
Viagra Extra Dosage
Generic viagra extra dosage 120mg otc
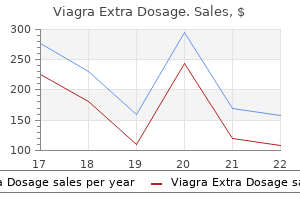
Since ca eine and ephedrine correct both the obesity theophylline made by Ciba-Geigy was twice as e ective 334 Greenway and Heber in raising resting metabolic rate in lean and postobese with ephedrine impotence nitric oxide buy generic viagra extra dosage 150 mg on-line. Although there was no with ephedrine maintained their weight loss to the end change in 24-hr energy expenditure in lean subjects of trial at week 50 (73). Seventy ve percent of the measured in a metabolic chamber, the postobese in weight loss was explained by anorexia, and 25% was creased their energy expenditure by 8%. Since acute methylxanthine combination normalized the defective treatment with ca eine 200 mg and ephedrine 20 mg thermogenic response to a meal in the postobese (69). There was no signi cant change in heart mg/200 mg, 20 mg/100 mg, and 20 mg/200 mg). Ephed rate, blood pressure, blood glucose, insulin, cholesterol, rine 20 mg with ca eine 200 mg gave increases in oxygen or side e ects relative to placebo, but weight loss was consumption that were greater than the sum of the greater in the ephedrine, ca eine, and aspirin group increase seen with ephedrine 20 mg and ca eine 200 (76). The acute dose of ca eine and was not di erent, but the group on ca eine and ephed ephedrine elevated systolic blood pressure 9 mm Hg and rine lost 4. This acute e ect of expect, the fall in energy expenditure was 13% in the ca eine and ephedrine in raising blood pressure, pulse, placebo group and only 8% in the group treated with and glucose is lost with chronic treatment (66). The Ephedrine with or without a methylxanthine was ca eine with ephedrine group lost 17. Side e ects of tremor, stimulating thermogenesis was lost after 1 week of insomnia, and dizziness reached the levels of placebo treatment, but was restored by combining it with ami by 8 weeks, and blood pressure fell similarly in all four nophylline for 1 week (79). Heart rate rose in a statistically signi cant trials with ephedrine alone give more weight loss than manner in the ephedrine group compared to placebo, placebo early in trial that decreases with time unless but fell below the baseline value in the ca eine and combined with a methylxanthine. Two weeks after cessation of the reported a 20-week, double-blind, placebo-controlled 24-week trial, headache and tiredness were more fre and randomized clinical trial of ca eine and ephedrine quent in the group that had taken ca eine with ephed in 32 adolescents age of 16 F 1 years and Tanner stage rine. The loss of Herbal and Alternative Approaches to Obesity 335 initial body weight was 14. All three dropouts were in the placebo group, and percentage of the total number of subjects studied. After the Since one trial compared ca eine and ephedrine to rst 4 weeks the adverse events in the ca eine group diethylpropion and another to dexfen uramine, some were not di erent than placebo. The raw 2 kg/m, the weight loss was greater with ca eine and dropout rates, however, do not re ect the reasons for ephedrine treatment. Ca eine and ephedrine are unique in that the side the subjects treated with dexfen uramine had more e ects return to placebo levels by 8 weeks and remain at gastrointestinal symptoms (diarrhea, dry mouth, and placebo levels at least to 24 weeks despite subjects re thirst), and the subjects treated with ca eine and ephed maining on the compounds (72) (Fig. Therefore, the rine had more symptoms of central nervous system incidence of adverse events may overestimate their true stimulation (tremor, insomnia, agitation). Symptoms clinical signi cance in obesity studies, since obesity is a in both groups declined by the end of the rst month of chronic disease and one for which chronic treatment is the 15-week trial (82). Catechins in green tea (see below) are Although dexfen uramine is no longer available synergistic with ca eine in stimulating thermogenesis owing to cardiac valvular toxicity, ca eine and ephed in man. No adverse e ects were detectable, even with rine are available without prescription. The cardiac acute dosing of ca eine with catechins in a study per valvular problems associated with fen uramine and formed in a metabolic chamber (85). Fen Two-thirds of 225 subjects were randomized to receive uramine with phentermine, fen uramine, with mazin ca eine and ephedrine for 12 weeks, and the rest were dol, and ca eine with ephedrine and mazindol alone randomized to placebo. At 12 weeks, rine was found to be the most cost-e ective treatment however, weight gain was less in the ca eine and ephed (83). One hundred thirty-six overweight nor momanometry, or continuous electrocardiographic re motensive or drug-controlled hypertensive subjects ran cording. The antihypertensive e ect of beta-blocker medica of human obesity is summarized in Table 1. The safety of ca eine and ephedrine in human Normotensive patients treated with ca eine and ephed obesity studies are summarized in Table 2, which rine had a 4. Start D/P End D/P Dose (E/C) Length D/P D/P Comments (3) 49/33 42/31 80/300 mg/d 12 wk 8. The number of subjects that started and nished the studies in the drug (D) and placebo (P) groups are listed. The study length is given, and the weight lost in kilograms and/or percent initial body weight lost is also given. The mean loss of plements (93), obesity management (94), energy balance weight of 4 kg was signi cant for all groups (87). Ca eine was combined with phenylpropanolamine Ca eine and ephedrine have been included in recent in the past to treat obesity (88). Thermogenic ergistic or even additive to phenylpropanolamine in approaches to treat obesity have been reviewed (103). This is in In a letter to the editor of the journal in which the clinical contradistinction to ca eine and ephedrine that do give trial was published, the authors reported that ephedrine more weight loss when combined than either compound alone, on reanalysis, actually gave more weight loss than induces alone. The addition of ca eine to ephedrine in a placebo, but less than ephedrine and ca eine, in the 24 6-month trial blocked the rise in pulse rate seen with week trial of ca eine, ephedrine, ca eine with ephed ephedrine alone (72). Ca eine and ephedrine have of ca eine has been reviewed (90), and nonprescription also been used to induce weight loss prior to comparing appetite suppressants including ca eine have also been di erent weight maintenance diets (109). Ephedrine products are sold without a prescription Ephedrine has been proposed as an adjunct to cog for the treatment of asthma and have a recommended nitive restructuring (92). Ca eine sold without a pre in reviews relative to nonprescription weight loss sup scription has a recommended dose up to 1600 mg/d. The Herbal and Alternative Approaches to Obesity 337 Table 2 Adverse E ects Symptom C&E No. Pharmaceutical grade prod dations up to 100 mg/d of ephedrine equivalent as ucts have greater potency than the herbal products ephedra. The ca eine content of these herbal products containing ca eine and ephedrine in equivalent doses containing ca eine and ephedrine varies, but is <600 because the herbal products contain some of the less mg/d. The peer-reviewed literature Table 3 Subjects Withdrawn from the Ca eine and Ephed Table 4 Adverse Events Responsible for Withdrawal Listed rine Trials for Subjects Participating in Ca eine and Ephedrine Trials Adverse event C&E Placebo Dexfena Ref. Each study is identi ed by reference list this table lists the reasons given for study withdrawal in subjects number. The bottom row on the table expresses the dropout incidence dropping out for adverse events during the ca eine (C) and inpercentfollowedbythenumberofsubjectswhodroppedoutandthe ephedrine (E) trials. The bottom row lists the incidence of dropouts total number of subjects in the trials. There was one trial in which for adverse events described in the trials followed by the number ca eine and ephedrine were compared to 50 subjects on diethylpro withdrawing and the number in the trials. When large numbers of the public use any product, adverse events can be associated with the use of the product, but establishing that there is a cause-and-e ect relationship of these adverse events to the product should be required prior to the withdrawal, prohibition, or licensing of such products. B Green Tea Catechins Green tea prepared by heating or steaming the leaves of Camelia sinensis is widely consumed on a regular basis throughout Asia. Black tea is made by allowing the green tea leaves to auto-oxidize enzymatically, leading to the conversion of a large percentage of green tea catechins to thea avins. The catechins are a family of compounds including epigallocatechin gallate, considered to be the Figure 1 Incidence of adverse events with ca eine and most potent antioxidant in the family of compounds. The incidence of adverse events (dizziness, decrease the odds ratio of su ering a myocardial ifarc tremor, headache, depressed mood, anxiety, euphoria, in tion to 0. These somnia, postural hypotension, palpitation, and tachycardia) compounds are avonoids in the class of polyphenols were mild and transient and reached the placebo level at 8 and have many activities including inhibition of the weeks where they remained for the rest of the trial. The catechins appear to be able to enhance sympathetic nervous system activity documents central nervous system stimulation, an in at the level of the fat cell adrenoreceptor. In vitro, a crease in pulse, an increase in blood pressure, and an green tea extract containing both catechins and ca eine increase in glucose when ca eine and ephedrine are was more potent in stimulating brown adipose tissue given acutely either separately or together. These side thermogenesis than equimolar concentrations of caf e ects disappear with chronic treatment and are no feine alone (112). The pulse rate in orally administered to mice over a 10-week period that trial was no di erent from placebo in the ca eine during high-fat feeding. Mean food consumption was and ephedrine group, but was signi cantly higher than not di erent between the groups, but oolong tea pre placebo in the ephedrine group. There were no di er vented the obesity and fatty liver induced by the high-fat ences between the ca eine with ephedrine group and the diet. Noradrenaline-induced lipolysis was shown to placebo group relative to serum glucose, serum choles increase and pancreatic lipase activity to be inhibited terol, or symptoms of stimulation. Since ca eine occurs naturally Ephedrine and ca eine have each been sold for years in green tea extract, it has been di cult to separate the without a prescription for the treatment of asthma and e ects of green tea from ca eine in humans.
Discount viagra extra dosage uk
Clinical practice guideline for the eradicating therapy of Helicobacter pylori infections associated to duodenal ulcer in primary care erectile dysfunction treatment nj buy discount viagra extra dosage 200mg. Current concepts in the management of Helicobacter pylori infection: the Maastricht 2000 Consensus Report. Alberta Society of Gastroenterology consensus statement: Helicobacter pylori in peptic ulcer disease. Canadian Helicobacter Study Group consensus conference on the approach to Helicobacter pylori infection in children and adolescents. Various causes include adverse physiologic adaptations of the gut during exercise; G excess ingestion of carbohydrate drinks, alcohol, and anti-inflamma tory medications; emotional stressors; exposure to pathogens in closed envi ronments and during travel; trauma; and abdominal wall pressure overload. Vigilance for such conditions is essential; however, timely diagnosis and treatment can be delayed as most athletes have enhanced pain tolerance, often do not verbalize their symptoms in a timely manner, and frequently indulge in self-medication prophylactically and therapeutically. Physiologic digestive processes, such as gut emptying, are enhanced [1] and there is a reduced incidence of liver disease [2], cholelithiasis [3], colon cancer [2], and constipation [4, 5]. Conversely, frequent, high-intensity exercise causes undesirable symptoms such as heartburn, chest pain, bloating, belching, nausea, vomiting, abdominal cramps, frequent urge to defecate, diarrhea, and constipation. Mucosal injury increases gut mucosal permeability, enhances occult blood loss, and induces translocation of protective bacterial flora and generation of endotoxins that can induce diarrhea [8, 14]. The excitement of competition elevates circulating catecholamines that are known to suppress thirst [21, 22]. Furthermore, athletes are frequently averse to the unpleasant sensation of a full stomach during competition. Therefore, it is not uncommon to delay hydration during competition, which in turn may expedite fluid and electrolyte imbalance. Dysphagia, a common swallowing disorder in the athletic population, is most commonly caused by acid reflux. However, it is important to recognize and expeditiously treat other potentially serious yet rarer causes of dysphagia. A careful history is crucial to diagnosis and can determine the cause of dysphagia in 80% of cases [27]. Although athletes may present with a spectrum of complaints, a few pivotal elements of a detailed history allow anatomic classification of dysphagia into two subclasses: oropharyngeal or esophageal. Second, does the difficulty swallowing occur soon after the initiation of deglutition or is it de layed Finally, is dysphagia painful or painless, and if painful, does the pain during deglutition localize to the neck or the chest Other characteristics may include either a change in dietary habits, dehydration, regurgitation, or unexplained weight loss. Frequent complaints include an ill-defined substernal pressure and burn ing, and in severe cases, frank chest pain. Other less common, yet important, causes of esophageal dysphagia in the athletic population include aortic aneurysm in athletes who have Marfanoid features; mechanical obstruction of the esophagus from strictures, webs, or malignancy; or motility disorders, such as achalasia or scleroderma. Although the precise mechanisms are not well defined, either the isolated effects or combination of several physiologic alterations contribute to acid reflux during exercise. Thus, exer cise has profound effects on acid reflux that are intensity-dependent [29]. Collings and colleagues [32] demonstrated that athletes involved in predominantly anaerobic sports, such as weight lifters, experience the most heartburn and reflux. In the same study, runners had mild symptoms and moderate reflux and cyclists had mild symp toms and mild reflux compared with weight lifters. However, there was a higher number and increased duration of reflux episodes in symptomatic individuals. Therefore, a future double-blind, randomized control study to compare the ef fects of acid suppression on exercise-induced gastroesophageal reflux should include asymptomatic and symptomatic athletes. For persistent symptoms, the addition of a motility-influencing agent such as dicyclomine may be effective. Athletes frequently eat shortly before bedtime, a deleterious habit that can enhance postprandial reflux. Dicyclomine, in turn, has been shown to decrease early postprandial reflux episodes [41]. Other less common causes in this population include diabetes, thyroid disease, and lactose intolerance. However, dyspeptic symptoms are vague, and athletes frequently delay assessment and treatment. Rehydration with carbohydrate drinks during exercise may lessen mucosal damage by enhancing blood flow to absorption sites in the gut, thereby reducing dyspepsia [45]. Failure of conservative therapy warrants testing and treatment for Helicobacter pylori infection, especially in athletes who are from underdeveloped countries. Although several theories have been proposed and a few studies have elucidated mechanisms, the literature is limited and the precise pathophysi ology remains largely undefined in the athletic population. Possible causative factors include enteric fluid and electrolyte imbalance, mesenteric ischemia contributing to increased mucosal permeability [14], mechanical trauma [47], and altered colonic motility. Some studies have shown that, by independent mechanisms, exercise can accelerate gut transit time of chyme and fecal residues [5] and intraluminal gas [26]. The transit of chyme and fecal residues is largely a passive process dependent on phasic motor activity and altered by exercise [49], whereas the transit of gas is influenced by visceral reflexes and involves con traction/relaxation of the abdominal wall [50, 51]. Furthermore, running has been shown to delay small bowel transit time [1, 8] and accelerate colonic transit time [8]. Other studies, however, have found that exercise does not alter small bowel or colonic motility [52], and transit time does not appear to be influenced by short bouts of high-intensity exercise and is independent of the mechanical bouncing of abdominal contents [53]. The diar rhea is defined as abnormally frequent, semisolid to watery bowel movements (>>3>> times per day) that can be acute (<<4<< weeks) or chronic (>>4>> weeks). In the absence of complications, such as fluid or electrolyte imbal ance, protracted vomiting, melena, hematochezia, or frank bleeding per rectum, supportive management with intravenous fluids, rest, and bismuth is suffi cient. Athletes who have viral gastroenteritis should temporarily be excluded from exposure to other teammates [54]. Antidiarrheal medications such as loperamide have adverse, depressive effects on the central nervous system, can affect heat dissipation and concentration [30], and should be used with caution. Although uncommonly encountered in athletes, infectious diarrhea must be ruled out if general sup portive measures are inadequate. A history of a recent camping trip or well water consumption could be suggestive of giardiasis. Athletes who have sickle cell trait or disease could have bloody diarrhea secondary to invasion with salmonella. Diarrhea associated with right lower quadrant abdominal pain that mimics appendicitis could be caused by Yersinia enterocolitica, and a history of bloody diarrhea following recent consumption of poorly cooked beef could suggest infection with hemorrhagic Escherichia coli (O157:H7). It is imperative to obtain stool cultures prior to instituting specific therapy because generic treat ment with ciprofloxacin can prolong salmonella infection and increase the risk for hemolytic uremic syndrome in individuals who have hemorrhagic E coli infection. Bloody diarrhea without an infectious cause, following the recent use of antibiotics, and associated with abdominal pain and fever is highly suggestive of Clostridium difficile colitis and should be aggressively treated with appropriate antibiotic therapy. A stool osmolar gap readily distinguishes secretory diarrhea from osmotic diarrhea and is an especially pivotal component of the laboratory investigation for chronic diarrhea in a female athlete at risk for an eating disorder. Proposed mechanisms include increased motor reactivity to various stimuli, in cluding stress, food, cholecystokinin, impaired transit of bowel gas [56, 57], visceral hypersensitivity, impaired reflex control that delays gas transit [58], autonomic dysfunction, and altered immune activation [59]. The clinical characteristics are diverse, yet the most common symptoms include cramping abdominal pain relieved by defecation, altered stool fre quency, altered stool form (mucus, watery, hard, or loose), altered stool passage (strain, urgency), a sense of incomplete evacuation, and abdominal distension especially following meals. Reassurance, stress reduction, consumption of small meals during the day, high-fiber diet, and avoidance of foods such as those containing lactose and candy that contains sorbitol are helpful first-line measures. Postexercise endoscopic colonic mu cosal biopsy samples have revealed congestive and hemorrhagic vascular le sions [70, 71]. As blood is shunted from the viscera to the working muscles during maximal exercise, splanchnic blood flow is decreased by as much as 80% [74].
| Comparative prices of Viagra Extra Dosage | ||
| # | Retailer | Average price |
| 1 | Brinker International | 381 |
| 2 | Belk | 656 |
| 3 | Verizon Wireless | 821 |
| 4 | SonyStyle | 487 |
| 5 | True Value | 453 |
Buy viagra extra dosage us
Range of symptoms the visual symptoms consist of diminished vision or blindness erectile dysfunction treatment san antonio buy viagra extra dosage on line amex, nonanatomic visual field defects, diplopia, and photophobia. The Pt has no signs of cerebral lesions extensive enough to cause cortical blindness and no history compatible with such lesions. The organically blind Pt moves cautiously and slowly, rarely banging into objects. Psychogenically blind persons may bang into objects, as if to prove they cannot see. The eyes of the psychogenically blind Pt may glance at a moving object that appears unexpectedly. The Pt may show optokinetic nystagmus (railroad nystagmus) when exposed to a rotating drum or moving stripes. Its presence thus establishes the integrity of the retinogeniculo-calcarine pathway and the efferent optomotor pathway to the brainstem from the occipital cortex, but the absence of nystagmus does not prove that the Pt has a lesion. The Ex may induce the Pt to have double vision by applying canthal compression (Fig. Acute retrobulbar neuritis can cause acute, complete blindness in an eye with a normal-appearing fundus before optic atrophy sets in. The diseased eye will show a diminished or absent direct pupillary light reflex, and the opposite pupil will fail to show a consensual reflex. In Anton syndrome, a bilateral, occipital lobe lesion causes bilateral cortical blindness, but the pupillary responses remain intact. Although obviously blind, the Pt confabulates vision, describing nonexistent scenes around him. During the diaschisis that may follow an acute, severe unilateral occipital lobe lesion, Anton syndrome may occur temporarily. Psychogenic visual field defects the typical psychogenic visual field defect consists of constriction of the diameter of the field, thereby producing tunnel or tubular vision, as if the person were looking through a tunnel. In a closely allied phenomenon, the spiral visual field, the size of the field diminishes on successive trials. In tunnel vision, the visual field remains the same diameter for near and far objects (Fig. In tunnel vision the field remains the same size for targets at different distances. The spectrum of psychogenic ophthalmologic manifestations include monocular diplopia. Caveat: A dislocated lens; a fold, detachment, or elevation of the retina; or a hole in the iris may cause organic monocular diplopia, but the ocular examination and ophthalmoscopy easily differentiate these conditions. Photophobia Pain in the eyes on exposure to light may occur with hysteria or with organic illnesses, for example, iritis. Careful slit-lamp examination and ophthalmologic investigation must rule out definable organic disease. Clinical and laboratory tests to establish the integrity of the auditory pathway the psychogenically deaf Pt may turn when addressed unexpectedly from the side or may show a startle response to sudden sound when awake or asleep. The presence of a response indicates an intact auditory pathway, but absence of a response does not establish organic deafness. The tuning-fork tests of Weber and Rinne described in Chapter 9 may produce bizarre results. Audiologists have several methods of manipulating sound to recognize hysterical deafness, which, combined with the brainstem evoked response test (Chapter 13) showing evoked potentials recorded over the auditory cortex, document the integrity of the auditory pathways. Caveat: acute viral illness, vascular occlusion, or pontine tegmental lesions can cause sudden deafness, with no other evidence of neurologic disease V. Range of disorders Patients with psychogenic somatosensory disorders may complain of anesthesia, paresthesia, hyperesthesia, or pain in the body or extremities. If the Pt loses one modality, it usually affects touch or pain, not vibration or position sense. Psychogenic sensory losses follow nonanatomic distributions and often have variable but very sharp borders from examination to examination. Chapter 10 explained how organic facial anesthesia from a V nerve lesion spares the angle of the mandible, which receives its sensory innervation from C2. In psychogenic anesthesia of an extremity, the loss usually includes the hand or foot and extends proximally to stop abruptly at a line transverse to the long axis of the limb, as if the extremity were amputated (seemingly a mental amputation). In psychogenic lower extremity anesthesia, the proximal border often falls at the waist or the gluteal fold posteriorly or the inguinal line anteriorly (Figs. As the anesthesia improves, the border moves distally along the limb, stopping at successive transverse levels until it disappears. The border follows the distribution of the entire Vth nerve or one of its three branches. In psychogenic paraplegia with a sensory level, the line circles the body horizontally; in organic paraplegia, the dermatomes slant downward in the abdomen; but this distinction is not absolute (Fig. The Pt not only loses all somatic sensation from one-half of the body but also may lose sight, hearing, taste, and smell on the affected side, an obvious anatomic impossibility. In psychogenic hemianesthesia, the sensory loss stops sharply at the midline and may run up the entire body and head as in the mental image of one-half of the body. The psychogenic Pt with hemisensory loss, for example, reports complete absence of vibratory sensation when a tuning fork, applied to the sternum or forehead, just reaches the midline. In fact, the vibration travels some distance through the bone, and its perception does not cut off sharply at the midline (Figs. Thus, the finding is not pathognomonic of psychogenic disease (Stone et al, 2002). Some differences in the borders of psychogenic and organic sensory losses in hemianesthesia. However, some patients with organic hemisensory loss also have an abrupt midline cutoff. Figure 14-9 shows the usual differences in the border zone of organic and psychogenic sensory losses. The site of the border between the anesthetic and the normal zone in psychogenic sensory disorders, although usually sharp, may change from time to time. Normal motor function: If the Pt has psychogenic anesthesia for all modalities, not anesthesia plus paralysis, the Pt may use the part completely normally, which is impossible without proprioception. This fact plus the preservation of stretch reflexes and absence of hypotonia, atrophy, and dystaxia prove that the Pt cannot have organic anesthesia. Rhythmic responses: In testing touch or pain responses, the Ex may elicit a rhythm of answering that inadvertently discloses the integrity of the sensation in the putatively anesthetic or analgesic area. Starting with areas of intact sensation, get the Pt to respond by saying yes when you apply the stimulus or no when you withhold it. Then, unexpectedly, out of rhythm, incorporate the anesthetic region in the testing. If the Pt says no each time just after the Ex unexpectedly touches the anesthetic zone, then at some level of consciousness, the Pt has perceived the stimulus. Pattern of exactly opposite responses: In responding to position sense testing, the psychogenic Pt may give exactly opposite answers, saying, for example, down each time for up. The fact that the Pt gives exactly the opposite response each time means that position sense has to be intact. Even with total absence of position sense, the Pt should guess the right answer about half of the time. Histrionic underreaction or exaggerated overreaction: Some Pts respond very slowly and deliberately to sensory tests.
Discount viagra extra dosage american express
Many Consider the impact of smoking and other substance abuse issues erectile dysfunction nyc buy generic viagra extra dosage line, may have tried and failed. A coordinated plan must be available for unhealthy diet and obesity, sedentary behavior and failure to maintain each patient who wishes to make improvements in lifestyle and must adequate exercise. Epidemics in obesity, diabetes and cardiovascular be developed with the individual needs of the particular patient with disease are directly related to smoking, poor diet, excess alcohol goals set and with sustained follow up. All have signi cant consequences approached as addictions and treated as intensely. All, to some extent, can promote better health if of health and disease prevention will result in a happier, healthier modi ed or can lead to severe deterioration and progression of illness. One will hopefully follow an improvement in lifestyle of the current estimate found that the calculated per capita medical spending for an population. Thompson in his research felt that a lifetime course of per and the overall economic impact of these diseases on the healthcare person obesity related medical costs were equal to those increases related system. World Health Organization data demonstrates obesity trends have been this comprehensive plan discusses ve key principles for obesity increasing globally over the last 3 decades. They are: United States have stabilized since 2003, they have more than doubled 1) Obesity is a chronic condition. It is approximated that two out of three adults in the Obesity is a chronic and often progressive condition not unlike diabetes U. In the United States 55 percent of adults diagnosed as diabetic are 2) Obesity management is about improving health and well-being, and obese and 85 percent are either overweight or obese (4). Diabetes as not simply reducing numbers on the scale de ned by the American Diabetes Association as the presence of any the success of obesity management should be measured in improvement one of the following three criteria A1C* 6. Pre diabetes is a risk factor for Type 2 3) Early intervention means addressing root causes and removing diabetes. As with any obesity, and setting unachievable targets simply sets up patients for journey, exercise needs to begin with getting started. Professional exercise prescriptions can be written for patients they can sustain while still enjoying their life and reaping the bene ts whose physical abilities are so signi cantly restricted by their obesity of improved health. If patients set weight 3) Advise (on obesity risks, discuss bene ts and options) loss as an immediate goal, many will stop exercising. Most patients will Speci c complain that free time for exercise is limited, so the best strategy is to Measurable have them set the alarm clock in the morning 15 minutes earlier. Exercise Achievable rst in the morning avoids con icts that arise later in the day. The addition of 5 minutes of exercise every 5) Assist (in addressing drivers and barriers, offer education and 2 weeks, will eventually lead to 40 minutes or more of exercise, where resources refer to provider, and arrange follow-up) goals of weight loss will begin to be ful lled. The electronic monitoring bracelets such as those offered by Nike, or FitBit allow for feedback in the opportunity to develop goals for obesity management must calorie output, achievement of set goals and tracking of each days effort also include information on diet and exercise. Once patients begin to make tness developed over a number of decades, a diet that appeals and is useful habit and the realization of improved health occurs, the reinforcement for one patient may not be accepted by another patient. Facilitating of wellness will help to move the patient toward increasing and more patient access to nutritional counseling will provide the ability for the sustained goals of health lifestyle choices. To review some of these associations consider regarding long term compliance, health bene ts with demonstrated cardiovascular disease such as stroke, myocardial infarction, peripheral reductions in stroke and heart attack and weight loss. Smoking related cancers provide a good foundation and structure for achievement and goal such as lung, laryngeal, throat, oral, esophageal, pancreatic, gastric, attainment. In this current age of technology many mobile apps allow renal, bladder, and acute myeloid leukemia. The list of associated patients to track calories and calculate meals with speci c calorie disease continues to grow, yet smoking remains one of the most goals in mind. Estimates for 2010 in the United States from Center for Disease Control and Despite the best efforts of providers and patients, some obese patients Prevention (C. The economics surgeons working alongside other obesity specialists to provide a of smoking related illness in 2005 were estimated to cost the United comprehensive solution for the appropriate patients. Exercise must States $193 billion($97 billion in lost production and $96 billion in be considered as vital to weight management and good health as health care expenditures) (11). Prevention through education and information will help smoking cessation than either medication or counseling alone. It is clear that improving the health of individuals is well worth the efforts toward cessation of tobacco use and dependence. Evidence-based approaches to diet, exercise, and smoking cessation should be utilized for best outcomes. The associated health risks of alcohol preventable illness can have dramatic effects on male morbidity and abuse include cancer (oral, pharynx, larynx, esophagus, liver, breast, mortality. Risks increase when alcohol abuse is associated male health issues, such as sedentary lifestyle, poor diet, smoking with tobacco abuse. Additionally, Cardiovascular disease (including and alcohol consumption, through a gender-speci c approach. The cardiomyopathy, atrial and ventricular brillation), Cirrhosis, Dementia, epidemics of male obesity, diabetes, and cardiovascular disease Depression, Seizures, Gout, Hypertension, Neuropathy, Pancreatitis, cannot be left unchecked any longer. Department of Health and Human Services, Public Health Service, Agency for Healthcare Research and Quality, 2008 [accessed 2013 June 5]. Clinical Professor of Urology, Department of Urology, University of Washington School of Medicine. El resultado de esto es que los hombres viven menos y Lo mismo se puede aplicar para las consecuencias del sindrome meta de forma menos sana, lo que impacta a las familias, comu bolico, apnea del sueno, diabetes, colesterol y lipidos elevados. La mayoria de las causas subyacentes estan relacionadas con estilos de vida evitables Esto no es para decir que los medicos sean los propiciadores del ex y modi cables elegidos por los hombres. Las epidemias ceso, sin embargo la responsabilidad hacia la identi cacion de los causadas por obesidad y diabetes estan directamente rela riesgos de estilo de vida descansa sobre los hombros de medicos y cionadas con el tabaquismo, mala alimentacion, exceso de proveedores no medicos. Se debe educar al paciente sobre las conse consumo de alcohol, y estilos de vida sedentarios. Si los me cuencias del estilo de vida en la salud por un lado y la importancia de dicos y autoridades responsables desean cambiar realmente una intervencion apropiada ante cualquier solucion medicamentosa, el mal estado de salud de los hombres, deben concentrarse por otro. La intervencion respecto a la correccion de estos estilos de en las enfermedades evitables que son resultado de estilos vida es en la mayoria de los casos mas intensa, tanto para los pa de vida y comportamientos. Hay que considerar el impacto del tabaquismo y otros con jacion de metas y con un seguimiento sostenido. Los excesos en temas de abuso de sustancias, dieta poco sana y obesidad, sedenta los estilos de vida deben considerarse como adicciones y ser tratados rismo y falta de ejercicios. La nalidad ultima de la salud y prevencion de enferme el desarrollo de las enfermedades. Todos estos aspectos, hasta cierto dades tendra como resultado un paciente mas feliz y mas sano que se punto, pueden promover una mejor salud si se modi can, o por el vera aliviado al consumir menos medicamentos. Asimismo, conservar contrario, pueden llevar a un severo deterioro y avance de la enfer valiosos dolares en salud y recursos dentro del sistema de atencion medad. Pueden calcularse como costos directos (aquellos resul tantes de los servicios de salud de pacientes externos y de pacientes Para apreciar mejor el impacto de estilos de vida saludables y no sa hospitalizados cirugia, laboratorios, imagenologia, medicamentos), y ludables, revisemos enfermedades asociadas, oportunidades para in costos indirectos de nidos como recursos no percibidos como resul tervenir y el impacto economico general de estas enfermedades en el tado de una condicion de salud (perdida de trabajo (5), costos por sistema de salud. Aunque las tasas de obesidad ciones relacionadas con la obesidad, es relativamente sencilla cuando en los Estados Unidos se han estabilizado desde 2003, se han mas se la compara con desarrollar un plan para tratar a un paciente obeso. Se pronostica que si esta tendencia continua en los Estados Unidos, la mitad de los hombres y mujeres seran obesos (3). Este exhaustivo plan plantea cinco principios claves para el manejo de la obesidad. Estos son: La enfermedad mas reconocible asociada con peso excesivo es la 1) La obesidad es una condicion cronica diabetes.
Cost of viagra extra dosage
Also includes ability to find and interpret relevant medical and scientific literature covering patient care generated problems erectile dysfunction yeast infection order viagra extra dosage 200mg amex, learning from clinical errors and quality improvement paradigms (as appropriate). Difficulties frequently include limited ability to find appropriate resources of information, interpretation of clinical or other relevant science to the understanding of the patient condition and lack of interest or speculation concerning the best way to approach a patient care problem. System Based Learning: this is about understanding the system and milieu in which health care takes place and its impact on decision making and advocacy for patients. The roles of different members and professions in health care teams, limitations of medical student and other relevant team members are implicit in system-based practice and learning. A development of understanding concerning the structure of the health care system, reimbursement system and utilization and review functions are important for doctors in training to develop the skill to understand how to navigate a patient to receive maximal benefit. Difficulties in this competency include a lack of knowledge (or interest) in the other professions that share responsibility in patient care and the effective interface with them, a poorly developed ability to understand how to get services and mobilize resources for patients they are following. Important Questions: Is the presence of the learner preventing you from doing what must be done Transfer Student Adapted from: Mountain Area Health Education Center Office of Regional Primary Care Education, North Carolina. Successful medical students learn a great deal from the patients they see, and clinical rotations in medical school are their most intensive opportunity to do this learning. Interviewing, observing, examining and listening to patients, medical students learn about how sickness and health present in health care settings, how patients and their families live and cope with illness and adversity and what kinds of internal and external resources help to do so. Hearing the stories of patients and their families, students form an understanding of how professionals and the medical system have helped or failed them (at least from their perspective) and thus what kind of doctor they want to become and how they wish to develop as a resource for patients and the community. Something to consider is that a lukewarm or negative letter is more damaging to the applicant than a non-acceptance of the task. If you cannot write a positive letter, let the learner know, give her/him the option of asking a different person. Discuss whether the student waives the right to see it, and whether you will copy them on it. Paragraph #2: this should explain the nature of your relationship and involvement with the student. What rotation the student worked with you in and how often the student was with you. Address professionalism, communication skills and interrelations with other members of the team, medical knowledge and clinical judgement. Paragraph #5: this is the summary and concluding statement and strength of the recommendation. Conclusion: Providing a Letter of Recommendation to a student is a tremendous and vital service we do for them, and it is required for their residency selection process. Think of the letter as not only a recommendation but a characterization of the student, focusing on their unique attributes rather than just placing them on an achievement scale, something accomplished by other components of their transcript and application. Page | 68 Faculty Development Part Three: Mentoring and Modeling How Doctors Think: Clinical Reasoning Skills One emphasis drawn from looking at the past and future development of the physician role in the health care team is on the distinguishing feature of physician training clinical reasoning. While all health care team roles use algorithmic and protocol driven practice, it is pre-eminently the role of the physician to solve problems that are unique to the patient or illness and to identify where algorithms or guidelines may not apply or function well. Effective clinical reasoning requires a higher level of development of medical knowledge than just the recognition of facts or even citing of new findings in clinical practice it requires familiarity with the inductive reasoning applied to patient care and ability to critically analyze research that informs us about the significance of variations of presentations, application of treatment options, evaluation of patient progress and unexpected findings in diagnosis and monitoring of patients. But the third year, when students develop critical habit patterns of approaching patient care thinking and practice, is a critical developmental step and the expectation they develop clinical reasoning skills needs to be reinforced and modeled. Doctors also use pattern recognition, generation of differential diagnosis, formulating exclusions, and develop skills in researching relevant sources of information pertinent to patient care. How to Model and Assess Professionalism There is almost universal agreement that professionalism is a critical competency in the development of physicians, but the focus and understanding of the most important aspects of professionalism varies with the background and philosophy of the beholder. Given the diversity of opinion on the definition and key aspects of professionalism, it is not surprising that assessment of this competency is more challenging than the others, and consensus on good tools has lagged behind other aspects of competency based medical education. Students learn by what we do, who we are or what we talk about, and to a lesser degree from what we teach. Most of us consider our own professionalism to be a lifelong work in progress and it may intimidate even the most highly professional of us to be reminded about the importance of modeling. Sometimes it might involve sharing our dilemmas and challenges as well as our aspirations, how we negotiate emotional and logistical conflicts we face in practice and patient care decisions as well as the principles we aspire to follow. Modeling, of course, also reflects our work ethic, how we follow schedules, talk to patients, staff and other professionals, how we dress etc. In addition to our modeling, as teachers, we can emphasize important expectations we have of students and give them feedback positively and negatively about how they are doing in this regard. Career Mentoring for Students Students overtly and covertly seek mentoring from physicians they work with on their career directions and options, and how best to achieve them. To some extent, this can be a daunting task, given the continuously changing developments and options, but your advice to them is likely to be valuable notwithstanding. During the 7-hour exam day, the students perform 12 standardized patient encounters. Callbacks is a required component of the Osteopathic Clinical Integration & Callbacks course and successfully completing all the components is needed for graduation. Students that perform below 70% in their encounter or are red flagged will be re-evaluated and eventually remediated. How preceptors could help Preceptors should observe the students perform H&Ps at least once or twice during the rotation. Observing the students at the beginning of the rotation and giving them timely feedback has the advantage of allowing them Page | 70 to correct mistakes and improve their skills by the end of the rotation. The preceptors can be documenting the encounter in the electronic health record while observing the student, if that helps with timing in a busy practice. Entrustable Professional Activities are 14 skills, tasks or responsibilities that represent what a resident will be able to do without supervision from day one of the residency. It is essential that medical students develop competency in all these areas as a first step to reach entrustability by the time they graduate. The Clinical Performance Evaluation helps demonstrate if a particular student is on the right path or if an intervention is required. The Clinical Performance Evaluation Forms are available online, in New Innovations. Information about New Innovations and that evaluation is provided here as a guide for our clinical preceptors. We ask that preceptors allot a brief amount of time to meet with the students at the middle, and at the end of the rotation in order to apprise learners of their progress and performance.
Syndromes
- Side effects of ADHD medicine
- Washing of the skin (irrigation) -- perhaps every few hours for several days
- Do you also have pain in the chest, jaw, arm, or somewhere else?
- Melanoma
- Heat
- Fever
- Time it was swallowed
- Give your child a small sip of water with any drugs your doctor told you to give your child.
- Porphyria cutanea tarda
- Pain and change of color in the legs (due to decreased blood flow)
Order viagra extra dosage with visa
Tooth future task to accumulate evidence by cohort and other loss and intakes of nutrients and foods: a nationwide highly reliable studies to further disclose the associations survey of Japanese dentists erectile dysfunction after prostatectomy viagra extra dosage 150mg with visa. Yoshihara A, Watanabe R, Nishimuta M, Hanada N, nutritional improvement through collaboration with other Miyazaki H. J Dent the relationship between nutrient intake, dental status Res 2003; 82: 123-126. Implant-supported Mandibular anthropometric analysis of edentulous patients wearing Overdentures in Very Old Adults: A Randomized implant overdentures or conventional dentures. Relationship between nutritional change the eating patterns among completely edentulous status and tooth loss in an older population from Sri patients Nutritional status of the oral health related quality of life in edentulous patients. Impact of tooth replacement between oral health, nutrient intake and nutritional strategies on the nutritional status of partially-dentate status in a sample of Brazilian elderly people. Correlation between dental and nutritional improvement on the nutritional status and quality of life status in community-dwelling elderly Japanese. Persistent oral health problems Number of teeth and its association with central obesity associated with comorbidity and impaired diet quality in in older Southern Brazilians. J Nutr Health Aging 2006; 10: 495-499; discussion Gerodontology 2012; 29: e685-e692. Update on the biological characteristics of the antioxidant micronutrients: vitamin C, vitamin E, and the carotenoids. Dietary antioxidant flavonoids and risk of coronary heart disease: the Zutphen Elderly Study. Antioxidant vitamins and coronary heart disease risk: a pooled analysis of 9 cohorts. With regard to this subject, continued accumulation of evidence is required along with further discussion. They found that the use of a denture on the upper jaw communication, and 451 rest-related articles were extracted signifcantly contributed to the reduction in the subscales of from both databases. In total, nine articles were extracted with regard to rest Six articles were extracted as reports on patients with (including the concepts of stress reduction, relaxation, and lifestyle-related diseases. The former study Studies in Japan, Thailand, and Turkey showed the was conducted on 70, 363 diabetic patients aged 65 years associations between oral health and communication. From the comparison the latter study was a case-control study conducted, on a between the baseline and change in the score after the group of 102 diabetic patients and a sex and age-matched intervention, a significant increase in the score of the control group of 102 residents in the same area in Sweden. In a study 24 targeting 721 local elderly men living the latter group conducted a cross-sectional study using in the U. Most of these research studies used the profile 20-49 years and 50 years and older with overstress both type scales that measure health multidimensionally and showed significantly lower oral health promotion scores whose reliability and adequacy had been psychometrically (which mean higher risks of having oral health problems) validated. It sleepiness and oral health, targeting 173 persons with an is also considered necessary to further accumulate evidence. Persons having All of 14 articles reviewed here were published in and frequent problems with their dentures tended to show more after 1997. Considering that four of them were published daytime sleepiness than those not having such problems within the last two years, increase in the number of reports (P=0. Association between oral health and rest/ Using the baseline data of a cohort study, Fukai et al. The number of sleep disorder) and oral conditions, targeting 5, 584 local articles available is small maybe because the topic is on residents in Japan aged 40 years and older. An intervention study also suggested [Discussion] that betterment of oral conditions can contribute to 1. Associations between oral health and health-related improvement in communication functions (expression). Although hours30 with mortality risk have already been reported, it is most of the articles we reviewed were about cross-sectional considered worthwhile in view of public health to clarify the studies based on which the causal associations could not associations of these factors with oral health. We believe that be identifed, it is interesting that these studies suggest the it is important to further accumulated evidence. Further, stress and sleep states, which are related Dental status, quality of life, and mortality in an older to communication and rest, were also associated with oral community population: a multivariate approach. An evaluation of self [References] reported oral health and health-related quality of life. The related quality of life in type 2 diabetic patients and non Sickness Impact Profle: development and fnal revision diabetic controls. Int J Ment Health 1994; 23: oral health and general health and quality of life in older 24-56. Oral and quality of life in long-term head and neck cancer status and its association with general quality of life in survivors. Naito M, Kato T, Fujii W, Ozeki M, Yokoyama M, Dent Oral Epidemiol 2009; 37: 231-240. The on the quality of life and activities of daily living in association between clinical oral health and general institutionalized elderly in Japan. Arch Gerontol Geriatr quality of life: a population-based study of individuals 2010; 50: 65-68. Dental status and satisfaction with oral function in a sample of community-dwelling elderly people in Japan. Self-perceived oral health status, psychological well-being, and life satisfaction in an older adult population. The combined association of psychological distress and socioeconomic status with all-cause mortality: a national cohort study. Kakizaki M, Kuriyama S, Nakaya N, Sone T, Nagai M, Sugawara Y, Hozawa A, Fukudo S, Tsuji I. Long sleep duration and cause-specific mortality according to physical function and self-rated health: the Ohsaki Cohort Study. The first item of the Basic their behavior even when education is provided many times Matters Related to the Promotion of Dental and Oral and those who do not visit clinics for dental examinations in Health stipulated under the Act concerning the Promotion the frst place. However, such education does not reach determines the health and behavior of people. We provide patients who do not come to clinics for guidance in the frst an overview of systematic reviews and meta-analyses of place. There are also patients who do not mend or improve studies related to oral health inequalities and their social their behavior although they receive education repeatedly determinants. We furthermore examine evidence of such and have sufficient knowledge, just as some doctors and inequality in Japan. Results confirmed that there is indeed dentists cannot stop people from smoking or make people health inequality, with persons with higher incomes and decrease excess weight. However, many of these people, school educational levels having better oral health and who do not come to clinics for guidance or cannot mend observing better oral-health-related behaviors. Studies their behavior, rush to dental clinics once they are affected in Japan, where dental treatment is covered under the by dental diseases, which is quite a familiar situation. This notion has been introduced is diffcult to take preventive measures for patients who do into government policies, as well as the subject of research not change their behavior readily even when education is and studies, in various countries of the world, including provided many times or for those who do not visit clinics Japan.
Purchase viagra extra dosage from india
Chronic elevation of serum uric acid is associated with progression of atherosclerosis erectile dysfunction usmle viagra extra dosage 130 mg lowest price. Chronic gout is treated with allopurinol or an uricosuric agent to reduce the amount of uric acid in the system. These medications are used in the long term to reduce the amount of painful flares that occur. A degenerative joint disease caused by the wear and tear of the articular cartilage. As the protective joint cartilage is worn away, the underlying bone becomes ex posed, causing the exposed bones to rub. Degenerative changes within the bone tissue produce small areas of re-growth, causing jagged joint spaces and bone spurs. The major weight-bearing joints are more affected in overweight patients due to the excess wear and tear on the joints, especially affecting hips and knees. Initially patients respond well to rest periods and over-the-counter medications for pain control. As joints become more damaged over time, a joint replacement may be necessary to correct pain and to improve quality of life and mobility. There is no underlying inflammatory disorder, so the medications can be used on an as-needed basis. Many of the patients are older and will be on other medications, so it is important that you check for medication interactions. In an adult, it is most commonly due to direct contamination of the site during trauma, such as an open fracture. Bacteria that cause infections elsewhere in the body may also enter the bloodstream and become deposited into the bone, starting a secondary infection site there. Some of the patients have been treated with antibiotics previously for the initial infection. Acute infection is associated with inflammatory changes in the bone and may lead to necrosis. This risk is greater in patients with a compromised immune system or poor blood supply to the area (such as diabetics). Typically, patients need antibiotics for several weeks to properly treat the infection. This is a decrease in bone density, making bones more brittle and increasing the risk of fracture. The body continuously replaces older bone with new bone through a balance between the osteoblastic and osteoclastic activity. When bone-building activity does not keep up with bone-resorption activity, the structural integrity of the bone is compromised. Increased age, lack of physical activity, poor nutrition, having a small frame, being Caucasian, Asian, or female all increase the risk of osteoporosis. The most common fracture sites in patients with osteoporosis are hip, vertebrae, pelvis, and distal radius. There is increased morbidity and mortality in patients who sus tain a hip fracture. The cost of healthcare for these patients is significant, and includes the immediate care of the fracture as well as the necessary rehabilitation. Calcium supplementation may be necessary for patients who are not getting the recommended daily requirement of calcium in the diet. If there is insufficient dietary intake, the body will remove the calcium from the bone, further weakening the structural integrity. Once osteoporosis occurs, proper medical management is important to prevent fractures and increase bone density. Crucial Diagnostic Tests X-ray Body part to be imaged needs to be positioned properly to see underlying bone structure, identify fractures, and detect foreign bodies. The patient may need to lie, sit, or stand, depending on the body part to be imaged. Typically, two different views are taken of the same body part to allow better diagnostics. This may be done to better assess the possi bility of bone chips or torn ligaments within the joint space. Biopsy A tissue sample is taken from a body part (muscle or bone) to determine disease state of tissue. The sample may be taken through closed (needle) biopsy or open (incisional) biopsy. It is done to determine the presence of infection, cancer, muscular atrophy or inflammation, or presence of mitochondrial disorders. Bone Scan this is a peripheral intravenous injection of bone-seeking radiopharmaceutical fol lowed by 2 to 3-hour delayed imaging. It is done to diagnose osteomyelitis, bone tumors, metastatic disease, fractures, and unexplained skeletal pain. The patient may be asked to move the area to allow for measurement during minimal and maximal contraction of the muscle. Certain medications may need to be stopped prior to testing: muscle relaxants, stim ulants, caffeine. The test is done to detect neuromuscular, peripheral nerve disorders, or lower motor neuron disorders, and may be done in conjunction with nerve conduction studies. As the radio waves bounce off the tissues in the body, different signals are sent based on the density of the tissues. Prior to the test, ask the patient about possible metallic objects (surgical clips, implants), pacemakers or implanted infusion pumps (may cause dysfunction of devices), or pregnancy. Myelography this is an injection of contrast medium into the subarachnoid space of the spine to allow for better visualization of the vertebral column, intervertebral discs, and spinal nerves. Posttesting, the patient typically is sitting to keep the contrast medium low in the spinal column, away from the brain. This is done to determine the pres ence and location of mass, fluid, or surgical hardware. Patients who work in settings that require repetition of the same hand movements over a long period of time have an increased risk for which of the following disorders You are caring for a patient who has just had open carpal tunnel release sur gery. In obtaining the patient history for your patient with carpal tunnel syn drome, you would expect to note a history of: (a) pain and numbness or tingling sensation in the hand (over the palmar surface of the thumb, index finger, middle finger, and lateral aspect of the ring finger) that is worse at night. Initial treatment of the patient with a fracture should include: (a) surgical reduction of the fracture. The first priority of care of the patient with a new fracture includes assessing: (a) respiratory rate and effort, pulse. Patients with a history of osteoporosis have an increased risk for: (a) infection in the bone. Teaching patients about proper use of bisphosphonate medications for treatment of osteoporosis should include taking medication: (a) on a full stomach. In order to allow for proper healing, patients with osteomyelitis may need to have: (a) debridement and drainage of the area.

Generic 200mg viagra extra dosage free shipping
Compare photosynthe terconvert sufficiently quickly to be considered as a single chemical sis erectile dysfunction medication non prescription cheap viagra extra dosage 200 mg free shipping. In Escherichia the phenomenon is now exploited in sensitive enzyme assays and coli the che family of genes has been implicated in controlling cer labelling methods in nucleic-acid hybridization, etc. Essentially it states that the en chemotaxonomy the classification of organisms on the basis of the ergy-yielding reactions of the respiratory chain are coupled to the en nature, content, and/or the distribution of constituent chemical ergy-requiring reactions of phosphorylation through the creation of substances. An electrochemical gradient chemotherapy the treatment of disease, especially infections and of H+ ions, and a voltage gradient, is established across the mito neoplasms, with chemical agents (chemotherapeutic agents) that act chondrial inner membrane during electron flow through the respi specifically on infective organisms or tumours. Chemotrophs may be sub lar mechanism is believed to drive oxidative phosphorylation in the divided into (1) chemoautotrophs (or chemolithotrophs), i. Compare chemotropism the orientation of cells or organisms in response to physisorption. See mosaic, transgenic, chimeric mol where S is the substrate concentration and Km the Michaelis con ecule. The effect is analogous to the creation chimyl alcohol glycerol 1-hexadecyl ether, (+)-3-(hexadecyloxy) of a sonic boom that occurs when an object exceeds the speed of 1, 2-propanediol; a hydrolysis product of ether lipids. See also chicle a mixture of cis and trans-1, 4-polyprenoids obtained from prochiral. Chico an insulin receptor substrate-like protein in Drosophilia that links the insulin receptor to phosphatidylinositol 3-kinase and then chiral recognition the differentiation of the enantiomers of a com protein kinase B and protein synthesis. This can be achieved by living organisms, chiral molecules, sponding gene results in fruit flies less than half the normal size. Chimeras can occur as a result chiroptical describing any of the phenomena that depend on the of mutation, abnormal distribution of chromosomes, grafting, or ability of chiral and other intrinsically asymmetric molecules to ro genetic manipulation. For example, a chimera can be created by tate the plane of polarized light, known collectively as optical activ mixing the cells from embryos of two different animal species at the ity. It is found in annelid cuticle, arthropod ex use in radioimmunoassay or other in vitro techniques. In fungi, chitin represents quantities of many proteins are labelled efficiently at or near pH 7; the microfibrillar component of the cell wall. See also chitobiose, however, some proteins may suffer an unacceptable degree of ox idative damage. An enzyme that catalyses the hydrolysis of the 1, 4-b-linkages of N-acetyl-D-glu S Na+ cosamine polymers of chitin. This reaction forms the basis for ac chitosan the cationic polymeric carbohydrate obtained by the quired chloramphenicol resistance in certain bacterial strains. It is the proto 116 chloride chlorophyll typical benzodiazepine, used therapeutically as the hydrochloride. These are structurally unrelated to dichloro-1, 3-cyclopentanedione (caldariomycin). They are found in a wide range of organisms, from phyll) pigments, found in plants and photosynthetic bacteria, that bacteria and yeasts to plants and animals. Their functions in higher function in photosynthesis by absorbing light energy mainly in the animals are thought to include regulation of cell volume, control of red and violet-blue parts of the spectrum. The main chlorophylls of land plants are chlorophylls a and b, and chloride shift or Hamburger shift the phenomenon whereby, be some algae contain chlorophylls c. Chlorophylls a and b are dihy cause of the isohydric shift, there is a higher concentration of hydro droporphyrins, having no double bond at position 3 of ring B, while gencarbonate ions in the erythrocytes in blood leaving the tissues chlorophylls c are porphyrins. Photosynthetic bacteria contain var (venous blood) than in arterial blood, and hence the hydrogencar ious bacteriochlorophylls. It is formed by the light-catalysed reduction of protochloro phyllide attached to a protein, protochlorophyllide holochrome. It 118 cholecystokinin receptor cholestyramine resin is identical with pancreozymin. Their common C-terminal tetrapeptide amide se and the precursor of many steroids, including bile acids and steroid quence is identical to that in which the functional activity of gastrin hormones. Binding of the toxin to its receptor cholesterol acyltransferase see sterol O-acyltransferase. This is the first step in the biosynthesis of 2 H3C H bile acids from cholesterol and is rate-limiting. H3C H cholesterol side-chain cleavage enzyme see cholesterol monooxygenase (side-chain cleaving). M1 and M3 activate phosphoinositide-specific phos cholic acid 3a, 7a, 12a-trihydroxy-5b-cholan-24-oic acid; a meta pholipase C; M2 and M4 are negatively coupled to adenylate cy bolic derivative of cholesterol, produced in the liver and secreted as clase; M2 also increases potassium channel conductance through a bile acid. It is used as a detergent, as the sodium salt; aggregation the action of G-proteins. Torpedo elec tric organ and embryonic muscle pentamers have a2bcd, adult H C H mammalian muscle a2bde, and mammalian neurons a2b3 stoi 3 chiometry; each subunit contains four transmembrane segments. It is in chondroitinase see N-acetylgalactosamine-4-sulfatase, N-acetylgalac strumental in the synthesis of the neurotransmitter acetylcholine. They often are polydisperse and often dif choline phosphate with release of pyrophosphate. The chains of re cholinergic describing nerve fibres that, when activated, release peating disaccharide are covalently linked to the side chains of ser acetylcholine or an acetylcholine-like substance from their endings. It is found in most tissues including matrix of avascular zones of epiphyseal cartilage. It is not produced in chon in infancy, pregnancy, liver disease, thyroid deficiency, malnutri drosarcoma. They may suffer from procaine toxicity, prolonged suc ranuronosyl-D-galactopyranose; condensed form: GlcpA(b1 cinylcholine apnea, and cocaine toxicity. It is also a good chromaffin tissue a tissue made up of modified neural cells (chro marker for choriocarcinoma. It is a heterodimer of an a chain (iden maffin cells) that synthesize, store, and secrete catecholamines. Tumours of this tissue, usually in the adrenal cental hormone similar in action to somatotropin and prolactin. It medulla, cause a syndrome of intermittent hypertension and exces shows 85% homology with the former and 13% with the latter. The gene at 17q22-q24 is near chromatid one of the two daughter strands of a duplicated chromo those for somatotropin and prolactin. Chromatin is made up of repeating units, each unit motrophin an alternative name for choriomammotropin. It disappears at about and tyrosine; the other branch, the anthranilate pathway, leads to the time of vitellogenesis and its contents become dispersed in the tryptophan. Chromatin, partially digested with branch of the shikimate pathway that leads to synthesis of phenylala micrococcal nuclease, is electrophoretically separated in the first di nine. Transcrip chromodomain a protein domain that recognizes the C-terminal tional silencers are required for initiation of chromatin silencing, a tails of nucleosomal histones that contain specifically methylated state that is correlated with decreased histone acetylation. Both pro chromatography any technique, analytical or preparative, for sep teins are acidic (pI 4. A number of artificial radioactive nuclides are loaded with carotenoids are called carotenoid bodies. Chylomicrons are formed in the mucosa of the small tion to the two daughter cells. They then enter the lymphatic capillaries (lacteals) chromosome band any of numerous transverse bands along a of the intestinal villi, and thence the bloodstream. Hyperchylomicronemia results from deficiency of lipopro to regional base composition. An enzyme that catalyses preferential cleav then used in turn as probes to identify clones carrying sequences ad age of the bonds: Phe-|-Xaa > Tyr-|-Xaa > Trp-|-Xaa > Leu-|-Xaa. It is produced from a precursor in the chronic external ophthalmoplegia an alternative name for mucosa of the fourth stomach of calves. It preferentially cleaves at the car 123 chymotrypsinogen circular permutation bonyl end of Leu, Tyr, Phe, Met, Trp, Gln, and Asn residues.
Purchase viagra extra dosage 150 mg
Growth velocity resumes rapidly when the dose is reduced to <40 mg/kg day impotence prostate buy viagra extra dosage now, while it does not respond to hormonal treatment. It is therefore recommended that doses do not exceed 40 mg/kg until growth has ceased. Regular monitoring of growth is essential in all children (see Chapter 8 for details on endocrine complications). Rickets-like bony lesions and genu valgum may be seen in association with metaphyseal changes, particularly in the vertebrae, giving a disproportionately short trunk. Radiographic features include vertebral demineralization and flatness of vertebral bodies. Interstitial pneumonitis have been reported at very high doses of 10 mg/ kg/h or more. The % solution infused should not exceed 10% or the risk of skin reactions increase. Infection should be considered in any patient with a febrile illness, especially when associated with abdominal pain, diarrhoea or joint pains, and should be treated as a medical emergency. The most common were chromaturia (red in colour due to urine in iron), nausea (13%), vomiting, abdominal pain (10%), elevations in alanine aminotransferase (8%), arthralgia (10%) and neutropenia (7 %). Other unwanted effects >1% were back pain (2%), arthropathy (1%), agranulocytosis (1. The drug is licensed up to 100 mg/kg/day but insufficient numbers have been reported to know whether the incidence of the most serious complication, namely agranulocytosis, is increased at these higher doses or indeed decreased at lower doses. Dose related effects on bone marrow hypoplasia and neutropenia has been seen in animal studies. Reported timing of onset of agranulocytosis is variable, from a few months to nine years. The condition may occur with thrombocytopenia, but isolated thrombocytopenia has also been occasionally reported, particularly in patients of Asian origin with probable hypersplenism. Neutropenia is more common in patients with intact spleens and commonly occurs in the first year of therapy. However, it can be difficult in clinical practice to distinguish whether a low neutrophil count is part of a pattern of underlying neutropenia, or the first sign of agranulocytosis developing, which can be fatal. In 46 cases of agranulocytosis reported in Europe there were nine related deaths (Swedish Orphan 2006). A proportion of patients have to stop treatment for these reasons, which varies between studies. A liquid preparation is available which may be more palatable in children 1-10 years of age (ElAlfy 2010). An observational report of fibrosis after treatment of three or more years (Olivieri 1998) has not been supported by other reports (Wanless 2002, Hoffbrand, Tondury 1998). It is not yet clear whether these differences reflect environmental or genetic differences, or differences in iron overload between populations at the start of treatment. Symptoms range from mild non-progressive arthropathy, typically in the knees and controllable with non-steroidal anti-inflammatory drugs to (more rarely) severe erosive arthropathy that may progress even after treatment is stopped. Cases involving other joints, such as wrists, ankles and elbows and avascular necrosis of the hips have also been described. Neurological complications are very rare in thalassaemia treatment and have been typically associated with unintentional overdosing (>230 mg/kg/day). Reports of rare neurological effects have included stroke, cognitive effects, nystagmus, walking disorders, ataxia, dystonia and impaired psychomotor skills. A regular eye examination including retinal evaluation at least once yearly is therefore advisable. Zinc deficiency is difficult to measure in plasma samples, and needs to be taken during fasting, in the absence of chelator in the blood. The frequency of adverse effects appears somewhat higher at doses of 25 to < 35 mg/k g/day (n = 136; 39. Gastrointestinal, skin and renal effects can all be affected by dosing, although the exact relationship to body iron load has not been determined. Many clinicians therefore operate a dose reduction policy; giving very low doses (5 mg-10 mg/kg) to those patients who continue to be transfused. Some effects are notable by their absence, such as effects on growth, bone and arthropathy. Reported serum creatinine increases did not increase in low versus high-iron cohort patients. These symptoms rarely require dose adjustment or discontinuation, and decrease year on year over 5 years of follow up (Cappellini 2011). The role of co-administration of acidophilus or lactobacillus probiotic yoghurt to aid lactose has not been systematically studied. Special attention should be taken in patients taking concomitant medications that can increase the possibility of gastric ulceration. Skin rash is more common in Asian population (up to 18%), often mild in severity and rarely developing into severe drug-hypersensitivity (Viprakasit 2011). A minority of patients require permanent discontinuation of therapy, and mild rashes often resolve without dose modification, and became very rare after year 1 of treatment (Cappellini 2011). For moderate to severe rashes, treatment should be stopped and later restarted at a very low dose (<5 mg/kg), slowly increasing to therapeutic doses. In a randomized study, dose reduction of 33-50% was planned if at least two consecutive increases in serum creatinine were >33% above baseline. As the creatinine spontaneously normalised in a number of cases, dose reductions were instituted in only 13%. In about 25% of those cases, the creatinine then returned to baseline, while in the rest it remained stable or fluctuated between baseline and the maximum increase observed prior to dose reduction. At 5 years of follow up, no evidence of progressive renal dysfunction had been reported where the above doses and modifications were used (Cappellini 2011). It is recommended that urine is monitored regularly for protein, and this can be conveniently performed at the time of visits for cross matching blood. Although proteinuria can fluctuate considerably, if there is a clear upward trend in the protein/creatinine ration above 1 mg/g, interruption or dose reduction should be considered. Current drug labelling recommends monthly urine testing for protein, which is helpful in establishing trends in proteinuria, as isolated estimates can be misleading. Symptoms of renal tubular acidosis can be non-specific but may include polyuria, polydipsia and dehydration. Investigations may show proteinuria, hypokalemia, hypophosphatemia, hyperchloremic metabolic acidosis with excessive loss of substances in the urine. Some patients, especially children, have intercurrent infections associated with Fanconi syndrome. By the end of the study, stability of Ishak fibrosis staging scores (change of 1, 0, or +1) or improvements (change of </=-2) were observed in 82. Possible audiometric effects were identified in early studies but this has not been reported systematically. One investigator has reported lens opacities in 3 out of 12 patients (Bloomfield 1978), which would approximate to 80-times the incidence observed in the large-scale trials, the reason for which is presently unclear (Ford 2008). However, at present it is recommended that thalassaemia patients who plan to conceive should avoid the use of iron chelation for at least 3 months before. Because these are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or to establish a causal relationship to drug exposure. Concentrations in excess of this may increase the risk of local reactions at the site of infusion. Some patients find that the skin over the deltoid or the lateral aspect of the thigh provides useful additional, alternative sites. Many patients are happy with butterfly needles of 25 gauge or smaller, which are inserted at an angle of about 45 degrees to the skin surface. Other patients prefer needles that are inserted vertically through the skin and are fixed with an adhesive tape attached to the needle (see Figure 4).
Purchase viagra extra dosage 150mg free shipping
Anterior lumbar interbody conventional approach for degenerative spondylolisthesis with fusion for lumbosacral junction in steep sacral slope erectile dysfunction pumps buy 130mg viagra extra dosage. Lumbar sifcation, and management of neuralgia afer posterior lumbar posterolateral fusion alone or with transpedicular instrumenta interbody fusion surgery in 226 patients. Degenerative lumbar spondylolisthesis-induced degenerative spondylolisthesis treated with posterior de radicular compression: nonfusion-related decompression in compression alone via a new surgical approach. Aortic fap valve instrumentation for treatment of spondylolisthesis and degen presenting as neurogenic claudication: a case report. Uninstrumented in son of surgical and conservative treatment for degenerative situ fusion for high-grade childhood and adolescent isthmic lumbar scoliosis. Degenerative spondy with spinal stenosis: a prospective long-term study comparing lolisthesis: lumbar stenosis and instability. Posterolateral spinal fusion: Correlative radiological, self-assessment and clinical analy a study of 123 cases with a long-term follow-up. L2 radicular compression caused by a fo lumbosacral fusion at a minimum 5-year follow-up. J Neuro spinous dynamic stabilization using the locker for lumbar canal surg Spine. The positive predic medically compromised elderly patients: technical case report. Fluoroscopically guided plication of one-level posterior lumbar interbody fusion with caudal epidural steroid injection for management of degenera prospace and facet fusion using local autograf. Acta Neurochir surgical options for degenerative conditions of the cervical and (Wien). Sciatica in degenerative spondylolisthesis of the spine: anterior lumbar interbody fusion followed by percutane lumbar spine. J nopelvic alignment afer interspinous sof stabilization with a Bone Joint Surg Br. Clinical efcacy of lumbar and lumbo displacement afer fusion in patients with idiopathic scoliosis: sacral fusion using the Boucher facet screw fxation technique. Vertebral osteolysis laminectomy for bilateral decompression of lumbar spinal afer posterior interbody lumbar fusion with recombinant hu stenosis: a prospective comparative study with conservatively man bone morphogenetic protein 2: a report of fve cases. Rehabilitation following tionship between alterations of the lumbar spine, visualized with surgery for lumbar spinal stenosis. Translaminar screw fxation in in subjects with lumbar spondylolysis and spondylolisthesis: lumbar spine pathology. Are lumbar spine reoperation rates falling with greater fusion with local bone graf plus bone extender compared with use of fusion surgery and new surgical technology. Reoperation rates following lumbar spine surgery and the Implications of spinopelvic alignment for the spine surgeon. Hospital and surgeon variation in complications and inal versus posterior lumbar interbody fusion: comparison of repeat surgery following incident lumbar fusion for common surgical morbidity. Spinal stenosis in totactic efect on a herniated disc at the level adjacent to the grade I degenerative lumbar spondylolisthesis: a comparative anterior lumbar interbody fusion: report of two cases. Nonsurgically managed sults of circumferential spine fusion in smokers, using autograf patients with degenerative spondylolisthesis: a 10 to 18-year and allograf. Symptomatic ganglion cyst of ligamentum favum as a Natural history of degenerative spondylolisthesis. Microsurgical anterior approaches to and predictive factors relating to prognosis, in a 5-year mini the lumbar spine for interbody fusion and total disc replace mum follow-up. Analysis of the relationship between facet joint angle of the soleus H-refex in lumbar spondylolisthesis: a possible orientation and lumbar spine canal diameter with respect to early sign of bilateral S1 root dysfunction. How to stabilize a single level stenosis with a total posterior arthroplasty prosthesis: implant lesion of degenerative lumbar spondylolisthesis. Clin Orthop description, surgical technique, and a prospective report on 29 Relat Res. The indications for outcomes afer lumbar fusion for degenerative spondylolisthesis interbody fusion cages in the treatment of spondylolisthesis: with large joint replacement surgery and population norms. Microdecompression and uninstrumented 5-year follow-up of anterior column structural allografs in the single-level fusion for spinal canal stenosis with degenerative thoracic and lumbar spine. In-hospital postopera this clinical guideline should not be construed as including all proper methods of care or excluding or other acceptable methods of care reason ably directed to obtaining the same results. Radiologic assessment of lum the treatment of spondylolisthesis, failed-back syndrome, and bar intervertebral instability and degenerative spondylolisthesis. Spinous process-splitting open fxation with bone grafing for symptomatic isthmic lumbar pedicle screw fusion provides favorable results in patients with spondylolysis. Teriparatide accelerates lumbar parison between rigid fusion and dynamic non-fusion stabiliza posterolateral fusion in women with postmenopausal osteopo tion. Okuda S, Oda T, Miyauchi A, Haku T, Yamamoto T, Iwasaki approach for bilateral decompression of lumbar degenerative M. J Spinal Disord son of the percutaneous screw placement precision of isocentric Tech. A radiographic implantation and conventional fuoroscopy method with mini assessment of the ability of the extreme lateral interbody fusion mally invasive surgery. J term follow-up data afer placement of the Graf stabilization South Orthop Assoc. Medicinal and injection thera lumbar spine using the minimal access non-traumatic insertion pies for mechanical neck disorders. Association of incipient disc degeneration operative costs and outcomes in patients with and without and instability in spondylolisthesis. Instability in lumbar spondylolisthesis: lumbar spinal stenosis involving a unilateral approach with mi a radiologic study of several concepts. Clinical outcomes of microen strumented lumbar arthrodesis in elderly patients: prospective doscopic decompressive laminotomy for degenerative lumbar study using cannulated cemented pedicle screw instrumenta spinal stenosis. Degenerative lumbar scoliosis: radiographic correla tion afer multi-level posterior dynamic stabilization with tion of lateral rotatory olisthesis with neural canal dimensions. A comparison of unilater plications associated with minimally invasive decompression for al laminectomy with bilateral decompression and fusion surgery lumbar spinal stenosis. Degenerative lumbar spon interbody fusion with reduction of spondylolisthesis: technique dylolisthesis. Multiple laminotomy mum 2-year follow-up result of degenerative spinal stenosis compared with total laminectomy. Part I: Etiology, pathogenesis, pathomorphology, and clini solid fusion on clinical outcomes afer minimally invasive trans cal features. The reliability of the Shuttle efectiveness of minimally invasive versus open transforaminal Walking Test, the Swiss Spinal Stenosis Questionnaire, the lumbar interbody fusion for degenerative spondylolisthesis Oxford Spinal Stenosis Score, and the Oswestry Disability Index associated low-back and leg pain over two years. Toward uniformity in evaluat provement in pain, disability, and health state associated with ing results of lumbar spine operations. A paradigm applied to cost-efectiveness: introduction of the concept of minimum posterior lumbar interbody fusions. Intraoperative multimodality monitoring versus Open Transforaminal Lumbar Interbody Fusion for in adult spinal deformity: analysis of a prospective series of Degenerative Spondylolisthesis: Comparative Efectiveness and one hundred two cases with independent evaluation. The efect of iliac crest undergoing lumbar laminectomy for degenerative spondylolis autograf on the outcome of fusion in the setting of degenera thesis. Transforaminal lumbar symptoms in patients with spinal stenosis and degenerative interbody fusion: technique, complications, and early results. Retrospective computed tomography scan minimal invasive posterior transforaminal lumbar interbody fu analysis of percutaneously inserted pedicle screws for posterior sion: a clinical and radiographic follow-up. Spinal Care in a outcomes afer posterior decompression and fusion in degenera Single-Payer System: The Canadian Example. Current Opin Or compared with conventional open fusion for lumbar spondylo thop. Surgery for lumbar spinal stenosis in lumbar spinal stenosis compared with total joint arthroplasty for old people. Posterior lumbar interbody fusion cral autogenous bone graf fusion in adult patients with degen versus circumferential fusion using the B-Twin expandable spi erative spondylolisthesis.