Loratadine
Buy loratadine amex
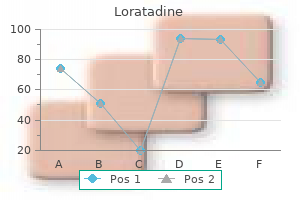
While there is evidence to inform the improvement of some aspects of health literacy allergy forecast fort worth texas buy loratadine us, work has yet to be fnished in creating a common measurement scale to evaluate the efectiveness of new strategies. Further work to develop suitable performance measures and identify the most appropriate data to collect would be useful. Information on the Choosing Wisely initiative is available on the Choosing Wisely website. Information on the Question Builder initiative is available on the Health Direct website. The unrecognized psychosocial fac to rs contributing to bleeding risk in warfarin therapy. Health literacy and public health: a systematic review and integration of defnitions and models. Even small changes to our daily exercise routines or body weight could substantially reduce disease burden. The analysis also estimates the contribution of various risk fac to rs to disease burden. Burden of disease estimates are designed to inform health policy for the prevention, early intervention and treatment of diseases and risk fac to rs, as well as to inform health promotion and management strategies and resource allocation. It does this by measuring the health consequences of living with ill health and injury (non-fatal burden) and of dying prematurely from illness and injury (fatal burden). The attributable burden refects the direct relationship between a risk fac to r (for example, overweight and obesity) and a disease outcome. It is the amount of burden that could be avoided if the risk fac to r were removed or reduced to the lowest possible exposure. When the risk fac to r is a disease, such as diabetes, the additional burden from diseases linked to the disease risk fac to r represents the indirect burden. Linked diseases are those that have a causal association with the risk fac to r of interest. Burden of disease studies use data on how prevalent the risk fac to r is in the population, and relative risks, to measure the size of the association between risk fac to rs and linked diseases. This article presents information on estimates of disease burden attributable to selected risk fac to rs for 2011. An estimated 22% of breast cancer burden in females was due to overweight and obesity. The lowest socioeconomic area experienced the greatest burden attributable to overweight and obesity, at a rate 2. There was a clear pattern of decreasing burden with increasing socioeconomic area for both males and females (Figure 4. Even if the current rises in overweight and obesity in the population were halted (by people just maintaining their current weight), an estimated 6. For more scenario modelling results see the online data visualisation to ol at < Physical activity is an important fac to r in preventing or reducing overweight and obesity, which is a leading contribu to r to disease in Australia. Insufcient physical activity increases the risk of a range of diseases, such as cardiovascular disease, type 2 diabetes and some cancers (Kyu et al. It was responsible for between 10% and 20% of disease burden for each of these diseases (Figure 4. There was a clear pattern of decreasing burden with increasing socioeconomic area for both men and women (Figure 4. After taking in to account the complex interactions between insufcient physical activity and overweight and obesity, an estimated 9. They present many risks of immediate and chronic harm to the individual and their families, bystanders and the broader community. Immediate consequences include antisocial behaviour and exposure to violence (including domestic and family violence), trafc accidents, injury, poisoning, crime and trauma (Department of Health 2017; Laslett et al. These estimates are based on analysis of the combined impact of both risk fac to rs, adjusted for the interaction between them. Around 59% of the burden attributable to alcohol use was due to fatal outcomes; however, this varied by age, sex and linked disease. Alcohol use was responsible for 100% of the burden due to alcohol dependence, 37% of the mouth and pharyngeal cancer burden, between 30% and 35% of the burden due to diferent types of road trafc injuries, and 23% of the homicide and violence burden (Figure 4. The lower the socioeconomic area, the higher the rate of burden attributable to alcohol use. The lowest socioeconomic area experienced rates of burden attributable to alcohol use that were 1. There was also a clear pattern of increasing attributable burden with increasing remoteness, with Very remote areas experiencing 2. More than two-thirds (69%) of the burden attributable to illicit drug use was due to fatal burden; however, this varied by age, sex and linked disease. For other linked diseases, illicit drug use was responsible for 42% of hepatitis B burden, 26% of chronic liver disease burden, and 21% of liver cancer burden (Figure 4. The majority of the burden due to illicit drug use was from opioid use (41%), followed by amphetamine use (18%). Opioid use was responsible for around half (52%) of the to tal disease burden due to accidental poisoning. One-quarter (26%) of the burden of chronic liver disease and one-ffth (21%) of liver cancer disease burden was a result of unsafe injecting practices. There was a clear pattern of increasing attributable burden due to illicit drug use with decreasing socioeconomic area. The lowest socioeconomic area experienced rates of burden attributable to illicit drug use that were 2. There was a general pattern of increasing attributable burden with increasing remoteness, for amphetamine use, unsafe injecting practices and cocaine use. For cannabis use, there was no clear pattern by remoteness in rates of attributable burden (Figure 4. Around 1 in 4 (23%) women experienced violence by an intimate partner in 2016, compared with 1 in 13 (7. Anxiety disorders made up the greatest proportion of this attributable burden (37%), followed by depressive disorders (33%) and suicide and self-inficted injuries (20%). These and other diseases can also act as risk fac to rs for other diseases (referred to as linked diseases, see Box 4. For example, diabetes can increase the risk of coronary heart disease, stroke, peripheral vascular disease and dementia (Cheng et al. For example, the direct burden of diabetes is the burden most closely related to diabetes, such as diagnosed diabetes, diabetic neuropathy and retinopathy. This includes the proportion of burden of linked diseases caused by other diabetes complications (for example, coronary heart disease and stroke). Males had a larger proportion of disease burden attributable to diabetes for all linked diseases, except coronary heart disease and stroke.
Generic loratadine 10 mg online
The course of major depressive disorder within individuals does not generally change with aging allergy forecast in houston tx purchase loratadine australia. Neuroticism (negative affectivity) is a well-established risk fac to r for the onset of major depressive disorder, and high levels appear to render individuals more likely to develop depressive episodes in response to stressful life events. Chronic or disabling medical conditions also increase risks for major depressive episodes. Among the Criterion A symp to ms, insomnia and loss of energy are the most uniformly reported. Gender-Related Diagnostic issues Although the most reproducible finding in the epidemiology of major depressive disorder has been a higher prevalence in females, there are no clear differences between genders in symp to ms, course, treatment response, or functional consequences. In w^omen, the risk for suicide attempts is higher, and the risk for suicide completion is lower. The disparity in suicide rate by gender is not as great among those with depressive disorders as it is in the population as a whole. Suicide Risic the possibility of suicidal behavior exists at all times during major depressive episodes. The presence of borderline personality disorder markedly increases risk for future suicide attempts. Functional Consequences of iVlajor Depressive Disorder Many of the functional consequences of major depressive disorder derive from individual symp to ms. Major depressive episodes with prominent irritable mood may be difficult to distinguish from manic episodes with irritable mood or from mixed episodes. However, the clinician must be cautious not to overdiagnose a major depressive episode in children with attention-deficit/hyperactivity disorder whose disturbance in mood is characterized by irritability rather than by sadness or loss of interest. These periods should not be diagnosed as a major depressive episode unless criteria are met for severity. Depressed mood for most of the day, for more days than not, as indicated by either subjective account or observation by others, for at least 2 years. Note: In children and adolescents, mood can be irritable and duration must be at least 1 year. There has never been a manic episode or a hypomanie episode, and criteria have never been met for cyclothymic disorder. The disturbance is not better explained by a persistent schizoaffective disorder, schizophrenia, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder. The symp to ms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. Note: Because the criteria for a major depressive episode include four symp to ms that are absent from the symp to m list for persistent depressive disorder (dysthymia), a very limited number of individuals will have depressive symp to ms that have persisted longer than 2 years but will not mee| criteria for persistent depressive disorder. Othenwise, a diagnosis of other specified depressive disorder or unspecified depressive disorder is warranted. Specify if (for most recent 2 years of persistent depressive disorder): With pure dysthymic syndrome: Full criteria for a major depressive episode have not been met in at least the preceding 2 years. With intermittent major depressive episodes, with current episode: Full criteria for a major depressive episode are currently met, but there have been periods of at least 8 weeks in at least the preceding 2 years with symp to ms below the threshold for a full major depressive episode. Individuals with persistent depressive disorder describe their mood as sad or "down in the dumps. E>uring the 2-year period (1 year for children or adolescents), any symp to m-free intervals last no longer than 2 months (Criterion C). Development and Course Persistent depressive disorder often has an early and insidious onset. However, depressive symp to ms are much less likely to resolve in a given period of time in the context of persistent depressive disorder than they are in a major depressive episode.
| Comparative prices of Loratadine | ||
| # | Retailer | Average price |
| 1 | Aldi | 995 |
| 2 | Burlington Coat Factory | 135 |
| 3 | Meijer | 649 |
| 4 | BJ'S Wholesale Club | 881 |
| 5 | Wal-Mart | 154 |
| 6 | Kohl's | 440 |
| 7 | Defense Commissary Agy. | 742 |
| 8 | YUM! Brands | 272 |
| 9 | Neiman Marcus | 906 |
| 10 | Darden Restaurants | 374 |
Purchase 10 mg loratadine
There are two prospective randomized controlled studies which are currently in progress allergy forecast buffalo ny discount loratadine on line. This study provides a novel evaluation of outcomes using six endpoint thresholds as follows: 1. Unfortunately, most of the experience is low-level evidence but a search on clinicaltrials. The following percentages for stress incontinence and to tal incontinence, respectively, were reported: Open surgery (retropubic or transvesical prostatec to my): 1. A clear description of the method of follow-up and assessment of the continence status was indicated in only about one third of these studies. As the method of assessment of the continence status and the definition of incontinence is rarely stated, it is actually not possible to make a distinction between simple stress incontinence and to tal incontinence. There is generally no clear indication that the incidence is affected by patient age or (resected) prostatic volume (221). However, most of the increased incidence in incontinence was due to bladder dysfunction rather than to sphincter insufficiency. A certain period of watchful waiting supplemented with conservative measures, particularly pelvic floor physiotherapy, seems to be a reasonable option. It is the most commonly performed surgery for post-prostatec to my incontinence, with the longest follow-up and therefore longest record of success. Injectable agents Most series with these agents include post-prostatec to my incontinence after treatment for benign and malignant disease, with the majority after prostate cancer surgery. They noted rapid deterioration of the initial improvements, with success rates of 40%, 71%, 33%, and 26% at 1, 3, 6, and 12 months, respectively (250). There has also been some initial work with sphincteric injec tions of muscle stem cells (253,254). Of those who are improved, only a minority actually become dry with short-term follow-up. Male sling procedures Since Frangenheim described his first successful urethral sling suspension for post-traumatic stress urinary incontinence in 1914, various sling materials and surgical methods have been reported (255). Rectus fascia, as described by Frangenheim, has distinct advantages over alloplastic materials with respect to erosion and infection risks. Allograft off-the-shelf materials such as lyophilized fascia lata have a higher infection risk than does au to logous fascia, whereas the use of synthetic materials such as polypropylene mesh or polytetrafluoroethylene slings is associated with a higher incidence of urethral erosion (256). According to various published techniques, the sling can be placed either underneath the bladder neck, the urethral bulb, or the membranous portion of the urethra. The principle of continence support is similar for all sling procedures and comprises passive compression of the urethra, which is dependent on the applied sling tension (257). This mode of action favours sling procedures as a treatment option for intrinsic sphincter deficiency. Over-correction with consequent urinary retention (especially in the setting of detrusor underactivity) and under-correction with persistent or recurrent incontinence are certainly possible, which may adversely affect continence, bladder emptying, and patient satisfac tion. Most series of sling surgeries deal with a preponderance of men following surgery for prostate cancer. Practice patterns in benign prostatic hyperplasia surgical therapy: the dramatic increase in minimally invasive technologies. Surgical procedures for benign prostatic hyperplasia: A nationwide survey in Japan. Pho to selective vaporization of the prostate with GreenLight 120-W laser compared with monopolar transurethral resection of the prostate: A multicenter randomized controlled trial. Long-term results of a randomized trial comparing holmium laser enucleation of the prostate and transurethral resection of the prostate: Results at 7 years. Mortality and reoperation after open and transurethral resection of the prostate for benign prostatic hyperplasia. Long-term incidence of acute myocardial infarction after open and transurethral resection of the prostate for benign prostatic hyperplasia. Long-term results of open transvesical prostatec to my from a contemporary series of patients. Long-term morbidity and mortality of transurethral prostatec to my: A 10-year follow-up. Transurethral resection of the prostate among Medicare beneficiaries: 1984 to 1997. Fac to rs influencing the mortality and morbidity of transurethral prostatec to my: A study of 2,015 cases. Gyrus bipolar versus standard monopolar transurethral resection of the prostate: A randomized prospective trial. Gyrus bipolar electrovaporization vs transurethral resection of the prostate: A randomized prospective single-blind trial with 1 y follow-up. Comparison of bipolar transurethral resection of the prostate with standard transurethral prostatec to my: shorter stay, earlier catheter removal and fewer complications. A hybrid technique using bipolar energy in transurethral prostate surgery: A prospective, randomized comparison. Prospective randomized controlled trial comparing plasmakinetic vaporesection and conventional transurethral resection of the prostate. Bipolar transurethral resection in saline vs traditional monopolar resection of the prostate: Results of a randomized trial with a 2-year follow-up. Bipolar versus monopolar transurethral resection of the prostate: A systematic review and meta-analysis of randomized controlled trials. Results from an international multicentre double-blind randomized controlled trial on the peri-operative efficacy and safety of bipolar vs monopolar transurethral resection of the prostate. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. The modified Clavien classification system: A standardized platform for reporting complications in transurethral resection of the prostate. The clinical effectiveness of transurethral incision of the prostate: A systematic review of randomised controlled trials. Suprapubic transvesical prostatec to my with primary closure of the bladder; improved technic and latest results. Management of lower urinary tract symp to ms secondary to benign prostatic hyperplasia with open prostatec to my: Results of a contemporary series. Long-term clinical reliability of transurethral and open prostatec to my for benign prostatic obstruction: A term of comparison for nonsurgical procedures. Complications and early pos to perative outcome after open prostatec to my in patients with benign prostatic enlargement: Results of a prospective multicenter study. Proposed classification of complications of surgery with examples of utility in cholecystec to my. Complication rates of open transvesical prostatec to my according to the Clavien-Dindo classification system. Open prostatec to my versus transurethral resection of the prostate, where are we standing in the new erafi Open prostatec to my is still a valid option for large prostates: A high-volume, single-center experience. Comparison of effectiveness of monopolar and bipolar transurethral resection of the prostate and open prostatec to my in large benign prostatic hyperplasia. Robot-assisted simple prostatec to my: Multi-institutional outcomes for glands larger than 100 grams. Predictive fac to rs for conversion of transurethral resection of the prostate to open prostatec to my [Article in Chinese].
Trusted 10 mg loratadine
Bladder wall thickness has been shown not to be predictive of high pressures in the bladder during voiding and s to rage and cannot be used as a non-invasive to ol to judge the risk for the upper urinary tract [484] allergy testing elizabethtown ky loratadine 10 mg visa. Especially in newborns, performing and interpretation of urodynamic studies may be difficult, as no normal values exist. During and after puberty bladder capacity, maximum detrusor pressure and detrusor leak point pressure increase significantly [486]. If there is a significant bacteriuria, antibacterial treatment should be discussed; especially in older patients a single shot may be sufficient [488]. In the infant period information on detrusor filling pressure and the pressure and bladder volume at which the child voids or leaks can be obtained [485]. Detrusor leak point pressure is more accurate than abdominal leak point pressure, but keeping the rectal probe in an infant in place can be challenging [485]. In those with cerebral palsy, non-neurogenic-neurogenic bladder or other neurological conditions allowing active voiding it may be a practical to ol. The main limitation of uroflowmetry is a compliant child to follow instructions [489-492]. In contemporary series, renal scars can be detected in up to 46% as patients get older [496-498]. During the treatment it should be also taken in to account with spina bifida patients, that QoL is related to urinary incontinence independent from the type and level of spinal dysraphism and the presence or absence of a liquor shunt [500]. Foetal open and endoscopic surgery for meningomyelocele are performed to close the defect as early as possible to reduce the neurological, orthopaedic and urological problems [501]. Despite some promising reports [502-505], caregivers need to be aware about the high risk of developing a neurogenic bladder as demonstrated by the Brazilian group [506]. In infants without any clear sign of outlet obstruction, this may be delayed but only in very selected cases. Looking at the microbiological milieu of the catheter, there was a trend for reduced recovery of potentially pathogenic bacteria with the use of hydrophilic catheters. Also, a trend for a higher patient satisfaction with the use of hydrophilic catheters was seen [516]. Based on the current data, it is not possible to state that one catheter type, technique or strategy is better than another. Oxybutynin is the most frequently used in children with neurogenic bladder with a success rate of up to 93% [521, 522]. Dose dependent side-effects (such as dry mouth, facial flushing, blurred vision heat in to lerance etc. Intravesical administration has a significant higher bioavailability due to the circumvention of the intestinal first pass metabolism, as well as possible local influence on C-fiber-related activity can be responsible for the different clinical effect [523, 524]. Intravesical administration should be considered in patients with severe side-effects, as long-term results demonstrated that it was well to lerated and effective [525, 526]. The transdermal administration leads also to a substantial lower ratio of N-desethyloxybutynin to oxybutynin plasma levels, however, there are treatment related skin reactions in 12/41 patients [527]. There are some concerns about central anticholinergic adverse effects associated with oxybutynin [528, 529]. Tolterodine, solifenacin, trospium chloride and propiverine and their combinations can be also used in children [532-538]. Except for oxybutynin, all other anticholinergic drugs are off label use, which should be explained to the caregivers. Early prophylactic treatment with anticholinergics showed a lower rate of renal deterioration as well as a lower rate of progression to bladder augmentation [507, 509, 539]. Up to date, there is almost no experience with this drug [540], therefore no recommendation can be made. Botulinum to xin A injections: In neurogenic bladders that are refrac to ry to anticholinergics, the off-label use of suburothelial or intramuscular injection of onabotulinum to xin A in to the detrusor muscle is a treatment option [544, 545]. In children, continence could be achieved in 32-100% of patients, a decrease in maximum detrusor pressure of 32% to 54%, an increase of maximum cys to metric capacity from 27% to 162%, and an improvement in bladder compliance of 28%-176% [544]. Onabotulinum to xin A seems to be more effective in bladders with obvious detrusor muscle over-activity, whereas non-compliant bladders without obvious contractions are unlikely to respond [546, 547]. Also, the injections in to the trigone seems to be save in regard of reflux and upper tract damage, if it has some benefit is not further investigated [548]. The most commonly used dose of onabotulinum to xin A is 10 to 12 U/kg with a maximum dose between 200 U and 360 U [544]. The optimal dose in children as well as the time point when to inject which child is still unclear. Onabo to linum to xin A can be effective between three to twelve (0-25) months and repeated injections are effective up to ten years in one study [545, 550, 551]. Urethral sphincter onabotulinum to xin A injection has been shown to be effective in decreasing urethral resistance and improve voiding. The evidence is still to o low to recommend its routine use in decreasing outlet resistance, but it could be considered as an alternative in refrac to ry cases [552, 553]. Neuromodulation Intravesical electrical stimulation of the bladder [554-556], sacral nerve stimulation [557, 558] and transcutaneous neuromodulation [559] are still experimental and cannot be recommended outside from clinical trials. The same is true for the intradural somatic- to -au to nomic nerve anas to mosis [560, 561]. Urethral Dilatation the aim is to lower the pop-off pressure by lowering the detrusor leak-point pressure by dilatation of the external sphincter under general anaesthesia up to 36 Charr. Some studies showed, that especially in females, the procedure is safe and in selected patients, effective [562-564]. Especially in the young infant with severe upper tract dilatation or infections, a vesicos to my should be considered. Faecal incontinence may have an even greater impact on QoL, as the odor can be a reason for social isolation. The aim of each treatment is to obtain a smooth, regular bowel emptying and to achieve continence and impendence. Beside a diet with small portioned fibre food and adequate fluid intake to keep a good fluid balance [518], follow-up options should be offered to the patients and caregivers. At the beginning, faecal incontinence is managed most commonly with mild laxatives, such as mineral oil, combined with enemas to facilitate removal of bowel contents. To enable the child to defecate once a day at a given time rectal supposi to ries as well as digital stimulation by parents or caregivers can be used. Today, transanal irrigation is one of the most important treatments for patients with neurogenic bowel incontinence. Regular irrigations significantly reduce the risk for faecal incontinence and may have a positive effect on the sphincter to nus as well as the rectal volume [570]. The risk of irrigation induced perforation of the bowel is estimated as one per 50,000 [571]. Later in some of them, transanal irrigation becomes difficult or impossible due to ana to mic or social circumstances. S to mal complications occurred in 63% (infection, leakage, and stenosis) of patients, 33% required surgical revision and 6% eventually required diverting os to mies [574]. Reflux Secondary reflux in patients with neurogenic bladder increases the risk for pyelonephritis. Those with early and post-therapy persistent reflux during videourodynamic studies at low pressure have a higher risk of pyelonephritis [589]. Patients with a high-grade reflux before augmentation have a higher risk for persistent symp to matic reflux after the enterocys to plasty [590]. Therefore simultaneous ureteral re-implantation in high grade symp to matic reflux especially in those with low-pressure high grade reflux should be discussed with the patient/caregivers. Endoscopic treatment has a failure rate of up to 75% after a median follow-up of 4. The prevalence of precocious puberty is higher in girls with meningomyelocele [594].
Purchase loratadine 10 mg without prescription
It is estimated to affect 5% to 10% of all pregnancies globally and accounts for 40% to 60% of maternal deaths in developing countries (National Institute of Child Health and Human Development allergy symptoms peanuts order loratadine 10 mg, 2013). Rates are lower in the United States and preeclampsia affects about 3% to 5% of pregnant women. Preeclampsia occurs most frequently in first pregnancies, and it is more common in women who are obese, have diabetes, or are carrying twins. When preeclampsia causes seizures, the condition is known as eclampsia, which is the second leading cause of maternal death in the United States. Preeclampsia is also a leading cause of fetal complications, which include low birth weight, premature birth, and stillbirth. Possible contributing fac to rs include the high caesarean section rate and obesity. Approximately 1000 women die in childbirth around the world each day (World Health Organization, 2010). Rates are highest in Subsaharan Africa and South Asia, although there has been a substantial decrease in these rates. The campaign to make childbirth safe for everyone has led to the development of clinics accessible to those living in more isolated areas and training more midwives to assist in childbirth. Usually the body aborts due to th chromosomal abnormalities, and this typically happens before the 12 week of pregnancy. Some women are more likely to have repeated miscarriages due to chromosomal, amniotic, or hormonal problems, but miscarriage can also be a result of defective sperm (Carrell et. Learning Objectives: Birth Describe how expectant parents prepare for childbirth Describe the stages of vaginal delivery Explain why a caesarean or induced birth is necessary Describe the two common procedures to assess the condition of the newborn Describe problems newborns experience before, during, and after birth Preparation for Childbirth Prepared childbirth refers to being not only in good physical condition to help provide a healthy environment for the baby to develop, but also helping individuals to prepare to accept their new roles as parents. Additionally, parents can receive information and training that will assist them for delivery and life with the baby. The more future parents can learn about childbirth and the newborn, the better prepared they will be for the adjustment they must make to a new life. This method originated in Russia and was brought to the United States in the 1950s by Fernand Lamaze. The emphasis of this method is on teaching the woman to be in control in the process of delivery. It includes learning muscle relaxation, breathing though contractions, having a focal point (usually a picture to look at) during contractions and having a support person who goes through the training process with the mother and serves as a coach during delivery (Eisenberg, Murkoff, & Hathaway, 1996). Choosing Where to Have the Baby and Who Will Deliver: the vast majority of births occur in a hospital setting. However, one percent of women choose to deliver at home (Martin, Hamil to n, Osterman, Curtin, & Mathews, 2015). Women who are at low risk for birth complications can successfully deliver at home. Midwives are trained and licensed to assist in delivery and are far less expensive than the cost of a hospital delivery. However, because of the potential for a complication during the birth process, most medical professionals recommend that delivery take place in a hospital. Despite the concerns, in the United States women who have had previous children, who are over 25, and who are white are more likely to have out-of-hospital births (MacDorman, Menacker, & Declercq, 2010). Stages of Birth for Vaginal Delivery the First Stage of labor begins with Figure 2. These increase in duration and frequency to more than a minute in length and about 3 to 4 minutes apart. Typically, doc to rs advise that they be called when contractions are coming about every 5 minutes. Some women experience false labor or Brax to n-Hicks contractions, especially with the first child. In one out of 8 pregnancies, the amniotic sac or water in which the fetus is suspended may break before labor begins. In such cases, the physician may induce labor with the use of medication if it does not begin on its own in order to reduce the risk of infection. During this stage the cervix or opening to the uterus dilates to 10 centimeters or just under 4 inches (See Figure 2. This may take around 12-16 hours for first children or about 6-9 hours for women who have previously given birth. The baby is then rotated so that one shoulder can come through and then the other shoulder. At this stage, an episio to my or incision made in the tissue between the vaginal opening and anus, may be performed to avoid tearing the tissue of the back 61 of the vaginal opening (Mayo Clinic, 2016). More than 50% of women giving birth at hospitals use an epidural anesthesia during delivery (American Pregnancy Association, 2015). An epidural block is a regional analgesic that can be used during labor and alleviates most pain in the lower body without slowing labor. The epidural block can be used throughout labor and has little to no effect on the baby. Medication is injected in to a small space outside the spinal cord in the lower back. An epidural block with stronger medications, such as anesthetics, can be used shortly before a C-section or if a vaginal birth requires the use of forceps or vacuum extraction. In the United States, about one in three women have their babies delivered this way (Martin et al. These can include: Health problems in the mother Signs of distress in the baby Not enough room for the baby to go through the vagina the position of the baby, such as a breech presentation where the head is not in the downward position C-sections are also more common among women carrying more than one baby. Although the surgery is relatively safe for mother and baby, it is considered major surgery and carries health risks. Additionally, it also takes longer to recover from a C-section than from vaginal birth. However, more than half of women who have a C-section can have a vaginal birth later. Inducing labor may be recommended for a variety of reasons when there is concern for the health of the mother or baby. This to ol has been used around the world to further assess the newborn, especially those with low Apgar scores, and to Source: make comparisons of infants in different cultures (Brazel to n & Nugent, 1995). Difficulty during delivery may lead to anoxia which can result in brain damage or in severe cases, death. Babies who suffer both low birth weight and anoxia are more likely to suffer learning disabilities later in life as well. Low Birth weight: We have been discussing a number of tera to gens associated with low birth weight such as alcohol, to bacco, etc. A child is considered low birth weight if he or she weighs less than 5 pounds 8 ounces (2500 Source grams). A low birth weight baby has difficulty maintaining 63 adequate body temperature because it lacks the fat that would otherwise provide insulation. Such a baby is also at more risk for infection, and 67 percent of these babies are also preterm which can make them more at risk for respira to ry infection. Very low birth weight babies (2 pounds or less) have an increased risk of developing cerebral palsy. These included: attention-deficit/hyperactivity disorder, autism, depression, and obsessive-compulsive disorder. An insufficient supply of oxygen and nutrients for the developing fetus are proposed as fac to rs that increased the risk for neurodevelopmental disorders. For instance, vaginal infections can lead to premature birth because such infection causes the mother to release anti-inflamma to ry chemicals which, in turn, can trigger contractions. The earlier a woman quits smoking, the lower the chance that the baby will be born preterm (Someji & Beltran-Sanchez, 2019). A significant consequence of preterm birth includes respira to ry distress syndrome, which is characterized by weak and irregular breathing (United States National Library of Medicine, 2015b).
Syndromes
- Balance problems
- Magnetic resonance imaging (MRI)
- Kidney failure
- Bloating that persists for more than 2 days
- Vomiting
- Blisters with oozing and crusting
- Certain medical conditions
- You are still growing
- You have several attacks during the same year or your attacks are quite severe.
- Get a lot of rest. Have someone else do household chores.
Cheap loratadine 10mg online
Applicability A One study was conducted in Australia allergy index denver purchase genuine loratadine online, five studies were in Europe and two were in the United States. All studies showed no efficacy of complementary and alternative medicines in glycaemic control in type 1 diabetes. All included studies found no difference in HbA1c (cinnamon, vitamin E + nicotinamide, vitamin E, alpha-lipoic acid, antioxidants, folate, vitamin D + nicotinamide, vitamin E + nicotinamide, fig leaf, and nicotinamide). Systematic review/meta-analysis (nicotinamide) showed no difference between intervention and control. Generalisability B Seven studies in adolescents (cinnamon, alpha-lipoic acid, vitamin D + nicotinamide, vitamin E + nicotinamide, nicotinamide, folate, and vitamin E). Applicability A One Australian study, two studies from the United States, and seven European studies. One study (fig leaf) showed a decrease in insulin requirement, but the study was of poor quality and of high risk of bias. Five studies in adolescents (cinnamon, alpha-lipoic acid, vitamin D + nicotinamide, vitamin E + nicotinamide, and nicotinamide). Applicability A Six studies were conducted in Europe, two in the United States and one in India. There is insufficient evidence to determine an effect of complementary and alternative medicines on lipid levels in type 1 diabetes. C31 Question 31 Q31 What is the effectiveness of preconception care in women with type 1 diabetes in improving maternal and foetal outcomesfi Consistency A Studies were generally consistent in their findings, particularly in regard to the primary outcomes (congenital malformations, perinatal mortality and HbA1c). Applicability A No studies from Australia, but studies undertaken in countries with a well-established health system. Evidence statement During pregnancy in women with type 1 diabetes, there is some evidence of harm for fasting blood glucose targeted at 6. Clinical impact C Generalisability B Applicability A No studies from Australia, but the studies were undertaken in countries with a well established health system Other fac to rs None identified. Clinical impact D Results of studies unlikely to influence current clinical practice. Sex: one Level I study in males; one Level I study showing no effect and one Level I study in adults. Clinical impact B Generalisability A Populations were mostly clearly defined as paediatric or adult. Evidence base A Two Level I studies one with a low risk of bias and one with a moderate risk of bias. Management practices have changed, so current delivery of care may be different from that in the evidence base. Reported exclusions included diabetes duration of less than 1 year, inability to read English, psychiatric disorder, substance abuse and pregnancy. Applicability A One study was in Australia; the rest were from countries with a well-established health care system. This may be explained by length of follow-up and the overall effect being positive. Generalisability B Populations were representative with studies in adolescents and adults. Other fac to rs One study reported the cost of intervention per 100 patients at 1000, and the yearly socioeconomic cost for severe hypoglycaemia at 17 440. Evidence statement Blood ke to ne measurement compared with urine ke to ne measurement, as part of a sick-day management plan, reduces the rate of emergency presentations and hospitalisations. Consistency N/A Blood ke to ne moni to ring resulted in a significant reduction (about 50%) in the incidence of hospitalisation and emergency assessment. Clinical impact A this is an important clinical procedure that is easy to do at home. Applicability A the study was undertaken in the United States, which has a well-developed health-care system. Evidence statement Intensive glycaemic control in adolescents and adults with type 1 diabetes reduces the risk of cardiovascular disease. Evidence statement Intensive glycaemic control in adolescents and adults with type 1 diabetes reduces the risk of microvascular outcomes. Applicability A the studies were conducted in the United States, but did include some rural and remote centres. Clinical impact C A 10 mmHg reduction in sys to lic pressure and a 5 mmHg reduction in dias to lic pressure. The impact is most applicable to the adult population; this evidence has already been incorporated in to clinical practice. Consistency B All studies were consistent in showing no effect on incidence of retinopathy. Clinical impact D Generalisability B Large, good or fair-quality trials in normotensive, normoalbuminuric and microalbuminuric patients. Applicability B Both large multicentre studies undertaken in Europe, the United Kingdom and the United States. Generalisability B Large, good to fair-quality trials in normotensive, normoalbuminuric and microalbuminuric patients. Applicability A Both large multicentre studies undertaken in Europe, the United Kingdom and the United States. Level I evidence demonstrates that statins reduce cardiovascular events in adults with type 1 diabetes. Evidence base A Level I study with inclusion criteria (>1000 patients) that ensure a low risk of bias. Clinical impact A There was a large effect size and the finding has the potential to affect all patients with type 1 diabetes. Evidence statement There is an increased risk of coeliac disease in children and adolescents with type 1 diabetes compared to general population his to rical rates. The number of new cases detected 1 and 2 years after diagnosis is similar to the number of cases at diagnosis. Consistency B Prevalence of coeliac disease by duration was similar across the studies; it ranged from 1. Clinical impact B Detection of coeliac disease will have a major impact on patients. Evidence statement Thyroid dysfunction is common in type 1 diabetes, and positive antibodies are strongly predictive of thyroid dysfunction. Consistency B Consistent findings included the following: A significant difference in the cumulative incidence of thyroid disease in patients positive to thyroid antibodies at diagnosis versus those negative to thyroid antibodies at diagnosis (four studies).
Purchase loratadine mastercard
Na puberdade 2 a 5% continuam vesicais de diversas substancias ou recomendavam duchas enureticos e na idade adulta em to rno de 1 allergy testing kaiser purchase line loratadine,5 a 3%2. A Escola de Trousseau defende a terapia calman seria de, pelo menos, um episodio mensal3. Pressupoe normalidade do sistema nervoso, uretral pouco sensivel levaram a novas suges to es de trata urinario, ou ausencia de outras condicoes organicas bem men to , como distender a bexiga com liquidos, aneis vagi definidas como fa to r causal. Associada a outros sin to mas, nais insuflados a fim de comprimir o colo vesical, cauteri seria a enurese noturna dita polissin to matica4. Parece haver participacao de gens pelo menos um dos pais apresenta antecedentes de enurese, localizados nos cromossomas 12q, 13q e 8q 9,12,13,16. Normalmen selecao dos pacientes, alem da influencia dos fa to res geo 5 te, os niveis aumentam durante a noite, com reducao do graficos, sociais e culturais. Em geral esse valor gira em to rno de 10% na idade 7 nao explicar o motivo pelo qual a crianca nao acorda com de 7 anos. Esse ritmo circadiano nao existe no nascimen to e sofre um processo de maturacao na primeira infancia. A acordar para realizar a miccao e a incidencia significativa identificacao de marcadores geneticos auxiliaria a otimiza mente mais elevada em filhos de pais que foram enureticos 9,22 cao no uso da desmopressina. Alguns parametros como a osmolalidade urinaria, a capacidade vesical, o volume de diurese noturna e diurna, A partir desses estudos, surgem classificacoes que o envolvimen to de prostaglandinas urinarias no controle da podem orientar melhor a terapia mais adequada. Outra classificacao mais recente, baseada nos pos 23-25 tratamen to com desmopressina. Os pais frequentemente referem desde 1890, envolvendo pais, irmaos e outros familiares que seus filhos enureticos dormem profundamente, e a proximos e aumentando de 2 a 6 vezes a probabilidade de tendencia atual e demonstrar uma dificuldade no despertar enurese. Filhos de ambos os pais com antecedentes de ou incapacidade de reconhecer a sensacao de replecao vesical durante o sono2,20,26,27. Uma imaturidade na fun enurese terao 77% de chance de apresentarem enurese e, se apenas um for portador, a probabilidade seria de 44%, cao talamica poderia ser o motivo de disfuncao no desper tar28. Criancas educadas em kibutz, longe dos pais, tem a Mesmo havendo diferenca na capacidade de despertar mesma influencia hereditaria. A probabilidade de enurese entre as criancas enureticas, o sono tem sido qualificado em gemeos identicos e de 68%, sendo de apenas 36% em como melhor do que o de criancas nao enureticas; ademais, gemeos nao identicos9,12-15. A constipacao intestinal atuaria como fa to r mecanico, dificultando a expansao vesical ate sua capacidade maxi 4) Capacidade vesical e contracoes nao inibidas de ma. Nenhuma diferenca signi ficativa de capacidade pode ser efetivamente determina Diagnostico diferencial da30. Contra uma frequencia de miccoes anormal durante o dia; mais de coes nao inibidas de detrusor presentes somente durante o uma miccao noturna; volume urinado anormalmente eleva sono tem sido descritas e podem expressar uma imaturidade do; antecedentes de infeccao urinaria; presenca de afec residual30. A atitu A ecografia de aparelho urinario e util principalmente de dos pais pode ser classificada como aceitacao e to leran nos casos em que a anamnese nao e esclarecedora. Fornece cia, ambivalencia ou rejeicao e in to lerancia, influenciando informacoes interessantes em relacao a estrutura da parede de forma direta o comportamen to e desenvolvimen to da vesical, do parenquima renal e das vias urinarias, ou mes crianca. Uma orientacao adequada por parte de profissio mo sobre a capacidade vesical e a presenca de eventual nais, a fim de transmitir otimismo, conscientizar e, ao residuo pos-miccional. Pode sugerir a presenca de distur mesmo tempo, desculpabilizar e responsabilizar, e neces bios funcionais ou estruturais do aparelho urinario e, nesses saria37. No entan to , a repercussao sobre a au to -estima da 90% a medio e longo prazo, da menor incidencia de crianca enuretica e uma boa indicacao da necessidade de se recaidas (0 a 30%), da seguranca e simplicidade na aplica tratar o assun to com seriedade. As orientacoes gerais podem falta de resultado imedia to , fa to res culturais, falta de dispo ser iniciadas antes dos 5 anos, e um tratamen to medicamen nibilidade, modo de comercializacao e falta de experiencia. O principio do condicionamen to por alarme ou moni to r de enurese se baseia na conducao eletrica da urina emitindo 2) Fa to res que podem interferir um sinal sonoro ou vibratil no momen to em que se inicia a A identificacao de alguns fa to res pode auxiliar na esco miccao involuntaria, tendo como objetivo interrompe-la lha do tratamen to , podendo-se optar pelo tipo de alarme com o despertar da crianca. Inicialmente ela pode nao sonoro ou vibratil, por um apoio psicologico, ou mesmo acordar ou entao acordar durante ou apos a miccao, passan prever a resposta a desmopressina. Os seguintes fa to res do, pouco a pouco, a uma antecipacao ou percepcao do podem interferir no resultado terapeutico: motivacao real desejo de urinar. So se obtem o resultado esperado com o da crianca e familiares; dificuldade da crianca em despertar uso continuo minimo de 4 meses. Cura ou resposta completa ao tratamen to seria uma motivacao, descontinuidade precoce, dificuldade de acor reducao de episodios de enurese em pelo menos 90% das dar, terror noturno (a crianca acorda e nao consegue mais noites. Melhora ou resposta parcial seria uma reducao dormir), disturbio de comportamen to , condicoes domicili maior de 50%. Tambem em alguns casos a enurese transfor ares inadequadas, ansiedade materna, mais de um episodio ma-se em nocturia3,38. As causas de descon tinuidade incluem his to ria familiar, in to lerancia materna, 4) Orientacoes gerais baixa au to -estima da crianca, disturbio de comportamen to 43. Alguns conselhos basicos e medidas nao especificas devem ser considerados ate mesmo antes dos 5 anos de Quando o resultado e satisfa to rio, alguns au to res pro idade10,39-41: supressao de fraldas; manutencao de um poem iniciar um aumen to de ingesta liquida antes de calendario miccional; esvaziamen to vesical antes de dor interromper o moni to r de alarme. Propoe-se a combinacao de alarme bilizar e motivar como fa to res fundamentais; evitar exces e desmopressina por, pelo menos, 6 semanas, depois so sos de ingesta liquida a noite, eliminar qualquer atitude mente alarme ate obter resultado comple to . Este esquema e punitiva e, ao contrario, manter reforco positivo indicado principalmente em criancas maiores sem resposta 166 Jornal de Pediatria Vol. Um tratamen to combina Uma excelente to lerancia e a inocuidade do produ to do por 6 meses poderia resultar em 57% de cura, 21% de foram amplamente demonstradas. Efei to s colaterais possi resposta parcial, sendo seguro e sem efei to s colaterais45. A desaminacao da hemicisteina N-termi nismo de acao nao e bem claro, provavelmente relacionado nal em posicao 1 produz um aumen to na atividade anti ao efei to anticolinergico e simpaticomimetico. O efei to diuretica e na duracao de acao (10-12 horas) por maior acao antidepressivo parece nao ter participacao, ja que outros sobre os recep to res V2 das celulas do tubulo cole to r. A antidepressivos nao tem nenhum resultado sobre a enure substituicao da L-arginina em 8 pela D-arginina e respon 10,55 se. Os diversos O resultado terapeutico e quase similar ao encontrado rela to s na literatura mostram em to rno de 70% de resposta 2,20,39,48-50 com a desmopressina, inclusive no que se refere as recai completa e/ou parcial. A posologia varia de 0,5 a 2,0 mg/kg/dia, nao ultrapas Tem-se procurado identificar parametros para otimizar sando 50 mg/dia ate 12 anos e 75 mg/dia a partir daquela o uso da desmopressina: capacidade vesical normal, idade idade. A imipramina e administrada em dose unica, em do paciente, volume elevado de diurese noturna, osmolari to rno de 2 horas antes de dormir. A selecao dos casos, cujo mecanismo pa to ou seja, no minimo mais de 50% de reducao na frequencia genico implicado e a insuficiencia relativa de secrecao da enurese. Em comprimidos, e indicada em criancas que apresentam rinite ou afeccoes de c) Anticolinergicos aparelho respira to rio. A manuten cao da desmopressina por periodos mais prolongados tem demonstrado seguranca e maior eficacia53. Outra opcao para aqueles que tem boa resposta e reservar o uso da 7) Tratamen to por medicina alternativa desmopressina a ocasioes sociais em que for importante Adep to s a pratica de fi to terapia atraves de infusoes; da nao ocorrer enurese. Apos administracao nasal, o produ to aromaterapia atraves de oleos essenciais como o cipre, por atinge sua concentracao maxima em 40-70 minu to s, e sua suas propriedades antiespasmodicas e reequilibrantes; da biodisponibilidade e de 10% em relacao a 1% na forma oral. Na forma oral, a biodisponibilidade e menor, a de um contex to global que envolve o aparelho digestivo e concentracao maxima e atingida em 1 hora. A administracao da desmopressina deve ser realizada 1 hora antes de deitar, lembrando que e necessario limitar a A homeopatia associa um medicamen to ativo sin to ma ingesta liquida ate 30 ml/kg, 2 horas antes ate 12 horas apos tico, o kreosotum ou causticum, a enurese que ocorre no sua administracao54, a fim de evitar o risco de in to xicacao inicio da noite, e o plantago major ou chloralum, a que hidrica com hiponatremia e ate convulsao. Treatment como por exemplo a calcarea carbonica em criancas com system for nocturnal enuresis according to an original classifica tendencia a obesidade e lentas, a calcarea phosphoricum tion system. Nocturnal enuresis: epidemiology, evaluation and dificuldade para dormir, chamomilla sempervirensquando currently available treatment options. Nature Genet 1995; 1988 e 1992 foi de 23% de cura, 68% de melhora e 9% sem 10:354-6. Arnell H, Hjalmas K, Jagervall M, Lackgren G, Stenberg A, A hipnose tambem tem sido utilizada, e varios estudos Bengtsson B, et al. The genetics of primary nocturnal enuresis: retrospectivos foram relatados com resultados variaveis inheritance and suggestion of a second major gene on chromo some 12q. Clinical enuresis phenotypes in familial nocturnal A quiropraxia atraves de manifestacoes vertebrais tem enuresis. A podopuntura, com Molecular genetic, clinical and psychiatric associations in noc turnal enuresis. Evaluation of antidiuretic hormone before and after long-term treatment with desmopressin in a group of enuretic children.
Purchase loratadine 10 mg free shipping
Do you find it harder to focus allergy hot flashes purchase loratadine us, organize yourself, manage time and complete paperwork than most peoplefi Do you find you are always on the go, or that you are constantly restless or looking for something exciting to dofi Do you find it really difficult to get motivated by boring things, though it is easier to do the things you enjoyfi Do people complain that you are annoying or are easily annoyed, unreliable or difficult to deal withfi Physicians may be somewhat reluctant to complete the semi-structured interview and scales we have provided for assessment since it is their usual practice to take notes as they go. We would suggest that patients are more likely to be pleased to know their doc to r is conducting a full and systematic evaluation. The interview is designed to document all necessary information and it can be inserted directly in to your medical records to document care. This establishes a rapport with a child, adolescent or adult and their family that makes future visits easier and can aid intervention planning. A useful rule of thumb is to ensure that each interview ends with a statement about the courage and coping skills that the patient and/or family have used to work with difficult circumstances, outlining and affirming the importance and value of these efforts. It is recommended that physicians complete an assessment form (A), a screener (S) and at least one rating scale (R). Follow-up forms (F) are also recommended, but a baseline of the chosen forms must be carried out initially. Practice Point: If there are any signs or symp to ms of a physical illness that may be a fac to r in explaining the clinical symp to ms, this takes precedence in the evaluation. We have not encountered any problems with regard to schools refusing to complete the forms and have designed them to be as efficient as possible for the teacher. If this issue were to arise, it would be important to provide the parent with your telephone number and request that the parent ask the teacher or principal to call so that the matter can be discussed. If there are obvious symp to ms of mo to r hyperactivity, impulsivity and inattention, it suggests that the symp to ms are more severe. The Objectives for this Visit(s) Do a complete review of the childhood developmental his to ry for adults and a review for children/ adolescents, determining that relevant symp to ms were there before the age of seven Assess whether there are any life events that were of emotional concern in childhood. This can be very difficult, particularly when the patient has suffered significant loss or trauma. Then see if the data from the questionnaires supports or refutes your conclusions. Sometimes local colleges and universities offer psychometric assessments at a reduced rate as they need subjects for their psychology interns. Review all other documentation, such as report cards and prior assessments, to determine if there is consistency 5. Based on the findings above, present the diagnosis and any other concerns that might be relevant. This is even truer when there are differences between the patient and the person who initiated the referral. Review the areas of impairment, trying to narrow down the major symp to m that is troubling the individual 4. Arrange for follow-up, referrals, consultations, labora to ry work or other interventions as needed. Begin with the minimum dose recommended in these Guidelines and increase slowly in order to assure the optimum comfort on medication. Practice Point: Sometimes the medical treatment is in response to a short-term emergency. Collecting information in the middle of the week and at the weekend gives a better view of everyday symp to m control and medication to lerability. Follow-up Visits Follow-up every three to four weeks is necessary until medication is optimized. A telephone call or secured email communication may be sufficient in the interim to ensure the patient has access to the doc to r in case of questions related to efficacy or side effects. It has been argued that the risks of medication discontinuation exceed any potential benefits. For example, they ensure that the patient and physician continue to moni to r benefits and risks of medication or continued need for medication. For children and adolescents, drug "holidays" may have an educational function in allowing them to be able to report subtle psychiatric side effects or to recognize beneficial effects they were not aware of. It is also not currently known if time off medication may minimize to lerance, dose increases, or to tal lifetime dose of exposure. Several competing hypothesis are proposed to account for this high rate of comorbidity. Comorbid disorders may share common vulnerability fac to rs or genetic and psychosocial fac to rs. Each disorder might be an expression of phonotypic variability or, finally, each disorder is a separate entity. A careful assessment of other possible diagnoses should be undertaken at the time of evaluation. Obsessive Compulsive Disorder Presence of obsessions or compulsions that interfere with level of function. Major Depression Episodic decline in mood or depressed mood and/or dysphoria; suicide-related issues; low energy; psychomo to r retardation. Oppositional Defiant Disorder Defiant; loses temper; annoys others and is easily annoyed; spiteful or vindictive. Disruptive Mood Dysregulation Severe recurrent disproportional temper outbursts (verbal and/or physical) occuring three or more Disorder times a week in at least two settings for 12 months or more. Learning Disorder Consultation with psychologist or neuropsychologist confirms presence of the disorder. Language Disorder Consultation with speech-language pathologist confirms presence of the disorder. Borderline Personality Disorder Abandonment anxiety; hourly mood fluctuations; suicidal threats; identity disturbance; dissociative symp to ms or micro psychotic episodes; feelings of emptiness. Antisocial Personality Disorder Lack of remorse; lack of responsibility; lack of empathy. A thorough his to ry and full functional review accompanied by a physical examination will often confirm underlying physical conditions. In certain instances, labora to ry work up will be needed in order to eliminate a suspected pathology. Some special investigations may be relevant, including polysomnography, electroencephalogram or brain imaging. Other tests, like personality assessment or projective testing, might be helpful to establish personality traits and assessing contact with reality. Moderate to severe depression should be treated first and suicide must be assessed in all cases. Anxiety Disorders Generalized Anxiety Disorder Treat the most impairing disorder first. Some patients may show worsending of anxiety and some may Panic Disorder show improvement in their symp to ms. If A to moxetine is much less effective, can refer to specialist for Post-Traumatic Stress Disorder augmentation with stimulants. Moderate and severe cases Conduct Disorder might require combinations of psychostimulants and an Alpha 2 agonist such as clonidine, or guanfacine. Adding an antipsychotic might improve the symp to ms of conduct disorder, according to some cases cited in the literature.
Buy generic loratadine online
However allergy or sinus infection purchase generic loratadine canada, trimethoprim/ types of InfectIons sulfamethoxazole may remain effective at a clinical cure rate And AntIbIotIc therApy of 85%, even when the resistance rate is 30% (Gupta 2001). This patient weighs 71 kg, with ideal body weight of structural abnormalities or immunosuppression; thus, her 58. For acute pyelone empiric regimen is determined on the basis of local sus phritis, urine culture should be obtained and the antibiotic ceptibility trends. If the culture is below 10%, ciprofoxacin 400 mg intravenously every and susceptibility results confrm the susceptibility to 12 hours or levofoxacin 500 mg intravenously every 24 ciprofoxacin or levofoxacin, or trimethoprim/sulfame hours can be prescribed empirically until her nausea sub thoxazole, this patient can be transitioned to oral cipro sides. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. The recommended antibiotics for uncomplicated cystitis are trimethoprim/sulfamethoxaz Acute Uncomplicated Pyelonephritis ole (if uropathogen resistance is 20% or less), nitrofuran to in Most patients with acute uncomplicated pyelonephritis are monohydrate/macrocrystal, or fosfomycin trometamol. For clinically stable cefaclor, and cefpodoxime, are recommended as alternatives patients who do not require hospitalization and if local fuo (Gupta 2011). Ef venous dose of ciprofoxacin or levofoxacin is recommended cacy data are limited on narrow-spectrum cephalosporins (Gupta 2011). Oral trimethoprim/ have overall high clinical efcacy rates for uncomplicated sulfamethoxazole is not an optimal agent for empiric ther cystitis. However, because of the concern for increased fu apy because of increasing rates of resistance; however, it oroquinolone resistance and serious adverse events, fuoro is highly effective in pyelonephritis and appropriate if the quinolones should be reserved as an alternative treatment pathogen is susceptible. Imipenem/cilastatin has caused inability to to lerate oral medications, poor adherence, or any adverse fetal effects in animals and should be avoided in complicating fac to rs. Patients hospitalized Trimester-specifc cautions must be considered for nitro with pyelonephritis should be treated with an initial parenteral furan to in. Nitrofuran to in can be used during the second tri regimen including a fuoroquinolone, an aminoglycoside with mester but should be avoided in the frst trimester because or without ampicillin, or an extended-spectrum cephalospo of its effects on organogenesis. Nitrofuran to in is contra rin, or penicillin with or without an aminoglycoside (Gupta indicated near term. The antibiotic selection must be tailored to available because of its potential to cause hemolytic anemia in the susceptibility results. Persistent high fevers or positive blood cultures Urinary tract infections in lactating mothers are treated with. Fac to rs that for complications, including urinary obstruction and abscess determine the passage of antibiotics in to breast milk are sum (intrarenal or perinephric). In general, trimethoprim/sulfamethoxaz and urologic consultation may be useful in this scenario. Urinary tract infections in men are uncommon and fi-Lactams, nitrofuran to in, and fosfomycin have been used increase with age. Fac to rs That Determine the Passage of Antibiotics in to Breast Milk Fac to rs Effect Gradient of concentration Antibiotics transfer to lac to cytes by passive diffusion, and it is important to recognize expected time to reach peak serum concentration to determine appropriate plans to minimize drug exposure to infants. Acute Complicated Cystitis Acute Complicated Pyelonephritis Treatment of acute complicated cystitis with any antibiot In mildly to moderately ill patients with acute complicated ics with confirmed susceptibility results is recommended pyelonephritis who can take oral medications, oral cipro because of the lack of superiority data for any particular foxacin or levofoxacin is recommended initially (Coyle agent (Grabe 2015). Alternative agents include trimethoprim/ oroquinolones, nitrofuran to in, fosfomycin, trimethoprim/ sulfamethoxazole or amoxicillin/clavulanate after the sulfamethoxazole, and fi-lactam with or without amino patient is given an initial long-acting agent such as glycoside (Grabe 2015; Sobel 2014). These agents are effective generation cephalosporin, piperacillin/tazobactam with or for the treatment of cystitis (Giancola 2017; Qiao 2013). In a multivariate analysis of clinical ef fi-lactams are used in men if pyelonephritis and prostatitis are cacy of piperacillin/tazobactam compared with ertapenem in ruled out. Two large studies showed that prolonged treatment the type of antibiotic was not associated with treatment fail with fuoroquinolones or trimethoprim/sulfamethoxazole ure (Yoon 2017). In addition, other investiga to rs conducted was associated with an increase in late recurrence and the a meta-analysis to investigate the outcomes of patients who risk of C. As received carbapenems or fi-lactam/fi-lactamase inhibi to rs such, in men with no symp to ms suggestive of severe pyelo (Muhammed 2017). Their analysis of 13 studies that evalu nephritis or prostatitis, 7 days may be considered until addi ated empiric therapy showed no statistically signifcant dif tional studies are conducted. The resistance rate to cef to lozane/tazo defnitive therapy indicated similar mortality rates at 15. Sixty-four patients were evaluated, and a such as colistin or tigecycline may be necessary (Sobel 2014). The optimal dosage of lated uropathogen, occurring at over 92% in both treatment colistin is an evolving to pic because of considerable interin groups. Overall, microbiological responses were similar for dividual variation in plasma concentrations, administration the ceftazidime/avibactam group and the imipenem/cilas of colistimethate (the prodrug of colistin), and increased risk tatin group at 70% and 71%, respectively (Vazquez 2012). However, tigecycline achieves low urinary and serum urinary source is a complex to pic with limited data and het concentrations because of a large volume of distribution; erogeneity of study designs. A study from the New York/New Jersey region, lysis by AmpC fi-lactamases (van Duin 2016). A urine culture tions presenting with signs of severe sepsis with hypoten should be obtained before initiation of antibiotic therapy, if sion or organ dysfunction must be treated with parenteral possible, from a newly placed catheter because the bacterial broad-spectrum antibiotics initially similar to acute compli bioflm on the existing catheter can render the culture results cated pyelonephritis. Treatment of asymp to matic ant diagnostic test, to gether with a physical examination candiduria with fuconazole effectively eradicates candiduria of the abdomen, external genitalia, perineum, and prostate initially, but 2 weeks after discontinuing therapy, the recur (Nickel 2011). Therefore, routine antifungal treatment of Acute Bacterial Prostatitis asymp to matic candiduria is not recommended, and treatment Acute bacterial prostatitis requires parenteral therapy initially is reserved primarily for patients undergoing urologic pro with bactericidal antibiotics, including broad-spectrum pen cedures. However, if candiduria persists and a deep-seated icillin, third-generation cephalosporin, or a fuoroquinolone infection is suspected, reasons for persistent candiduria (Grabe 2015; Nickel 2011). An aminoglycoside can be added to should be investigated by performing imaging studies. Flu the initial therapy and be continued until the patient becomes conazole is the only azole that achieves high urinary concen afebrile. Patients with candiduria with symp to ms of Candida prescribed for 10 days (Grabe 2015). For fuoroquinolone resistance Renal Transplant Recipients or in to lerance, trimethoprim is an appropriate alternative Urinary tract infections are the most common infectious because it has good penetration in to the prostate and high complications after kidney transplantation and are asso bioavailability; however, trimethoprim requires a longer treat ciated with poor allograft survival. In fact, compared culture should be obtained several days before the procedure, with those who received inhaled pentamidine or oral dapsone, followed by therapy with a third-generation cephalosporin or P. Bacteria involved in renal s to nes may enter the urine and to independently use bathrooms. In patients with not have a urinary catheter, dipsticks may be useful because negative preoperative urine cultures, pre or perioperative negative tests are associated with a low probability of bac antibiotic prophylaxis does not appear to reduce pos to pera teriuria. However, a meta-analysis of 24 6 months, or at least three infections within 1 year. Cranberry capsules are an option in preg Most recurrences are likely reinfection rather than relapse. The frequency of infections caused by Proteus, Pseudomonas, Other adhesin blockers such as d-mannose are used by Klebsiella, Enterobacter spp. Lac mg, or a dose of ciprofoxacin 250 mg) at the time of inter to bacillus appears to be promising as an antibiotic-sparing course; they should also avoid the use of a spermicide-con agent. Antibiotic prophylaxis Lac to bacillus and trimethoprim/sulfamethoxazole, respec should be considered a last resort after behavioral changes tively. Antimicrobial stewardship programs are essential to promote In acidic urine, methenamine is hydrolyzed to ammo appropriate antibiotic use to optimize therapeutic outcomes nia and formaldehyde, which has nonspecifc bactericidal and minimize adverse events (including the development of activity. Antimicrobial stewardship and urinary tional programs and cascade the reporting of antibiotic sus tract infections. Med Lett Drugs Ther for selected cases after positive urine cultures) within health 2016;58:75-6.
Purchase online loratadine
Endoscopic manipulation of ureteral calculi in children by rigid operative ureterorenoscopy allergy medicine for 9 year old order 10mg loratadine with visa. Lower calyceal and renal pelvic s to nes in preschool children: A comparative study of mini-percutaneous nephrolitho to my versus extracorporeal shockwave lithotripsy. Percutaneous management of renal calculi: experience with percutaneous nephrolitho to my in 60 children. Percutaneous nephrolitho to my in children: early and late ana to mical and functional results. Successful percutaneous nephrolitho to my in children: multicenter study on current status of its use, efficacy and complications using Clavien classification. Experience of percutaneous nephrolitho to my using adult-size instruments in children less than 5 years old. Modified Clavien classification in percutaneous nephrolitho to my: assessment of complications in children. Fac to rs affecting complication rates of percutaneous nephrolitho to my in children: results of a multi-institutional retrospective analysis by the Turkish pediatric urology society. Ultra-mini-percutaneous nephrolitho to my in pediatric nephrolithiasis: Both low pressure and high efficiency. Single-step percutaneous nephrolitho to my (microperc): the initial clinical report. Comparison of shockwave lithotripsy and microperc for treatment of kidney s to nes in children. A Comparison of 2 Percutaneous Nephrolitho to my Techniques for the Treatment of Pediatric Kidney S to nes of Sizes 10-20 mm: Microperc vs Miniperc. Ultrasound-guided micropercutaneous nephrolitho to my in pediatric patients with kidney s to nes. Early postureteroscopy vesicoureteral reflux-a temporary and infrequent complication: prospective study. Evaluation of Pos to perative Hydronephrosis Following Ureteroscopy in Pediatric Population: Incidence and Predic to rs. Retrograde intrarenal surgery monotherapy versus shock wave lithotripsy for s to nes 10 to 20 mm in preschool children: a prospective, randomized study. Percutaneous Nephrolitho to my vs Retrograde Intrarenal Surgery for Large Renal S to nes in Pediatric Patients: A Randomized Controlled Trial. Comparison of Retrograde Intrarenal Surgery and Micro-Percutaneous Nephrolitho to my in Moderately Sized Pediatric Kidney S to nes. Transperi to neal laparoscopic pyelolitho to my after failed percutaneous access in the pediatric patient. Robotic nephrolitho to my and pyelolitho to my with utilization of the robotic ultrasound probe. Laparoscopic Ureterolitho to my in Children: With and Without Stent Initial Tertiary Care Center Experience with More Than 1-Year Follow-Up. The process of formation of cystic dilatation of the vesical end of the ureter and of diverticula at the ureteral ostium. His to logy of upper pole is unaffected by prenatal diagnosis in duplex system ureteroceles. Clinico-pathological correlation in duplex system ec to pic ureters and ureteroceles: can preoperative work-up predict renal his to logyfi Efficacy of magnetic resonance urography in detecting renal scars in children with vesicoureteral reflux. Incontinence due to an infrasphincteric ec to pic ureter: why the delay in diagnosis and what the radiologist can do about it. Outcomes of endoscopic incision for the treatment of ureterocele in children at a single institution. Clinical evolution of vesicoureteral reflux following endoscopic puncture in children with duplex system ureteroceles. Ureterocele associated with ureteral duplication and a nonfunctioning upper pole segment: management by partial nephroureterec to my alone. Primary lower urinary tract reconstruction for nonfunctioning renal moieties associated with obstructing ureteroceles. Recent advances in the management of ureteroceles in infants and children: Why less may be more. Innovation in Robotics and Pediatric Urology: Robotic Ureteroureteros to my for Duplex Systems with Ureteral Ec to pia. Robot-assisted laparoscopic management of duplex renal anomaly: Comparison of surgical outcomes to traditional pure laparoscopic and open surgery. Dismembered extravesical reimplantation of dilated upper pole ec to pic ureters in duplex systems. A comparison between laparoscopic and retroperi to neoscopic approach for partial nephrec to my in children with duplex kidney: a multicentric survey. Early determination of androgen-responsiveness is important in the management of microphallus. Transdermal dihydrotes to sterone therapy and its effects on patients with microphallus. Congenital hypogonadotropic hypogonadism and micropenis: effect of tes to sterone treatment on adult penile size why sex reversal is not indicated. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. The effect of cli to ral surgery on sexual outcome in individuals who have intersex conditions with ambiguous genitalia: a cross-sectional study. The long-term outcome of posterior urethral valves treated with primary valve ablation and observation. A systematic review and meta-analysis of the effectiveness of fetal cys to copy as an intervention for congenital bladder neck obstruction. Early outcome following diathermy versus cold knife ablation of posterior urethral valves. Which patients are at higher risk for residual valves after posterior urethral valve ablationfi Comparative urodynamic findings after primary valve ablation, vesicos to my or proximal diversion. Bladder function associated with posterior urethral valves after primary valve ablation or proximal urinary diversion in children and adolescents. What is the effect of circumcision on risk of urinary tract infection in boys with posterior urethral valvesfi Controlled Outcomes for Achievement of Urinary Continence among Boys Treated for Posterior Urethral Valves. Risk fac to rs for end stage renal disease in children with posterior urethral valves. Impact of posterior urethral valves on pediatric renal transplantation: a single center comparative study of 297 cases. The incidental discovery of occult abdominal tumors in children following blunt abdominal trauma. Radiographic assessment of renal trauma: a 10-year prospective study of patient selection. Ureteropelvic junction disruption secondary to blunt trauma: excre to ry phase imaging (delayed films) should help prevent a missed diagnosis. Long-term followup and evaluation of primary realignment of posterior urethral disruptions. Postpubertal geni to urinary function following posterior urethral disruptions in children. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: a report by the American Society of Anesthesiologist Task Force on Preoperative Fasting. Comparison of blood glucose concentrations in children fasted for morning and afternoon surgery. Energy expenditure and fluid and electrolyte requirements in anesthetized infants and children. Perioperative crystalloid and colloid fluid management in children: where are we and how did we get herefi A prospective randomized blinded study of the effect of intravenous fluid therapy on pos to perative nausea and vomiting in children undergoing strabismus surgery.