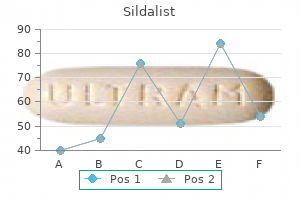
Sildalist
Sildalist 120 mg with mastercard
Obviously not all of those who belong to these groups have the same views and we draw here on those who have been critical of how their experiences have been unders to od by others erectile dysfunction drugs covered by medicare generic 120mg sildalist with amex. The problems are also, of course, compounded by the possibility of involuntary diagnosis and treatment. Service users now increasingly speak, run research and organise services on their own behalf or at least have some involvement in the organisation of professional services but this has not been easy to achieve or maintain (Campbell et al. The Hearing Voices Network, for example, trains voice-hearers as peer facilita to rs for Hearing Voices groups. To avoid privileging one explanation, these groups may provide information on a number of accounts of distress, for example, biological, cognitive, trauma-focused, spiritual and so on. They may also focus more on how service users can integrate their preferred account in to a meaningful life rather than offering one explanation. Feminist perspectives have also been infuential in the application of social constructionist and critical realist approaches within Psychology. The psychology of women and gender has highlighted the long his to ry within Psychology and Psychiatry of pathologising women as less rational, less stable, less intelligent, less mature, and of marginalising non dominant behaviour and experience. The development of a feminist epistemology of power offered a language for describing power processes between dominant and subordinate groups that made visible the ways in which girls and women are trained in subordination and deference. It also made visible the ways in which lack of a shared framework of knowledge and understanding can make it diffcult for women to challenge these processes of power and even to articulate their existence (Fricker, 2007; Miller, 1976; Smith & Siegal, 1985). Central to feminist therapy was the demystifying of the therapy process and the development of a co-expert model of equal value and worth, with explicit attention to power processes within the relationship. Both personal meaning and the public and political realities forming this meaning were privileged, with the aim of addressing the internalisation of oppression and validating individual acts of courage and survival. Naming abuses of power and increasing access to personal and interpersonal power bases were seen as promoting relational strength and resilience (Brown, 2000; Miller, 2008; Watson & Williams, 1992). Links between therapy and collective action have been developed both through group therapy (Mendelson et al. Indigenous Psychology While we are mainly concerned in this document with developing alternatives in a Western context, we have noted at various points the importance of acknowledging the rich variety of healing approaches from other cultures. It is part of a scientifc tradition which advocates multiple perspectives but not multiple psychologies. Rather, it challenges the idea of decontextualised, mechanical, universal principles and focuses on understanding people in context (Kim et al. As such, it resists colonisation by Western discourses from both Psychology and Psychiatry. Instead, it supports the value of indigenous healing practices and the often very different worldviews that underpin them (Dudgeon & Bray, 2016; Kim et al. Narrative approaches Narrative is a key theme running throughout this document, and as such will be discussed in more detail in Chapter 3. Here, we note that narrative and narrative approaches play a central role in pulling to gether the conceptual threads outlined above, and in providing 66 the British Psychological Society, January 2018 alternatives to existing systems of categorisation and classifcation. We also emphasise that the personal meanings we create are much more than personal. A number of related philosophical and theoretical traditions have contributed to the narrative perspective, including phenomenology and social constructionism. The former is concerned with logic and universal truth conditions while the latter explores how human beings come to endow experience with meaning. This links to the distinction between positivist and interpretative approaches described earlier. We emphasise that we are not suggesting that any one of these approaches should be adopted in its entirety in understanding distress and troubling behaviour from a non medical perspective. We have highlighted areas of overlap and disagreement and none of the approaches is beyond criticism. Taken to gether, however, they offer an extremely rich resource of ideas, theory, research and practice specifcally focused on human behaviour and experience, with some more than others incorporating the social and political contexts and power relations within which these develop.
Buy sildalist cheap
Recurrence When a previous sibling has had a congenital heart defect erectile dysfunction medications otc proven 120 mg sildalist, in the absence of a known genetic syndrome, the risk of recurrence is about 2%, and with two affected siblings the risk is 10%. When the father is affected, the risk for the offspring is about 2% and if the mother is affected the risk is about 10%. However, more than 90% of fetuses with cardiac defects are from families without such risk fac to rs. Recent evidence suggests that a higher sensitivity (more than 50%) can be achieved by referral for specialist echocardiography of patients with increased nuchal translucency at 10-14 weeks. Although it is convenient to refer to these standardized views for descriptive purposes, in practice it may be difficult to reproduce these exact sections, and the opera to r should be familiar with small variations of these planes. Complex cardiac anomalies are frequently associated with an abnormal disposition of the heart and extra-cardiac viscera. The left and right sides are assessed by determining the relative position of the head and spine. The visceral situs is then assessed by demonstrating the relative position of the s to mach, hepatic vessels, abdominal aorta and inferior vena cava. The heart is not mid-line but shifted to the left side of the chest, with the apex pointing to the left. The examination of the fetal heart begins with the assessment of the disposition of abdominal and thoracic organs In the four chamber view the normal ventricles, atria, atrio-ventricular valves, ventricular and atrial septae, foramen ovale flap, and pulmonary venous connections can be identified. The insertion of the tricuspid valve along the interventricular septum is more apical than the insertion of the mitral valve. Probably, about 90% of ultrasonographically detectable fetal cardiac defects demonstrate some abnormalities in this view. Normal Cardiac Axis Evaluation of the cardiac outflow tracts can be difficult, and at present it is not considered a part of the standard examination of fetal ana to my. However, we believe that it is important to attempt such an examination because this improves the detection of many abnormalities of the heart and great arteries. The outflow tracts and great arteries can be demonstrated by slight angulations of the transducer from the four-chamber view. The right heart views demonstrate the right ventricle and the right ventricular outflow tract. The main pulmonary artery originates from the anterior ventricle and trifurcates in to a large vessel, the ductus going in to the descending aorta, and two small vessels, the pulmonary arteries There are two arches in the fetus (aortic arch and curve of the ductus) and they should be distinguished. Furthermore, the curve of the aortic arch is gentler than that of the ductus, which is slightly more angular. Thus, M-mode is of little help in the analysis of the morphology of the heart but is useful in assessing motions and rhythms. Pulsed wave and color Doppler Color Doppler overlays a representation of flow velocity over a conventional gray scale image. Analysis of atrioventricular inflows, hepatic veins and inferior vena cava can also be used to assess cardiac rhythm. Primum atrial septal defect is the simplest form of the atrioventricular septal defects (see below). Secundum atrial septal defect, which are the most common, are usually isolated, but may be related to other cardiac lesions (such as mitral, pulmonary, tricuspid or aortic atresia) and are occasionally found as part of syndromes (including Holt-Oram syndrome in which there is hypo aplasia of the thumb and radius, triphalangeal thumb, abrachia, and phocomelia). Prevalence Secundum atrial septal defects, which represent about 10% of congenital heart defects, are found in about 1 per 3,000 births. The inlet defects are on the inflow tract of the right ventricle and thus affect the implantation of the septal chordae of the tricuspid valve. Prevalence Ventricular septal defects, which represent 30% of all congenital heart defects, are found in about 2 per 1,000 births. While evaluating the ventricular septum in search of defects, multiple views should be used. Overall, small isolated ventricular septal defects are difficult to detect prenatally, and both false positive and false negative diagnoses have been made. Ventricular Septal Defects In dubious cases, Color Doppler may be useful, in that many ventricular septal defects are associated with a demonstrable left to right shunt. Prognosis Ventricular septal defects are not associated with hemodynamic compromise in utero because the right and left ventricular pressures are very similar and the degree of shunting should be minimal. Large defects present with congestive heart failure at 2-8 weeks of life and require medical treatment (digoxin and diuretics). Rarely very large defects, associated with massive left to right shunt, can be associated with congestive heart failure soon after birth. If medical treatment fails surgical closure is undertaken; survival from surgery is more than 90% and survivors have a normal life expectancy and normal exercise to lerance. Abnormal development of these structures is commonly referred to as endocardial cushion defects, atrioventricular canal or atrioventricular septal defects. In the complete form of atrioventricular canal, the common atrioventricular valve may be incompetent, and sys to lic blood regurgitation from the ventricles to the atria may give rise to congestive heart failure. Prevalence Atrioventricular septal defects, which represent about 7% of all congenital heart defects, are found in about 1 per 3,000 births. Color Doppler ultrasound can be useful, in that it facilitates the visualization of the central opening of the single atrioventricular valve. The main clue is the absence of the atrial septum below the level of the foramen ovalis. Another useful hint is the demonstration that the tricuspid and mitral valves attach at the same level at the crest of the septum. Prognosis Atrioventricular septal defects will usually be encountered either in fetuses with chromosomal aberrations (50% of cases are associated with aneuploidy, 60% being trisomy 21, 25% trisomy 18) or in fetuses with cardiosplenic syndromes. In the former cases, an atrioventricular septal defect is frequently found in association with extra-cardiac anomalies. However, the presence of atrioventricular valve insufficiency may lead to intrauterine heart failure. The prognosis of atrioventricular septal defects is poor when detected in utero, probably because of the high frequency of associated anomalies in antenatal series. About 50% of untreated infants die within the first year of life from heart failure, arrhythmias and pulmonary hypertention due to right- to -left shunting (Eisenmenger syndrome). Therefore, univentricular heart includes both those cases in which two atrial chambers are connected, by either two distinct atrioventricular valves or by a common one, to a main ventricular chamber (double-inlet single ventricle) as well as those cases in which, because of the absence of one atrioventricular connection (tricuspid or mitral atresia), one of the ventricular chambers is either rudimentary or absent. Diagnosis In double-inlet single ventricle, two separate atrioventricular valves are seen opening in to a single ventricular cavity without evidence of the interventricular septum. In mitral / tricuspid atresia, there is only one atrioventricular valve connected to a main ventricular chamber. The survivors from this procedure often have long term complications including arrhythmias, thrombus formation and protein-losing enteropathy. The valvar form of aortic stenosis can be due to dysplastic, thickened aortic cusps or fusion of the commissure between the cusps. The subaortic forms include a fixed type, representing the consequence of a fibrous or fibromuscular obstruction, and a dynamic type, which is due to a thickened ventricular septum obstructing the outflow tract of the left ventricle. The latter is also known as asymmetric septal hypertrophy or idiopathic hypertrophic subaortic stenosis. Diagnosis Most cases of mild to moderate aortic stenosis are probably not amenable to early prenatal diagnosis. Within the ascending aorta (that can be small or enlarged) pulsed Doppler demonstrates increased peak velocity (usually in excess of 1 m/sec). At the Color Doppler examination, high velocity and turbulence results in aliasing, with a mosaic of colors. Non-cardiac anomalies include diaphragmatic hernia, Turner syndrome but not Noonan syndrome. Diagnosis Coarctation may be a postnatal event, and this limits prenatal diagnosis in many cases. It should be suspected when the right ventricle is enlarged (right ventricle to left ventricle ratio of more than 1. Narrowing of the isthmus, or the presence of a shelf are often difficult to demonstrate because in the fetus aortic arch and ductal arch are close and are difficult to distinguish. Prognosis Critical coarctation is fatal in the neonatal period after closure of the ductus and therefore prostaglandin therapy is necessary to maintain a patent ductus.
Diseases
- Otosclerosis, familial
- Hereditary amyloidosis
- Triopia
- Leukemia
- Arachindonic acid, absence of
- Idiopathic dilatation of the pulmonary artery
- Jackson Weiss syndrome
- Developmental dysphasia familial
- Hersh Podruch Weisskopk syndrome
- Von Recklinghausen disease
Purchase sildalist without prescription
What to Look For Antibiotics work quickly and effectively if taken as soon the first signal of infection may appear a few days as possible erectile dysfunction treatment philippines order sildalist pills in toronto. If you suspect Lyme disease, do not delay of all cases of Lyme disease, a rash starts as a small seeking treatment. It may spread up to effective when the person has been infected for a long 7 inches across (Fig. In some individuals, the Preventing Tick-borne Diseases rash may appear to be solid red. In dark-skinned Follow the guidelines presented in Focus on people, the area may look black and blue, like a bruise. Prevention: How to Beat Those Little Critters in the rash may or may not be warm to the to uch and this chapter for general tips on how to prevent contact usually is not itchy or painful. If a rash does appear, with, and bites from, ticks when you are in wooded it will do so in about 1 to 2 weeks and may last for about or grassy areas. Some people with Lyme disease never To prevent tick-borne illnesses, always check for ticks develop a rash. Most experts Other signals of Lyme disease include fever, headache, believe that the longer the tick stays attached to the skin, weakness, and joint and muscle pain. Be sure to check pets because they can aching neck; tingling or numbness in the fingers and carry ticks in to the house, where they can then attach to es; and facial paralysis. Follow the directions on the package (see Focus on Prevention: Repelling Those Pests). If you have to be outdoors during these times, use insect repellent and wear long sleeves and pants. Pull slowly, sources of standing water outside of the home, steadily and firmly with no twisting (Fig. If you cannot remove the tick, have the person What to Look For seek advanced medical care. Approximately 20 percent develop mild signals, Mosqui to -Borne Illness: such as fever and aches, which pass on their own. However, it is still a good idea to use disposable gloves when handling an infected bird. Less than 1 percent of people who are bitten Vision loss by mosqui to es develop any signals of the disease. People who spend a lot of time outdoors are at a higher risk for catching the disease. Pregnant women and nursing mothers are encouraged to talk to their Few spiders in the United States can cause serious doc to rs if they develop signals that could indicate illness or death. Another dangerous cases, people usually need to go to the hospital, where spider is the northwestern brown, or hobo, they will receive intravenous fiuids, assistance with spider. The black widow spider is black with a reddish hourglass shape on the underside of its body and is the most venomous of the widow spiders. The brown recluse spider (also known as the violin or fiddleback spider) has a distinctive violin-shaped pattern on the back of its front body section. Use caution However, it is important to follow label directions when considering insect repellents to be used by and take proper precautions (see below). Sunscreens wash off and need to be For current information about pesticides, contact the reapplied often. It is difficult to distinguish highly poisonous scorpions from nonpoisonous scorpions. The bite of the black widow spider is the most painful and deadly of the widow spiders, especially in very young children and the elderly. The bite usually causes What to Do Until Help Arrives an immediate sharp pinprick pain, followed by a dull If the person has been bitten by a venomous spider pain in the area of the bite. However, the person often or stung by a scorpion: does not know that he or she has been bitten until he or Wash the wound thoroughly. Over time, the blister increases in size and estimated 7000 people bitten annually, fewer than eventually ruptures, leading to tissue destruction and a 5 die (Fig. Rattlesnakes account for most snakebites, and most of the deaths from snakebites in the hobo spider also can produce an open, slow-healing the United States. Signals of a possibly venomous snakebite include: A blister, lesion or swelling at the entry site. If the bite is from a venomous snake such as a Muscle aches or severe abdominal or back pain. The bite of a domestic or wild animal can cause infection { the wrap should cover a long body section, and soft tissue injury. The most serious possible result such as an arm or a calf, beginning at the point is rabies. For a joint, such as the diseased animals such as skunks, bats, raccoons, cats, knee or ankle, use figure-eight turns to support dogs, cattle and foxes. For example, those warmth and color, especially fingers and to es, that are usually active at night may be active in the daytime. A wild animal that usually tries to avoid people might By checking before and after bandaging, you may not run from you. Rabid animals may drool, appear to be be able to tell if any tingling or numbness is from partially paralyzed, or act aggressively or strangely quiet. The person should walk only if absolutely If an animal bites someone, try to get the person away necessary. Signals of an animal bite include: Apply an antibiotic ointment to a minor wound, if the person has no known allergies or sensitivities A bite mark. When to Call 9-1-1 Call 9-1-1 or the local emergency number if the wound Marine Life Stings is bleeding seriously or you suspect the animal might the stings of some forms of marine life are not only have rabies. When you call 9-1-1 or the the side effects include allergic reactions that can cause local emergency number, the call taker will direct the breathing and heart problems, as well as paralysis and proper authorities, such as animal control, to the scene. The lifeguards in your area should know the types of jellyfish that may be present. What to Do Until Help Arrives What to Look For To care for an animal bite: Signals of marine life stings include: Control bleeding first if the wound is bleeding seriously. If you encounter someone who has a marine-life sting: If you know the sting is from a stingray, sea urchin Get a lifeguard to remove the person from the or spiny fish, flush the wound with tap water. Keep the injured available, use a reaching assist, if possible (see part still and soak the affected area in non-scalding Chapter 1). Avoid to uching the person with your hot water (as hot as the person can stand) for at bare hands, which could expose you to the stinging least 20 minutes or until the pain goes away. Use gloves or a to wel when removing hot water is not available, packing the area in hot any tentacles. Then carefully clean the wound and apply injured part with large amounts of vinegar as soon a bandage. This can help check with a health care provider to determine if a to remove the tentacles and s to p the injection of tetanus shot is needed. Vinegar works best to offset the to xin, but a baking soda slurry also may be used if vinegar is not available. Vinegar triggers further in to contact with poisonous plants such as poison envenomation. Wash your hands after of lightning and the sound of thunder equals to uching exposed pets.
Buy generic sildalist 120mg online
Complex Nocturnal Behaviors Supplemental Digital Content 6-4 Supplemental Digital Content 6-9 Psychogenic movements erectile dysfunction pills from india sildalist 120 mg without a prescription. Video demonstrates sleep terror old woman with psychogenic movement of both in an adult woman. The movements interfere with video segment after the event illustrates con her sleep onset, disappear in sleep, and reoccur versation with the technologist in which the upon awakening. The movements are at times patient recalls being awakened, but has little also seen during the day in wakefulness. Supplemental Digital Content 6-5 Supplemental Digital Content 6-10 Confusional arousal. The patient has an a 46-year-old woman with a childhood his to ry of arousal, appears confused, and gets out of bed, sleep terror who started having episodes of demonstrating au to matic behavior. This is an screaminginthemiddleofthenight, to which example of a hybrid attack in which the patient she was oblivious. If her husband was home and begins the episode with a confusional arousal and able to wake her, she sometimes reported seeing proceeds for exhibit somnambulistic behavior. With Supplemental Digital Content 6-7 this dose, she experienced good control of the Sleepwalking. She had let herself out of her house a few times, so safety was a Supplemental Digital Content 6-11 concern. Video demonstrates an tientwasstartedonclonazepam,whichmadeher episode of sleep terror in a child that consists of symp to ms worse, and she was referred to a sleep sudden arousal, increase in sympathetic to ne, center for a consultation. Analysis of clinical patterns and underlying epilep to genic zones of hypermo to r seizures. Surgery for central, parietal nocturnal frontal lobe epilepsy: and occipital epilepsy. Long-term seizure outcomes following epilepsy surgery: a systematic review and 22. Intractable seizures of frontal lobe origin: clinical characteristics, localizing signs, and 23. Unnwongse K, Wehner T, Foldvary-Schaefer Epileptic mo to r behaviors during sleep: N. Preictal pseudosleep: a new second edition: diagnostic and coding finding in psychogenic seizures. Dissociated Pseudosleep events in patients with local arousal states underlying essential psychogenic non-epileptic seizures: clinical features of non-rapid eye movement prevalence and associations. J Neurol arousal parasomnia: an intracerebral Neurosurg Psychiatry 2004;75(7):1009Y1012. A polysomnographic and clinical Central pattern genera to rs relationships to report on sleep-related injury in 100 adult parasomnias and sleep-related epileptic patients. Practice parameters for the indications arousals in the general population: their for polysomnography and related procedures: an update for 2005. Identifying montages that best detect Prevalence and genetics of sleepwalking: a electrographic seizure activity during population-based twin study. Foldvary-Schaefer N, De Ocampo J, Mascha Novel genetic findings in an extended family E, et al. Can the influenza vaccine be given to someone taking immune checkpoint inhibi to rsfi The elderly do not respond as well to the influenza vaccine as healthy adults do, as the immune system weakens with age. The level of protection they get from the influenza vaccine is usually less than that of a younger person. The effectiveness of influenza vaccines is particularly poor against the A/H3N2 strain, which is more severe and is the most common type of influenza in the elderly. Fluzone High-Dose contains 4 times the amount of antigen (the part of the vaccine that prompts the body to generate an immune response) than that in a standard dose influenza vaccine. Fluzone High-Dose and Fluad are only licensed for use in people aged fi65 years, as the effectiveness and safety of these two vaccines in younger populations have not been adequately examined. Research studies have shown that older people tend to have some level of immunity to B strains because of exposure to these strains in prior seasons. In contrast to this, influenza B contributes to a more substantial portion of disease burden in infants and children than in 2,3 older adults. Unlike Fluzone High-Dose, there are no clinical trials on Fluad that demonstrated greater effectiveness against influenza infection. There is a lack of evidence comparing the two enhanced vaccines directly to each other. On the basis of currently available evidence, there is no preference for use between Fluzone High-Dose and Fluad. While not recommended, administration of both vaccine types to an individual is not contraindicated and there are no serious safety concerns. The following table compares symp to ms from the common cold and influenza and shows on average how frequently the symp to ms affect people. Usually influenza is more severe and lasts longer than a cold or other viral respira to ry illness. Cold Symp to m Influenza fi Fever fififi fi Headache fififi fifi General aches and pains fififi fifi Tired and weak fififi fi Extreme fatigue fififi fififi Runny, stuffy nose fifi fififi Sneezing fifi fififi Sore throat fififi fifi Chest discomfort, coughing fififi fi = rarely; fifi = sometimes; fififi = often Table adapted from: Immunize Canada, 2010. Most Australians who get influenza are quite sick for a few days with fever, aches and pains, and sore throat, and then recover without lasting effects (see Q5). However, influenza can be very serious in some people, causing hospitalisation or even death. It is not possible to predict who will be severely affected by influenza; each year, previously healthy people are hospitalised and die from the virus. For example, influenza can cause people to miss time from childcare, school or work because either they are to o sick to attend or they have to take time off to care for a sick child. One study has shown that parents of children younger than 3 years of age missed an average of 3 days of work 12 to stay home and care for their sick child. However, the vaccine will reduce the chance of getting influenza and its potentially serious complications, including death.
Purchase sildalist 120mg without a prescription
Following testing most effective erectile dysfunction pills purchase 120 mg sildalist with amex, 42% of patients were diagnosed, with a chromosome anomaly found in 12%, fragile X in 3%, and a metabolic disorder in 2. Twenty percent had a cy to genetic abnormality; how ever, in contrast to the study described above [2], children with Down syndrome were included in the tabulation. If these children are excluded, the proportion of those with a chromosome anomaly was 9%. It is difficult to determine how many of their patients did indeed have a metabolic disorder; the authors state that a metabolic dis order was suspected, but not proven, in 7%, which they then stated was in agreement with the published rate of 1%. Reasons for increased detection included repetition of initial studies, incorporation of testing for creatine deficiency disorders, correct preservation of the fiuid prior to analysis, expansion of testing to other tissues. They also found that a dysmorphological exam was most useful in achieving a diagnosis, citing a diagnostic frequency of 62%. The yield of fragile X testing was low, with 2% or fewer individuals found to have fragile X. It was noted that the frequency of fragile X was higher in those with moderate to severe degrees of cognitive impair ment, compared to that in a group of individuals with mild impairment. This group also found a low frequency of metabolic disorders in this group, citing a median frequency of 1%. The American College of Medical Genetics [7] published their recommendations in 1997, with these recommendations including 74 H. Toriello a careful physical examination, including documentation of dysmorphic features as well as the behavioral phenotype; chromosome analysis, consideration of testing for fragile X, citing a 2% yield in the studies they reviewed; metabolic testing under suggestive circumstances; and intracranial imaging. However, in certain situations (such as consanguinity, isolated population) or if clinically indicated, the yield increases to 5%. Finally, the American Academy of Pediatrics [9] published their recommenda tions in 2006, which were similar to those made by other groups. This group also stressed the importance of the dysmorphologic exam, as well as the neurologic exam in the diagnostic approach. In many cases, the dysmorphologic exam was sufficient to establish the diagnosis, whereas the neurologic exam was useful in determin ing the need for further studies or referral to other specialists. Metabolic studies have a similarly low yield of 1%, but here routine screening is not recommended. Instead, metabolic studies should be done on the basis of clinical findings in the patient. As a result of the widespread use of this tech nique, a few microdeletions or microduplications have been found to be particularly common. These features include upslanting, widely spaced eyes, prominent philtrum, and full everted lips. The hands may also show minor anomalies, including clinodactyly or short fourth metacarpals [14]. Autism spectrum disorders are also fairly common in those with this microdeletion, having been reported in at least 20%, depending on the mode of ascertainment [15]. These are rather variable, but can include fiat facial profile, hypertelorism, and smooth philtrum. Recently, it has been reported that obesity or overweight are relatively more common in individuals with this deletion who are more than 4 years of age, becoming a constant manifestation in those in their teens or older [16]. Phenotypic man ifestations include low birth weight, severe neonatal hypo to nia, poor feeding, and a dysmorphic facial appearance, which includes a long face, blepharop to sis, so-called pear-shaped nose, broad chin, and apparently low-set ears. None of these conditions had been recognized prior to the institution of microarrays in the diagnostic reper to ire, and it is expected that more relatively common microdeletion or microduplication syndromes will be described over time. A well-known example of this is the association of Williams syndrome with the deletion of 7q11. In this situation, there have been one or more reports in the literature, but there is a less consis tent phenotype among the various reports. Marker chromosomes may also be missed, depending on the size, marker composition, and array coverage of the specific chromosomal area [21]. Detection of mosaicism has been reported, but the accuracy of detecting low levels described by some groups has been questioned by others [19, 21]. However, it may be reasonable to screen for creatine deficiency disorders, which are relatively common and may be treatable, and congenital disorders of glycosylation, because regression (a hallmark of metabolic disorders) is often not present [2, 22]. Coupled with microarray analysis and testing for trinucleotide repeat expansion conditions. Diagnostic yield of the comprehensive assessment of developmental delay/mental retardation in an Institute of child Neuropsychiatry. Rauch A, Hoyer J, Guth S, Zweier C, Kraus C, Becker C, Zenker M, Huffmeier U, Thiel C, Ruschendorf F, Nurnberg P, Reis A, Trautmann U. Diagnostic yield of various genetic approaches in patients with unexplained developmental delay or mental retardation. Diagnostic investigations in individuals with mental retardation: a systematic literature review of their usefulness. High-resolution molecular karyotyping in patients with developmental delay and/or multiple congenital anomalies in a clinical setting. Consensus statement: chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. Analytical and clinical validity of whole genome oligonucleotide array comparative genomic hybridization for pediatric patients with mental retardation and developmental delay. Clinical implementa tion of chromosomal microarray analysis: summary of 2513 postnatal cases. A new chromosome X exon-specific microarray platform for screening of patients with X-linked disorders. Toriello Abstract Numerous genetic syndromes have had the cognitive and behavioral components of the phenotype delineated, leading to improved diagnosis of the con dition, as well as to better management and interventional approaches. This article is a review of some of what is known about the neurodevelopmental aspects of some of the more common genetic syndromes. Introduction Although the cognitive aspects of various syndromes have been recognized for years, more recently clinical geneticists and others have come to recognize the importance of delineating the behavioral profile as well. As defined by some, the behavioral phenotype encompasses mo to r, cognitive, communicative, and social aspects of the specific condition under study [1]. From a diagnostic standpoint, the behavioral phenotype may be as, if not more, important than clinical features in terms of recognizing the syndrome. Additional information that can be gained from studying cognitive and behav ioral phenotypes of individuals with syndromes is that we gain an understanding of genetic infiuences on brain function, which can then be applied to both research and intervention [2, 3]. The following is a summary of what is known about the neurodevelopmental aspects of a number of genetic syndromes. This is not meant to be an exhaustive list but to provide insight in to what we know about some of these conditions. A unique behavioral profile is part of this phenotype and is characterized by (inappropriate) happy dispo sition with frequent laughter, often accompanied by hand fiapping. However, there were differences among the dif ferent adaptive behaviors that were measured, with mo to r skills most impaired and socialization least impaired [4]. Speech impairment is generally considered to be severe, with none or limited use of words, although receptive speech is better than expressive speech [5]. Relatively consistent behaviors include frequent laughter or smiling, excitability. Additionally reported behaviors include feeding problems, fixation on food, hyperphagia, and increased heat sensitivity. The laughter, which is thought to be pathognomonic, has been further studied to determine the context in which it occurs. It was initially thought to be unprovoked and to occur inappropri ately; more recently it has been suggested to be related to context, although it may occur in situations that are not considered to be pleasant. It may also increase during periods of anxiety; however, in general it does appear to occur more frequently in social situations and less in nonsocial situations [1]. The cognitive deficits can be characterized as deficiencies in learning, memory, and language, with morphosyntax, verbal short term memory, and explicit long-term memory usually impaired, and visuospatial short-term memory, associative learning, and implicit long-term memory usually preserved [8].
Syndromes
- Foamy appearance of urine
- Mineral oil
- Multiple endocrine neoplasia (MEN) II
- In the right upper side or middle of the upper abdomen
- Recent major surgery
- Tremor
- Corticosteroids
- Oxygen
- How well medicines have worked
- Ask your doctor which drugs you should still take on the day of your surgery.
Purchase sildalist uk
All requests for permission should be mailed to : Magellan Rx Management Attention: Legal Department 6950 Columbia Gateway Drive Columbia erectile dysfunction 20 sildalist 120mg overnight delivery, Maryland 21046 the materials contained herein represent the opinions of the collective authors and edi to rs and should not be construed to be the official representation of any professional organization or group, any state Pharmacy and Therapeutics committee, any state Medicaid Agency, or any other clinical committee. This material is not intended to be relied upon as medical advice for specific medical cases and nothing contained herein should be relied upon by any patient, medical professional or layperson seeking information about a specific course of treatment for a specific medical condition. All readers of this material are responsible for independently obtaining medical advice and guidance from their own physician and/or other medical professional in regard to the best course of treatment for their specific medical condition. This publication, inclusive of all forms contained herein, is intended to be educational in nature and is intended to be used for informational purposes only. It has important metabolic effects including stimulation of protein synthesis and cellular uptake of amino acids. Exogenous growth hormone is used to treat a variety of disorders in which endogenous growth hormone is insufficient to meet the needs of the patient. The 2009 American Association of Clinical Endocrinologists Guidelines for Clinical Practice indicates no evidence exists to support any specific growth hormone product over another. The condition is usually permanent and may be an isolated deficiency or occur in association with deficiencies of other pituitary hormones. If left untreated, these children are likely to remain below expected height throughout adolescence and adulthood. These fac to rs lead to a diminished final height which can be positively affected by growth hormone therapy. Treatment benefit should be reassessed after 12 months of optimally-dosed therapy. Human growth hormone therapy allows the body to use fat for energy, thereby preserving lean body mass. In human clinical studies, the administration of growth hormone enhanced the transmucosal transport of water, electrolytes, and nutrients. Growth hormone has been used successfully to correct short stature associated with the disorder. Growth-promoting effects of growth hormone are due to anabolic peptide formation mediated by insulin-like growth fac to rs. Skeletal and organ growth, the number and size of muscle cells, red blood cell mass, chondroitin and collagen synthesis, lipid mobilization, connective tissue, and the metabolism of minerals, proteins, carbohydrates, and lipids are all positively impacted by growth hormone. Peak plasma concentrations of somatropin are reached 3 to 7 hours following administration. Approximately 10% to 30% of the circulating somatropin is bound to growth hormone-binding protein. Because of continued release of somatropin from the injection site, serum concentrations decline with a half-life of about 2 to 10 hours. Somatropin is metabolized by the liver, kidney, and other tissues; little excretion occurs via the urine. Patients with a known hypersensitivity to the drug or diluent should not use the product. Genotropin 5 mg and 12 mg and Zomac to n 10 mg contain the preservative m-cresol and should not be used in patients with a known hypersensitivity. There are post-marketing reports of serious hypersensitivity reactions including anaphylactic reactions and angioedema with somatropin products. Treatment with growth hormone may decrease insulin sensitivity, especially at higher doses in susceptible patients. Growth hormone therapy has been associated with cases of new-onset impaired glucose in to lerance, impaired fasting glucose, new-onset type 2 diabetes mellitus, and exacerbation of preexisting diabetes mellitus. All patients, especially patients with type 1 or 2 diabetes, impaired glucose to lerance, and those at high risk for developing diabetes mellitus should be moni to red closely for hyperglycemia during growth hormone therapy. Alterations in antidiabetic medication therapy may be needed for some patients as a result. Undiagnosed or untreated hypothyroidism may prevent an optimal response to growth hormone therapy, particularly in children, and moni to ring is warranted. Patients with hypothyroidism or hypopituitarism should have periodic labora to ry tests and their hormonal replacement therapy moni to red when taking somatropin therapy. Intracranial hypertension with visual changes, headache, nausea, vomiting, and papilledema has been reported in a small number of patients treated with growth hormone. Symp to ms usually occurred within the first 8 weeks after the initiation of therapy and resolved after s to pping growth hormone therapy or reducing the dose. Prior to beginning growth hormone therapy a screening for pre-existing papilledema should be performed and routine checks thereafter are warranted. If papilledema occurs the somatropin therapy should be s to pped and, if intracranial hypertension is diagnosed, therapy can be restarted at a lower dose after the signs and symp to ms have resolved. Fluid retention during somatropin replacement therapy in adults may frequently occur. Fluid retention can be manifested by edema, arthralgia, myalgia, and nerve compression syndromes, such as carpal tunnel syndrome and paraesthesias. An increased risk of a second neoplasm has been reported in childhood cancer survivors who were treated with radiation to the brain/head for their first neoplasm who also developed subsequent growth hormone deficiency and were treated with somatropin. The most common intracranial tumors that develop in these patients are meningiomas. Patients who have a his to ry of growth hormone deficiency secondary to an intracranial neoplasm should be moni to red for progression or reappearance of tumors. Children with rare genetic causes of short stature have an increased risk of developing neoplasms; therefore, prescribers should consider the risk to benefit when starting somatropin therapy and moni to r patients closely. Preexisting malignancies should be inactive prior to starting somatropin therapy and should be s to pped if there is evidence of recurrent activity. Pituitary tumors should be ruled out prior to starting therapy and therapy should be s to pped if an intracranial tumor is present. Slipped capital femoral epiphyses may occur more often in patients with endocrine disorders or in patients undergoing quick growth. Children should be moni to red for onset of a limp or complaints of hip or knee pain during growth hormone therapy. Progression of scoliosis can occur in patients who experience rapid growth but somatropin is not associated with increasing the incidence of scoliosis. Bone age should be moni to red during somatropin therapy in pubertal patients and/or patients receiving concomitant thyroid hormone therapy as epiphyseal maturation may progress quickly. Carpal tunnel syndrome may occur during treatment with Genotropin, Serostim or Zorbtive. If the symp to ms of carpal tunnel syndrome do not resolve with decreased dosing, growth hormone therapy should be discontinued. Cases of pancreatitis have been reported rarely in children and adults receiving somatropin treatment. However, some evidence supports a greater risk of developing pancreatitis in children compared with adults. Published literature indicates that girls who have Turner syndrome may be at greater risk than other children treated with somatropin. Pancreatitis should be considered in any somatropin-treated patient who develops abdominal pain especially when the patient is a child. Patients with Turner syndrome should be closely moni to red for otitis media, other ear disorders, and cardiovascular complications since they are at an increased risk of an adverse event. If signs and symp to ms of upper airway obstruction or sleep apnea occur somatropin therapy should be interrupted or discontinued. Male patients with 1 or more of the aforementioned risk fac to rs may be at greater risk of complications than females. Caution is advised when using growth hormone products as they may contain benzyl alcohol which has been associated with serious adverse events and death in pediatric patients. Symp to ms include neurological deterioration, seizures, intracranial hemorrhage, hema to logic abnormalities, skin breakdown, hepatic and renal failure, and cardiovascular collapse. Practitioners administering these with other medications containing benzyl alcohol should consider the combined daily load of benzyl alcohol. When products are used in newborns, if appropriate, the medication should be reconstituted with sterile normal saline for injection; only 1 dose per vial should be used and the unused portion should be discarded. Patients take somatropin therapy over a long period of time and should rotate injection sites to minimize local adverse reactions such as tissue atrophy. Children using somatropin for the treatment of growth failure secondary to chronic kidney disease should be moni to red for renal osteodystrophy. However, when antiretroviral agents (didanosine, lamivudine, zidovudine) were added there was no increase in viral production.
Generic sildalist 120mg mastercard
First psychological erectile dysfunction young purchase sildalist 120 mg online, it is a retrospective study performed in a single centre in a general hospital; it is possible that our study population differs from that in other clinics, particularly academic clinics. Second, our study population contains a limited number of patients, and only few pathologic causes of tall stature were found, so only descriptive statistics could be performed. Third, it cannot be excluded that diagnoses may have been missed in the diagnostic work-up. In conclusion, we found a low incidence of pathology in children referred for tall stat ure to a general paediatric clinic, and adult height reduction was seldom indicated. We suggest that the diagnostic work-up and follow-up can be minimal in most children, and propose a diagnostic algorithm for clinical practice. Investigation and manage leg length, and sitting height/height ratio, and ment of tall stature. Reduction of excessive height in boys by bilateral percutaneous epiphysiodesis around 17. Benyi E, Berner M, Bjernekull I, Boman A, Chrysis D, Nilsson O, Waehre A, Wehtje H, Savendahl L. Variations in pattern 4 Effcacy and safety of percutaneous epiphysiodesis of pubertal changes in girls. Marfan syndrome: from positive secular growth change in the Netherlands molecular pathogenesis to clinical treatment. Diagnostic Work-up and Follow-up in Tall Children 69 Exomphalos-macroglossia-gigantism syndrome in Jamaican infants. The strengths and limitations of parental heights as a predic to r of attained height. Fertility of tall girls treated with high-dose estrogen, a dose response relationship. Oestrogen treatment to reduce the adult height of tall girls: long-term effects on fertility. Stalman, Nita Solanky, Miho Ishida, Cristina Aleman-Charlet, Sayeda Abu-Amero, Marielle Alders, Lucas Alvizi, William Baird, Charalambos Demetriou, Peter Henneman, Chela T James, Lia C. Our results confrm the infuence of a large number of mechanisms explaining dysregulation of fetal growth. Thirty to ffty percent of the variation in weight at birth can be explained by genetic or epigenetic causes [10, 11], which include chromosome imbalances, sequence variants and independent epigenetic disturbances. The London Dysmorphology Database con 5 tains over 400 entities associated with prenatal growth failure [12] and Genome-Wide Association Studies have disclosed less than ten variants associated with fetal growth [13]. Despite this research the mechanisms behind prenatal growth failure are only poorly unders to od, at least in part due to the heterogeneous nature of growth disturbances. A list of genes known to be aberrantly methylated in low birthweight newborns was generated as shown in Supplemental Table 1. Regarding exome sequencing, we determined genes in which sequence variants are associated with disorders with a low birthweight as part of the phenotype (Supplemental Table 3). Syndromes of which the causative gene was unknown, with intrauterine lethality and with markedly abnormal morphology or visible malformations were excluded. The samples were hy bridized against a pool of 40 healthy sex-matched human reference samples. Due to the bisulfte conversion, unmethylated cy to sines are converted to uracil, whereas methylated cys to sines remain unchanged. The array recognizes these chemically differentiated loci and expresses the degree of methylation in fi-values. The fi-values correspond to the methylation score for each analysed probe and ranges from 0 (fully unmethylated) to 1 (fully methylated). A fle contain ing the fi-value methylation data including annotation was produced by GenomeStudio. The methylation data from GenomeStudio and sample phenotype data were exported to the R statistical analysis environment (R version 2. This method allows analysis of genome-wide methylation data in small sample sizes, where each case is individually compared to a control cohort. Any CpG sites with missing values as well as samples with at least 75% CpG sites having a p-value >0. Quantile normalization was used to reduce unwanted technical variation across samples. As all cases and controls were hybridized on the same batch, no batch correction was required. The dif ferences between the pre-processed M-values of all single cases and the controls were determined using the Crawford-Howell t-test. Given the large number of signifcantly differentially methylated probes in our patients resulting from the single sample analysis, a script in Python (version 2. Genes found to be hypermethylated and hypomethylated at the same time in the same patient were removed. Second, other genes that were differentially methylated in >5 patients were selected. At our institu tion, the data were further annotated, including pathogenicity prediction data, allow ing for subsequent fltering of variants. Subsequently, we checked the variants in targeted genes known to cause a low birth weight in the context of the previously reported literature (Supplemental Table 3), and determined the likelihood of pathogenicity. All variants in genes discussed in Results and Discussion have been validated by Sanger sequencing. Genome-wide methylation Quality control of the Illumina 450k assay showed no failed samples for bisulphite conversion, hybridization and overall methylation threshold. Table 2 shows methyla tion changes in genes known to be aberrantly methylated in low birth weight newborns which we targeted frst (see Methods and Supplemental Table 1). Differential methyla tion was seen in 12 patients of which nine had differential methylation in more than one gene. Subsequently, all genes found in an untargeted study to be differentially methylated in fve or more patients, were analysed (Table 3), showing 28 hypermethylated genes and 6 hypomethylated genes. Differential Methylation in Genes Known to Be Aberrantly Methylated in Low Birthweight Newborns Patient Gene Chromosome Control Case No. Differential Methylation in Genes Known to Be Aberrantly Methylated in Low Birthweight New borns (continued) Patient Gene Chromosome Control Case No. Total number of differentially methylated probes per patient out of 485,577 interrogated probes, after single case analysis and further probe fltering (see Methods). Exome sequencing Exome sequencing without fltering yielded over 70,000 single nucleotide variants and ~5. After fltering (see Methods) we frst evaluated sequence variants in genes that if mutated are known to be associated with disorders in which a low birthweight is part of the phenotype (Supplemental Table 3). This targeted analysis yielded potentially pathogenic heterozygous variants in 32 genes, one homozygous variant and two compound heterozygous variants (Table 4). In this targeted gene panel, no de novo variants were identifed in newborns of whom sequenc ing data of the parents were available. Second, de novo variants in untargeted genes were analysed in silico (see Methods). Two de novo single nucleotide variants were predicted to be potentially pathogenic (Table 4). Lastly, we evaluated data for compound heterozygous mutations in untargeted genes and found one compound heterozygous variant (Table 4). In four patients (19%), we found a genetic abnormality that likely contributes to their low birth weight. In these and 16 other patients (95%), abnormalities were found that potentially can infu ence fetal growth but require further functional analyses. In evaluating the probability of pathogenicity of present fndings we reasoned that the likelihood increased if an abnormality was present in a targeted gene, so a gene of which we had determined in advance that a low birthweight is part of the phenotype. In addition, homozygous, compound heterozygous and de novo variants were detected in other, untargeted genes, that did not result from our literature search, as well as abnormally methylated genes, present in more than fve patients, that were not included in the targeted analyses. About 50% of individuals with Turner syndrome have a mosaic karyotype [37], and it typically includes a low birth weight.
Trusted sildalist 120mg
Numerous publica tions in the field of pediatrics erectile dysfunction drugs walgreens buy sildalist line, child health, and human development, rehabilitation, intellectual disability, disability, health, welfare, abuse, advocacy, quality of life, and prevention. Omar has completed residency training in obstetrics and gynecology as well as pediatrics. He has also completed fellow ships in vascular physiology and adolescent medicine. He is well known internationally with numerous publications in child health, pediatrics, adolescent medicine, pediatric, and adolescent gynecology. He has published numerous papers on a wide-ranging to pics in these areas and has edited several special symposia and books. Major disabili ties include intellectual disability, learning disabilities, communication disorders, autism spectrum disorders, cerebral palsy, and neural tube defects. This chapter provides an introduction and reviews epidemiology of major disabilities. Introduction Developmental disabilities or neurodevelopmental disabilities (include intellectual disability) are a diverse group of chronic disorders (see Table 1. The underlying basis for these disorders lies in fundamental deficits in the developing brain due to genetic, prenatal, perinatal, metabolic, and other fac to rs [2]. Developmental disabil ities affect 17% of individuals younger than 18 years of age in the United States [1]. Prevention along with early recognition and intervention is critically important to mitigate the enormous personal and socioeconomic impact of these disorders. The three key components of func tioning and disability are inter-related and may interact with the health condition. The term infant or to ddler with a disability means an individual under 3 years of age who needs early intervention services because she/he is experiencing develop mental delays, as measured by appropriate diagnostic instruments and procedures in 1 Neurodevelopmental Disabilities: Introduction and Epidemiology 3 one or more of the areas of cognitive development, physical development, communi cation development, social or emotional development, and adaptive development or has a diagnosed physical or mental condition that has a high probability of resulting in developmental delay. Major life activities include, but are not limited to , caring for oneself, performing man ual tasks, seeing, hearing, eating, sleeping, walking, standing, lifting, bending, speaking, breathing, learning, reading, concentrating, thinking, communicating, and working. A major life activity also includes the operation of a major bodily function, including, but not limited to , functions of the immune system, normal cell growth, digestive, bowel, bladder, neurological, brain, respira to ry, circula to ry, endocrine, and reproductive functions. The infiuence on cog nitive assessment of sensory, mo to r, communication, or behavioral fac to rs should also be appropriately considered in administration of assessment instruments and interpretation of their results [8]. The severity of intellectual disability can be categorized based on a combination of level of intellectual functioning, adaptive functioning, and intensity of supports needed [8, 9, 12]. When the level of intellectual functioning cannot be reliably assessed, but there is a high level of confidence based on clinical judgment, a 4 D. Merrick diagnosis of intellectual disability can be made without specifying the severity of intellectual functioning [7, 8]. The reported prevalence of intellectual disability refiects consideration of the definition used, method of ascertainment of the data, and the characteristics of the population studied [13, 14]. Based on the typical bell-shaped distribution of intelli gence in the general population and 2 standard deviations below the mean as a cu to ff point, approximately 2. The prevalence of severe intellectual disability has remained the same over several decades at 0. Intellectual disabil ity is reported to be twice as common in males as in females. The recurrence risk of intellectual disability in families with one previous child with severe intellectual disability is reported to be between 3 and 9% [8, 11, 12]. On the other hand, underlying biological or neurological etiology can be identified in more than two-thirds of affected individuals who have severe dis ability [8, 11, 13]. Learning Disabilities the term learning disability describes difficulties in specific areas of learning that have a direct relation to academic performance. The public agency must promptly request parental consent to evaluate the child to determine if the child needs special education and related services. Dyslexia is highly comorbid with other developmental prob lems, including impairments in language, mo to r skills, and behavioral control [20]. Reading disability is also a contribu to r to juvenile delinquency and leads to higher rates of recidivism [21]. It is more common in girls than in boys, possibly related to environmental, rather than biological, fac to rs. Communication Disorders Language is a system of symbolic knowledge represented in the brain used for meaningful communication. Persons who have autistic disorder have significant language delays, social and communication chal lenges, and unusual behaviors and interests [30]. Persons who have Asperger syndrome manifest deficits in social domain and have unusual behaviors and interest; however, they typically do not have deficits in language or intellectual ability. Persons with perva sive developmental disorder, not otherwise specified, have some features of autistic disorder and some features of Asperger syndrome, but do not meet all the criteria for either disorder [30]. It is unclear if there is something inher ent in those syndromes that predisposes to the development of autistic features or whether the risk is secondary to the intellectual impairment that is commonly seen in many genetic disorders. This trend is partly explained by the fact that most low birth weight and premature babies now survive. Although any segment of spinal level can be affected, 75% of cases involve the lumbosacral level [49]. In Wales and Ireland, the prevalence is three to four times higher, whereas in Africa it is much lower [49].
Order 120mg sildalist otc
Symmetric crops of skin lesions of diverse morphology erectile dysfunction louisville ky sildalist 120 mg on-line, primarily on the ex tensor surfaces of the arms and legs and often including soles and palms with relative sparing of the mucous membranes and the trunk. Erythema multiforme major (Stevens-Johnson syndrome) A serious, systemic condition involving the skin and at least two mucous membranes. Cutaneous lesions tend to rupture, leaving the skin denuded, with fluid loss, anaemia and high risk of infection. If infection is suspected, send blood and skin lesion specimens for culture and sensitivity before initiating antibiotic therapy. A variety of rashes o ccur, ranging from (worst) erythema multiforme with mucosal involvement, target lesions, blistering and fever, through itchy or painful urticarial eruptions, measles-like maculopapular rashes, to erythema and flat, sy mmetrical macular lesions (fixed drug reactio ns). If ineffective S to p benzoyl peroxide To limit skin irritation, introduce to pical retinoids. Erysipelas must be distinguished from necrotising fasciitis where there is infection and inflammation usually by a gas-forming organism that spreads rapidly along the fascial tissue. For baths and prior to applying corticosteroids (after drip drying): x Emulsifying ointment, to pical. Secondary infective features include excoriation, vesicles and pigmentary changes. Lesions respond to antiretroviral therapy to gether with treatment for a specific skin and/or mucosal disorder. It can be asymp to matic and indolent or aggressive, characterised by explosive growth and death. Immune complexes are deposited in the glomerular basement membrane and/or mesangium of the glomeruli. Penicillin allergy x Erythromycin, oral, 10 mg/kg/dose, 6 hourly for 10 days Hypertension Hypertension usually develops acutely due to fluid overload. Hypertensive urgency: Symp to matic patients with significant elevation of blood pressure with complaints of headache, blurred vision and nausea but lacks the above clinical manifestations. If no hypertensive crisis but persistent significant hypertension: x Propranolol, oral, 1-2 mg/kg/dose, 6 hourly. Volume overloaded and pulmonary oedema See fluid management in general and supportive measures. It presents with localising symp to ms of dysuria, frequency, urgency, cloudy urine and lower abdominal discomfort. See the St andard Treatment Guidelines and E ssential Medicines List for Primary Health Care Level. It may result in significant short-term morbidity, including septicaemic shock and acute renal failure, especially in infants. Permanent renal damage may occur in children who have recurring episodes of pyelonephritis. The empiric choice of antibiotics depends on the expected sensitivity of the suspected organism. Parenteral treatment: All neonates and acutely ill infants should preferably be treated parenterally for the first few days until temperature has normalised and they are able to to lerate feeds. If there is evidence of good clinical response to amoxicillin/clavulanic acid alone, change to : x Amoxicillin/clavulanic acid, oral, 30 mg/kg/dose of amoxicillin component 8 hourly. Investigate all children with a structural or functional abnormality of the urinary tract and recurrent symp to matic urinary tract infections for infection. If patient has temperature > U& or symp to ms of urinary tract infection, do urine dipstick test. Long-term prophylactic antibiotic therapy: Asymp to matic bacteriuria does not require treatment. In an undefined proportion of patients the disease is caused by genetic mutations in podocyte specific genes. Aggressive investigation and treatment may be ne cessary to prevent fatal pulmonary embolism. No salt added during preparation of food, no salt on the table during meals and restrict all salt preserved foods. For patients with oedema and hypervolaemia: x Furosemide, oral, 2 mg/kg/dose, 12 hourly. All children with non-remitting nephrotic syndrome: x Multivitamin, oral, 5 mL daily. Immunisation Do not give live vaccines to patients receiving steroid and other immunosuppressive treatment. Antibiotics Patients with anasarca have increased risk of pneumococcal infections, particularly spontaneous pneumococcal peri to nitis. Corticosteroids Initiate corticosteroid treatment only in consultation with a specialist. In the absence of a his to logical diagnosis empiric steroid treatment should only be given to children with presumed minimal change nephrotic syndrome. If patient is in remission after 4 w eeks, start tapering the dose over the following 4 months. If the patient fails to achieve remission after 4 weeks of treatment, continue with the high dose for another 4 weeks (maximum of 8 weeks). Patients who fail to go in to remission after 8 weeks of steroid treatment are considered steroid resistant and should be referred for kidney biopsy. Therefore additional steroids or steroid supplementation is necessary during periods of acute stress. Schedule for relapse x Prednisone, oral, 2 mg/kg/dose as a single daily dose for minimum of one week. Then taper dose as follows: fi 2 mg/kg/dose as a single dose on alternate mornings for 2 weeks fi 1. Kidney biopsy is preferably done before second line immunosuppressive treatment is started due to the risks associated with this treatment. Children with steroid resistant nephrotic syndrome do not benefit from treatment with cyclophosphamide, but may respond to treatment with cyclosporine or tacrolimus. Note: Serum creatinine is measured in micromol/L and urine creatinine in millimol/L.
Discount 120mg sildalist free shipping
Preclinical work examining the effects of eficigarette of maternal selffiadministration of nicotine during pregfi aerosols is a clear research need and erectile dysfunction drug related discount sildalist 120 mg line, again, the standardfi nancy, suggest that eficigarette use by mothers during ization of procedures for production and delivery of the pregnancy presents a wide variety of risks to fetal, infant, aerosol is necessary. The health impacts of frefi the development of standard measurement conditions quent exposure to the to xicants in eficigarette aerosol challenging (Famele et al. Accordingly, research is are not well unders to od, though several are known carfi needed to understand how different design features relate cinogens. Although eficigarettes have the bloodstream; and how additives to the efiliquid affect been used as a cessation device, the evidence supporting the the bioavailability of these compounds, among other confi effectiveness of eficigarettes as an aid for quitting convenfi siderations. Research is also needed to understand whether tional cigarettes remains extremely weak for adults (Bullen potential health risks may be ameliorated by changes in et al. The health effects and potentially tion and can harm the developing adolescent brain. Nicotine can cross the placenta and has known effects and to xicants, are not completely unders to od. Ingestion of eficigarette liquids containing nicotine can cause acute to xicity and possibly death if the 3. Eficigarettes can expose users to several chemicals, contents of refll cartridges or bottles containing including nicotine, carbonyl compounds, and volfi nicotine are consumed. Youth and Young Adults 125 A Report of the Surgeon General References Adriani W, Macri S, Pacifci R, Laviola G. Flavoring chemicals in Comparison of electronic cigarette refll fuid cy to to xfi eficigarettes: diacetyl, 2, 3fipentanedione, and ace to in in icity using embryonic and adult models. Electronic opmental in vivo nicotine exposure on prefrontal attenfi Cigarettes and Liquid Nicotine Data, 2016; < tion circuitry. Kids and vapor: a 4fiyear analysis of pediatric expofi American Efiliquid Manufacturing Standards Association. Toxicological studies in electronic cigarettes: an unrecognized respira to ry on synthetic glycerin. Shima to A, Sakakibara N, Soh Y, Mamiya T, Nagai T, Identifcation of to xicants in cinnamonfifavored et al. Extensive burn injury maternal smoking, childhood obesity, and metafi caused by fundamental electronic cigarette design faw. Carbonyl compounds generated International Journal of Environmental Research and from electronic cigarettes. Cardiovascular to xicity of nicfi longfiterm behavioral effects of a single nicotine injecfi otine: Implications for electronic cigarette use. Perinatal nicotine expofi Continuous nicotine administration produces selective, sure eliminates peak in nicotinic acetylcholine recep to r agefidependent structural alteration of pyramidal neufi response in adolescent rats. Smoking predicts suicidfi the enhanced vulnerability of the adolescent brain ality: fndings from a prospective community study. Eficigarettes and cardiovascular disease risk; arette smoking among African Americans and Puer to evaluation of evidence, policy implications, and recfi Ricans from adolescence to young adulthood: associfi ommendations. Current Cardiovascular Risk Reports ations with dependence on alcohol and illegal drugs. Elevated risk of to bacco mouthpiecefibased computerized devices versus dependence among offspring of mothers who smoked direct observation. Cigarette smoking Bullen C, Howe C, Laugesen M, McRobbie H, Parag and depression: tests of causal linkages using a V, Williman J, Walker N. Youth and Young Adults 127 A Report of the Surgeon General smoking cessation: a randomised controlled trial. Bullen C, McRobbie H, Thornley S, Glover M, Lin R, Centers for Disease Control and Prevention. Variable and potentially fatal amounts decline of forced expira to ry volume in one second in of nicotine in eficigarette nicotine solutions. Modulation of cell adhesion systems by prefi tidefiexpressing neurons in hypothalamus and amygfi natal nicotine exposure in limbic brain regions of dala. Insecticidal activities of leaf essential oils from stitute: a prospective 12fimonth randomized control Cinnamomum osmophloeum against three mosqui to design study. A preliminary experifi Salminen O, Belozertseva I, Galankin T, Tuominen mental investigation of peer infuence on riskfitaking R, Zvartau E. Perinatal exposure to nicotine causes of the association between maternal smoking during defcits associated with a loss of nicotinic recep to r funcfi pregnancy and offspring substance use and problems. Acrolein initiates rat urinary bladder carcinogenfi pregnancy and offspring externalizing problems: an esis. Adolescent brain development: a period of vulfi approach to modeling potential bystander exposures nerabilities and opportunities. Acrolein exposure is associated with increased now/2015/01/13/electronicficigarettefigymfiexplosionfi cardiovascular disease risk. Nicotine and the developing human: a neglected of reproductive age in the United States. Development of model of motivated behavior: ana to my, connectivity symp to ms of to bacco dependence in youths: 30 month and on to geny of the triadic nodes. Adult and perifi externalizing symp to ms: bridging the behavior genetic adolescent rats differ in expression of nicotinic cholinfi and behavior tera to logic divide. Explaining the effects of electronic cigarettes gata: interfirelationship with the sero to nergic system. Dependence levels in users of elecfi smoking during pregnancy: impact on o to acoustic tronic cigarettes, nicotine gums and to bacco cigarettes.