical to assess quality of life impact and determine what the patient would consider a favorable outcome. Most evaluation and treatment guidelines stress that chronic pelvic pain can be a diagnostic and therapeutic challenge, and success will depend on comprehensive and customized evaluation and multidisciplinary care. Specific behavioral etiologies to consider include: depression, history of emotional trauma (including sexual assault or abuse, adverse childhood events),[4] and post-traumatic stress disorder. The use of testosterone has a dose dependent effect on vaginal tissue by inducing a hypoestroenic state which promotes atrophy, increases vaginal pH and thus increases increases the risk of vaginitis and cervicitis. Additionally, transgender men may have decreased access to or utilization of screening and therefore treatment for cervicitis and sexually transmitted infections. Transgender men who have pelvic pain after hysterectomy but have retained one or both ovaries/gonads should be screened for a gonadal pathology. The interaction between a genotypic female skeleton and increased muscle mass as a result of testosterone therapy may result in changes in postural carriage. Additionally, recent and/or history of sexual trauma may be exacerbated among those with gender minority status. Engaging with medical June 17, 2016 60 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People professionals can be re-traumatizing in this setting; in all cases a trauma informed approach should be taken. Also assess for use of pain medication, and any association with testosterone dosing cycles. A comprehensive sexual history, including assessing for specific behaviors with other individuals such as (vaginal-vaginal), vaginal or anal or receptive penile sex, recognizing that many transgender men may engage in receptive vaginal sex. A surgical history should note for history of an open, laparoscopic or vaginal approach to inform suspicions of scar tissue and adhesions and subsequent symptomatology. Other history should include screens for adverse childhood events, current domestic violence, and for substance use and overuse, including tobacco. Physical exam On exam assess for involvement of various abdominopelvic organs, including a check for costo vertebral angle tenderness, palpation of the abdominal wall, noting any particular tenderness along prior surgical scars or point tenderness along scars or the abdominal wall in general. Palpate the bladder for localized sensitivity, and palpate the abdomen for visceral organ involvement. Consider a speculum exam only if clearly indicated, noting vaginal discharge or any evidence of vaginitis, and assess the general condition of vaginal tissues and the cervix. If a bimanual exam is performed, note any cervical, adnexal or ovarian tenderness to palpation. Also if indicated consider a rectal exam, noting masses, tenderness, or hardened stool. A pregnancy test should be considered, however some patients who are not sexually active with someone capable of insemination may be offended by the suggestion of this test. It is best to explain to patients in advance that this test is part of a standard protocol, and if it is certain that pregnancy is not possible based on sexual behaviors, a pregnancy test may be omitted. Imaging should be performed using transabdominal or transvaginal ultrasound; in those men who have had a vaginectomy, a transrectal ultrasound may be an option. Some transgender men may decline vaginal ultrasound and/or bimanual exams due to potential exacerbation of gender dysphoria. In these cases proceed with an abdominal exam as well as laboratory and transabdominal ultrasound for the initial workup. June 17, 2016 61 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Specifically for transgender men, critical components of the assessment include timing of pain and associated symptoms in relation to initiation of testosterone therapy, moliminal timing (symptoms in relation to an expected menstrual cycle) even in the presence of amenorrhea, and a detailed history of prior surgeries and related organ inventory. Testosterone-induced dyspareunia, vaginitis, and cervicitisthe use of testosterone often results in estrogen deficient, atrophic vaginal tissues akin to a post menopausal state in cisgender women. Symptoms are often described as rough sand-paper and burning or dry vaginal irritation. Visual inspection consistent with atrophy will demonstrate thin pale tissues, a loss of rugae, loss of elasticity, friability, and dryness. Interstitial cystitis should be considered when infectious causes have been rules out and symptoms localize to the urinary bladder. Vaginal estrogen to treat underlying atrophy may be warranted and a short course may be successful in restoring comfort. Patients may be reassured that vaginal estrogen is associated with mnimal systemic absorption and should not interfere with the desired effects of Testosterone. Other therapeutic approaches may include vaginal lubricants or vaginal moisturizers. In one cross sectional study 20% of respondents had a hysterectomy to decrease post-testosterone cramping and another 22% to stop extreme bleeding and cramping. These conditions may be simultaneously present in up to 35% of non-transgender female patients with chronic pelvic pain. Conversely, pelvic pain and living with a chronic pain condition may result in depression. These symptoms may be even greater in transgender men for whom examination of genital and reproductive organs may be particularly challenging and triggering of June 17, 2016 62 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People gender dysphoria, and result in avoidance of pelvic exams. Role of hysterectomy In addition to non-surgical approaches, in some cases hysterectomy may have a role in the management of pelvic pain. Depending on the preferences and reproductive goals of an individual patient, gynecologists may revise their therapeutic approach to consider hysterectomy earlier than they might in non-transgender women (Grading: X C S). At the same time hysterectomy should not be viewed as a cure-all, and in some cases is not effective in improving pain. For this reason, transgender men with pelvic pain must be evaluated on a case-by case basis due to the lack of evidence-based guidance at this time. Decision to perform oophorectomy should be based on the etiology of pelvic pain, presence of comorbidities, future fertility desires, and any future plans to stop taking testosterone. Management of specific symptoms and syndromes If pain is vulvar and there are no identifiable lesions or infections, Consider the use of topical 2-5% topical lidocaine placed on soaked cotton-ball and left in the vestibule overnight for general pain relief, or for 30 minutes prior to sexual activity as desired. If pain is vulvar and exam is consistent with vaginal atrophy in the setting of testosterone administration, consider a short course of vaginal estrogen in doses and administration similar to that used for post-menopausal non-transgender women. Patients who are uncomfortable with intravaginal use may be instructed to place treatment cream on their external genitalia. Choice between tablets, creams, and rings depends on patient preference and formulary considerations. If pain is abdominal, present in the abdominal wall or associated with abdominal scar tissue, consider treatment with 1% lidocaine instilled at trigger points in repeated administration. If transvaginal ultrasound is required, consider a low-dose benzodiazepine such as lorazepam 0. Some patients may feel safer and more comfortable placing the ultrasound probe intra-vaginally themselves. June 17, 2016 63 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Introduction: Persistent menses & unexpected vaginal bleeding Many transgender men chose not to undergo hysterectomy, oopherectomy and/or gender-affirming genital procedures. For those transgender men using physiologic doses of testosterone, cessation of menses is expected, typically within 6 months. Cessation of menses is driven by a combination of testosterone induced ovulation suppression, which may be incomplete, and endometrial atrophy. Factors that affect time to cessation of menses likely include: dose of testosterone, route of administration, frequency of testosterone administration, presence and functioning of ovaries, body habitus, and the presence of other structural or non structural medical conditions of the uterus or ovaries. Transgender men with a history of abnormal cycles prior to initiating testosterone. Therefore in patients with risk factors for endometrial hyperplasia and a degree of clinical suspicion, evaluation for and elimination of known causes of irregular bleeding should be considered concurrent with testosterone administration; those with pre-existing amenorrhea or oligomenorrhea may require evaluation for endometrial abnormalities prior to initiating testosterone. This includes ruling out pregnancy in transmen who are sexually active with partners who produce sperm. Despite prior suggestions that endometrial cancer risk may be increased in transgender men on testosterone,[25] longer-term data do not support this risk.
Order metoclopramide 10mg otc
A certain amount of wastewater from bathing gastritis diet effective metoclopramide 10 mg, kitchen, and laundry activities will be generated in the community, both at the individual and community level. This greywater can pose a danger to public health if not properly disposed of in a soakage pit, or allowed to drain away from the settlement. In some cases and with certain precautions, greywater may be reused for vegetable gardens or to flush latrines. Treatment Water may contain pathogens, particularly certain viruses, bac teria, protozoal cysts, and worm eggs. These organisms may be transmitted to water by feces, and may be ingested when water is consumed, potentially causing disease. Although water con tamination by human feces is the major concern, animal feces in water may also transmit disease. Water contamination by human urine is a significant threat only in areas where typhoid and urinary schistosomiasis (Schistosoma haematobium) are endemic. By far the greatest risk associated with polluted drinking water is infection with a variety of organisms that cause diarrheal diseases, as well as typhoid and infectious hepatitis (hepatitis A). The numbers of viruses and protozoa in water will always decrease over time, with the most rapid decrease occurring at warm temperatures. Bacteria behave similarly, but in exceptional circumstances they may multiply in polluted water. The infectious dose of viruses and protozoa is typically very low, whereas the dose of bacteria needed to establish an infection in the intestine may be high, as in the case of cholera, or extremely low, as in the case of the shigella dysentery organism. Simple and practical measures, however, can be taken before such help is available. In addition to protecting water at its source, five basic methods can be used for water treatment: storage, sand filtration, coagulation and flocculation, chemical disinfection, and boiling. Storage Leaving water undisturbed in containers, tanks, or reservoirs improves its quality over time. Storage allows pathogens to die off and suspended particles to settle through sedimentation. If water supplies are unsafe and cannot be easily treated, immediate action must be taken to provide maximum water storage capacity. Storage of untreated surface water for 12 to 24 hours will considerably improve its quality; the longer the period of storage and the higher the temperature, the greater the improvement. In addition, the clarification of turbid or cloudy water can be greatly speeded by the addition of aluminum sulfate (alum). A two-tank system is often used, with the first tank used as a settling tank and the second used to store the clarified water. Further treatment can be done in the second tank as well, and a third tank used for storage, if necessary. While clear water may only require chlorination, turbid surface water will usually require sedimen tation and/or filtration before chlorination. Organic matter that causes turbidity reduces the effectiveness of chlorine by reacting with and dissipating chlorine, and also makes it much more difficult for chlorine to maintain necessary contact with microorganisms. This task can be done by covering storage tanks and screening all inlets into them. In addition, the area where storage tanks are located should be fenced off and guarded to prevent children from playing or swimming in the tanks. Rapid sand filters, which are suitable for low turbidity waters, operate either by gravity flow or within enclosed pressure vessels. Both methods employ relatively complex backwashing operations to remove suspended particles captured on the filters. The schmutzdecke breaks down a large percentage of the bacteria, viruses, and protozoans found in polluted waters, while the sand layers filter out additional organisms, along with suspended sediments and particulate matter. In general, the slower the rate of filtration, the higher the quality of the water. A packed drum filter can be used for sand filtration and is a good way of providing limited quantities of safe water quickly. In a packed drum, filter water passes down through layers of sand and gravel and is drawn off at a rate not to exceed 60 L per hour for a 200-L drum. Unfiltered water equal to the amount drawn off is continually added to the top of the drum. Other types of sand filters include horizontal sand filters and riverbed filters (suitable only where the riverbed is permeable). These methods can be used to treat larger amounts of water but are likely to be more difficult to set up quickly and effectively. This water must still be considered river water, and though it will have been filtered through the bed and bank, further treatment may be necessary. Coagulation and Flocculation Because chlorine and other forms of chemical disinfection do not work well in highly turbid waters, coagulation and flocculation is used to clarify water through the addition of aluminum sulfate (alum). Over time, particles begin to stick together in the flocculation process, eventually forming clus ters of larger particles that are removed by sedimentation and/or filtration. Chemical Disinfection Chemical disinfection kills pathogenic organisms and is the final stage in the water treatment process. This type of dis infection is most effective when used to purify relatively clear water or to disinfect wells, sand filters, pumps, and piped water systems. Various forms of chlorine can be used as well as iodine, although chlorine is more widely used, cheaper, and often more readily available. Chlorine gas, which is normally used in large conventional water treatment systems, is highly corrosive and should not be used in emergency situations except under extremely unusual circumstances. Expert advice is essential for large-scale chlorination, and all systems using chlorine products must be given close attention and regular maintenance. Chlorination generally occurs after sedimentation and filtration, if these processes are needed. At least 30 minutes contact time is needed for chlorine to react with and kill microorganisms. Water should be tested for chlorine residual levels after each disinfection and before distribution. Chlorine should be added to the water until the free available chlorine reaches approximately 0. Highly polluted waters will require greater doses of chlorine than relatively clean waters. The amount of free available chlorine remaining in the water should be no more than 0. Tablets, however, may be useful to treat water in health facilities or supplementary feeding centers. Certain new technologies for home-based water treatment such as individual bottles of chlorine, individual packets that both flocculate and disinfect water and small portable filtration units are currently being used on a limited basis, and are under investigation and trial application to evaluate their suitability for emergency use. The biggest obstacle to their effective use is the difficulty of implementing programs requiring substantial change in human behavior during acute stages of emergencies. Boiling Boiling is the surest and perhaps simplest method of water sterilization but is practical only for small displaced popula tions. At low altitudes, bringing water to a boil for 1 minute will essentially destroy all pathogens transmitted by drinking water. Boiling times, however, must be increased by 1 minute for every 1,000 m of altitude above sea level, as the temper ature at which water boils decreases with altitude. To improve taste, allow the water to cool, and then pour the water from one clean container to another several times. Boiling increases the concentration of nitrates, which are dangerous for very young babies. Care must be taken not to use the boiling option for babies drinking water when using ground water sources that potentially contain elevated nitrate levels. Prolonged vigorous boiling is often recommended but not necessary to destroy fecal-oral transmitted pathogens. In general, boiling is not suitable for camp situations if the energy source is firewood, which is likely to be in short supply. The availability of domestic fuel supplies may be the determining factor, as boiling requires about 1 kg of wood per liter of water. If the displaced people have traditionally boiled their water, however, they should be encouraged to do so. Nutrients Foods are made up of five basic types of nutrients: carbo hydrates, fats, proteins, vitamins, and minerals.
Cheap 10mg metoclopramide with amex
Transmasculine peoples vocal situations: a critical review of gender-related discourses and empirical data gastritis diet karbo buy 10 mg metoclopramide free shipping. Evaluation of a consecutive group of transsexual individuals referred for vocal intervention in the west of Sweden. Endocrine therapy for transgender adults in British Columbia: suggested guidelines. June 17, 2016 171 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 35. Health insurance coverage issues for transgender people in the United States Primary authors: Andre A. The burden of fighting against this level of adversity when people are physically ill or injured represents a significant barrier to care. This adversity has contributed to the high incidence of transgender people avoiding seeking needed health care. These are health benefits plans and are not insurance plans strictly speaking, although they may appear the same to the enrolled member. Most carriers have now issued their own internal guidelines specific to transgender-related healthcare, especially surgical interventions. These guidelines (called by various names such as medical policies or coverage positions) spell out what services will be covered for a specific medical condition June 17, 2016 172 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People and usually apply to all insurance products issued by a carrier. Thus, what is covered by a given health plan will vary not only by state but also by employer. These large employers have chosen to implement medical guidelines that offer increased access, such as coverage of a greater range of medically necessary services. Smaller businesses, which depend on the insurance company to assume the risk (and whose risk is combined with other small employers), may not have the leverage to negotiate inclusion of transgender health benefits. However, smaller employers can inquire with their carrier representative as to feasibility and per-member, per-month costs of doing so, since coverage is becoming increasingly common across the country. Gaining coverage: changing the paradigm From the 1960s through the 1990s, some very persistent Individuals, often with support from their health care providers, were able to secure benefits payments, in certain instances. However, systemic reform did not begin until the 2000s, after advocates were able to convince the City & County of San Francisco to eliminate exclusions in at least one of the five plans City & County employees could select from for their health care coverage. Utilization data from the first five years showed that there was little or no increase in plan cost when medically necessary gender-affirming care was included in a large group plan. Department of Health and Human Services issued a ruling that Medicares longstanding exclusion of transsexual surgical procedures was no longer valid, leaving the provision of services up to local coverage determinations. If there is no provision for transgender care in this instance, it will be necessary for the provider to appeal to the carrier for coverage of the specific treatment or diagnosis. Overriding a sex mismatch: condition code 45 All federally-funded health institutions. However, the code may not have been implemented by all hospitals or carriers systems; in these cases using Code 45 may result in a returned claim for correction, or outright denial of the claim. Many more never receive a formal denial because their plan contains transgender specific exclusions and the physician never files paperwork for prior authorization for such services. Many call their insurance carrier and are told services will not be covered, and on that basis never attempt to file a claim. Transgender individuals and their health providers June 17, 2016 174 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People should be aware that unless a denial is in writing, it is not a denial and cannot be appealed. More importantly, transgender individuals with well-documented claims are increasingly achieving success in their appeals. Individuals are encouraged to work proactively with their medical providers to ensure that appeals documents include individualized, extensive documentation of the necessity and appropriateness of services. Such appeals should also include a comprehensive and detailed overview of the process of gender transition, including the role of and evidence in support of the specific services requested. In addition to providing a background to uninformed reviewers, such comprehensive documentation conveys the individuals intent to pursue the appeals to the final stages, which can be quite persuasive. To see if your state is one of these, check for the latest information on health coverage at Employer Plans, these are group plans available to small businesses, and sometimes Fully-Funded may include plans offered to qualified individuals. Insurance companies often aggregate these plans to reduce their risk by pooling similar customers; if a small employer could find out who else was in their pool, they might be able to convince the other companies to also ask for a policy change to make their plan transgender-inclusive. However, aggregate group composition is not public information, allowing insurers to control variables to maintain June 17, 2016 175 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Coverage Type General Characteristics and Caveats profit margins. Some of these plans have their own internal medical guidelines that provide for coverage of all services medically necessary for transition. Health these state-regulated organizations provide both the insurance Maintenance coverage and the medical services that they cover. As of December 2015, thirteen states including the District of Columbia have prohibitions on transgender exclusions (note a prohibition on exclusions is not the same as mandated inclusion) in these health plans, with implementation varying by state. Medicaid these are state-run (partially funded by federal money) safety net programs that provides payment to providers who will accept the amount the program is willing to pay (usually much less than private insurance will pay). Medicaid provides coverage for qualified low income people, families and children, pregnant women, the elderly, and people with disabilities. Some states are starting to remove exclusions for trans-specific care from their Medicaid plans. Medicare this is the federal program that covers people over 65 years old, and disabled people under age 65. Railroad Medicare Under this program, people who worked for railroads for at least 10 June 17, 2016 176 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Coverage Type General Characteristics and Caveats years may access Medicare Part B services at favorable rates through the railroad-specified administrator. Transgender-specific services are not available while transgender people are not permitted to serve openly in the military. Union Plans Some labor unions, in some states, may have transgender-inclusive policies available; check with the unions benefits office/department. Several labor unions have resolutions at the national level calling for the elimination of transgender exclusions. Although not binding on member unions, these may help union members fight for benefits equity. Veterans Transgender Veterans may obtain regular medical care, including Administration hormone therapy. Transgender-specific surgical procedures are currently restricted or prohibited, although this may change as the U. Costs and Benefits of Providing Transition-related Health Care Coverage in Employee Health Benefits Plans: Findings from a Survey of Employers. Nondiscrimination in Health Programs and Activities Proposed Rule Section 1557 of the Affordable Care Act [Internet]. The World Professional Association for Transgender Health advocates a simple administrative procedure to change legal identity documents to match experienced gender. The health provider may have leeway, depending on the law, as there is no particular surgery that is necessary for all trans people. Some trans people are unable to change their birth certificate in their home state or country, but may still change their gender markers on their U. While state laws may vary, in some cases it may be necessary for the provider to contact the insurance company and explain the specific circumstances in the case of a sex-specific denial. Once legal documents have been changed, patients should be sure to update their legal name and sex with their insurance company and medical provider to prevent a denial based on a mismatch of information. Legal change of name is not a gendered process in many, but not all jurisdictions; in most jurisdictions the name change process for transgender people is identical to that for non transgender people. License to be Yourself: Laws and advocacy for legal gender recognition of trans people [Internet]. This includes using restroom facilities, inpatient and residential beds, and locker rooms concordant with experienced gender (Grading: X C S). When available and preferred by the individual, non gendered facilities can be utilized, but services should not be dependent on their availability. The legal right to access to programs according to gender identity has expanded with recent state and federal regulation. Schools are required to allow students to use facilities and programs concordant with their gender identity, under the laws of some states, including California. Students should be able to participate in athletic programs and facilities according to gender identity. Students should be referred to according to preferred name and pronoun, and be listed according to gender identity in data systems. Department of Health and Human Services now requires shelters and other housing programs to provide housing and other accommodations and services to trans people according to their gender identity.
Generic 10mg metoclopramide otc
Questionnaires were administered to collect health data gastritis relief quality 10 mg metoclopramide, demographic factors, lifestyle exposures, and developmental progress (M agnus et al. However, these Belgian, Danish, and Dutch studies have poten tial relevance only to female Vietnam veterans with pregnancy subsequent to military service. These have included studies from the Dutch LifeLines cohort study, a multidis ciplinary prospective population-based cohort study examining health and health related behaviors of persons living in the northern region of the Netherlands (de Jong et al. For the current update, the subjects of studies of the effects of environmental exposures have included populations in Belgium (Den Hond et al. Three areas were defned on the basis of soil sampling: Zone A (556 people), the most heavily contaminated, from which all residents were permanently evacuated within 20 days; Zone B (3,920), an area of lower contamination that all children and women in the frst trimester of pregnancy were urged to avoid during daytime; and Zone R (26,227), a region with some contamination in which the consumption of local crops was prohibited (Bertazzi et al. The sample sizes differ among follow-up studies, presumably because of migration; the sample sizes given above were reported in Bertazzi et al. Adults seemed much less likely than children to develop chloracne after acute exposure, but surveillance bias could have affected that fnding. Several cohort studies have been conducted using the Zone A, Zone B, and Zone R exposure categories. There have been multiple long-term follow-up inves tigations of the health outcomes, especially cancers, of Seveso residents. Bertazzi and colleagues, for example, conducted 10-year mortality follow-up studies of adults (Bertazzi et al. Cause-specifc mortality was determined for each zone, compared with that in the comparison cohort, and adjusted for presence at the accident, sex, age, and time since the Seveso accident. They recommended that a distribution based multiple-imputation method be used to analyze environmental data when substantial proportions of observations have non-detectable readings. All the women were interviewed by a nurse blinded to their exposure status, and each subset received gynecologic examinations. M edical records of those who reported ever having received a diagnosis of cancer were obtained and subjected to blind review by a pathologist. Adding the questionnaire data improved the regression model to the point that it explained 42% of the variability. Of the 981 women who had participated in the frst study, 833 were located, alive, and willing to participate in the second. Each was re-interviewed, provided clinical measurements, and consented to a medical record review to confrm her cancer diagnosis. An additional 45 cancers had been diagnosed, for a total of 66 cases, of which 33 were breast cancers. Thyroid cancer was the next most prevalent, with 7 cases, and the 15 other types of cancer observed had at most 3 cases. The main analysis was restricted to the 278 women who had delivered live births that were not the results of contraceptive failure. The birth outcomes that were examined included gestational age, pre-term delivery, and birth weight. Of note, only 35% of women in the analysis were age 21 or older at the time of explosion, thereby limiting the inference of this work to female veterans who served in Vietnam. These have included risk for the development of diabetes and metabolic syndrome 30 years after the accident (W arner et al. The as sociations of adverse pregnancy outcomes and proximity of maternal residence (10 kilometers or fewer) with municipal solid waste incinerators with high dioxin emission levels at the time of birth have also been examined (Tango et al. The emphasis of environmental studies in Japan has been on the long-term follow-up of the 1968 Yusho rice oil poisoning accident. Because of changes in the symptoms and advances in analytic techniques, the diagnostic criteria have changed several times since they were frst published in 1968 (Akahane et al. Hokkaido Study on Environm ent and Childrens Healththe Hokkaido Study on Environment and Childrens Health is a prospec tive birth cohort study that began in 2002 and includes two cohorts (Kishi et al. The frst is the Sapporo (Toho Hospital) cohort with one obstetric hospital, and the second cohort is the much larger Hokkaido cohort, which has 37 hospi tals and clinics. The primary study goals are to examine the effects of low-level environmental chemical exposures on birth outcomes; to follow the development of allergies, infectious diseases, and neurobehavioral developmental disorders and perform a longitudinal observation of child development; to identify high risk groups based on genetic susceptibility to environmental chemicals; and to identify the additive effects of various chemicals, including tobacco smoking (Kishi et al. A self administered questionnaire was completed at the time of enrollment to obtain parental baseline information. Follow-ups and the administration of neurobehavioral developmental tests were conducted at ages 6 and 18 months and 3. The focus of investigations using the Sapporo cohort are on child neurobehavioral development, but the development of asthma, allergies, and infectious diseases is also examined. The Hokkaido cohort enrolled 20,926 pregnant women before 13 weeks of gestational age who visited one of the associated hospitals or clinics in the Hok kaido prefecture between February 2003 and M arch 2012 (participation rate of 55%). A simultaneous analysis of 11 perfuorinated alkyl substances in maternal plasma collected during the third trimester of pregnancy was conducted. Follow-ups of the children were conducted at 18 months and 3 years of age and began in October 2013 and January 2015, respec tively. The follow-ups of 5 and 6-year-old participants started in October 2014 (Kishi et al. Four publications using subsets of the cohort data were iden tifed and reviewed in this volume. The samples were tested for total dioxin levels (as the sum of 29 congeners) and genotyping for genes coding three enzymes involved in dioxin metabolism. The genotype status was previously shown to be related to birth weight in 484 children in the Hokkaido cohort. From 1967 to 1987 the plant pro duced hexachlorocyclohexane (lindane) and its derivatives, and many of the workers experienced chloracne. Dioxins were detected in the small number of air, soil, drinking-water, and cows-milk samples gathered in the region, but no description of how these media were sampled was given. The Russian Childrens Study was de signed to assess the effect of in utero and childhood exposure on development. Although 516 peripubertal boys (identifed through health insurance and clinic records) were enrolled, the fnal cohort consisted of 499 boys and 449 mothers. Annual follow-up examinations were also conducted (9-year retention rate of 73%), blood is collected biennially, urine is collected annually, and semen collection began in 2012. The published fnd ings have detailed the characterizations of serum concentrations in the boys (J. Russ Hauser, and is able to offer a bit more detail regarding initial fndings based on his presentation. Participants were recruited within 2 months after their 70th birthdays randomly from the registry of residents of the community of Uppsala, Sweden, between April 2001 and June 2004. Of the 2,025 subjects who were invited to participate, 1,016 were included, for a participation rate of about 50%; half 2Dr. All participants answered a questionnaire about their medical history, medications, diet, and smoking habits. However, the results are limited by the fact that participants were recruited in the 2-month period after their 70th birthday. In addition, an analysis of the association between each congener and the prevalence of metabolic syndrome was conducted. Using the same cross-sectional study with enrollment extended to December 2009, J. One limitation is the use of the Framingham score; other factors are associated with risk but were not included in the score, such as socio economic position, genetics, and imaging biomarkers. There may also be important unmeasured confounders related to which workers moved away and which ones did not.