
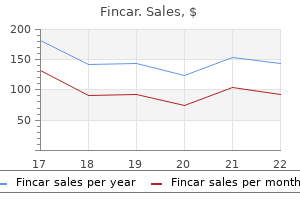
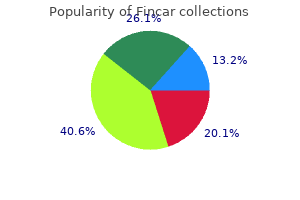
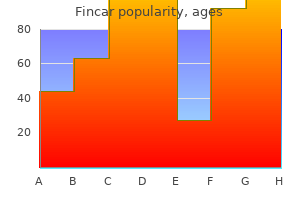
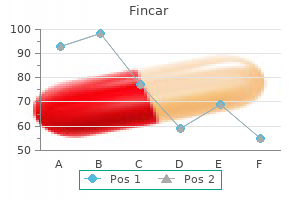
Fincar
Quality fincar 5 mg
A small subset of patients may experience radiating pain in addition to decreased range of motion and low back discomfort mens health june 2013 discount 5 mg fincar amex. For example, the pain intensity changes with increased physical activity, certain movements or postures and decreases with rest. However, night-time back pain may be present in the absence of serious specific spinal disorders. The precise location and originating point of back pain is often difficult for patients to describe. Several conditions may cause pinched or compressed nerves in the low back area putting pressure on the spinal cord that may cause tingling, muscle weakness and sudden loss or impairment of bowel and bladder function. Normally, the spinal cord is protected by the back bones (vertebrae) that form the spine, but certain injuries to and disorders of the spine may cause cord compression, affecting its normal function. The spinal cord may be compressed by bone, the collection of blood outside a blood vessel (hematomas), pus (abscesses), tumors (both noncancerous and cancerous), or a herniated/ruptured or malformed disc. These injuries and disorders may also compress the spinal nerve roots that pass through the spaces between the back bones or the bundle of nerves that extend downward from the spinal cord (cauda equina). The spinal cord may be compressed suddenly, causing symptoms in minutes or over a few hours or days, or slowly, causing symptoms that worsen over many weeks or months. Lumbar spine decompression is a broad definition of surgical procedures performed on the bones in the lower (lumbar) spine to relieve the pinched or compressed spinal cord and/or nerve(s). During a lumbar decompression surgery the surgeon removes portions of the intervertebral disc and/or adjacent bone and tissue in the lower spine to give the nerve root more space. Surgical procedures for spinal decompression include lumbar discectomy, foraminotomy, laminotomy, and lumbar laminectomy. Background Lumbar Discectomy (Diskectomy) Discectomy is a surgical procedure in which one or more intervertebral discs are removed. Extrusion of an intervertebral disc beyond the intervertebral space can compress the spinal nerves and result in pain, numbness, and weakness. Discectomy is intended to treat symptoms by relieving pressure on the affected nerve root(s). Discectomy can be performed by a variety of surgical approaches, with either open surgery or minimally invasive techniques. Page | 13 of 26 Disc Herniation Extrusion of an intervertebral disc beyond the intervertebral space can compress the spinal nerves and result in symptoms of pain, numbness, and weakness. The natural history of untreated disc herniations is not well-characterized, but most herniations 3 will decrease in size over time due to shrinking and/or regression of the disc. Clinical symptoms will also tend to improve over time in conjunction with shrinkage or regression of the herniation. Treatment Because most disc herniations improve over time, initial care is conservative, consisting of analgesics and a prescribed activity program tailored to patient considerations. Other potential nonsurgical interventions include opioid analgesics and chiropractic manipulation. Epidural steroid injections can also be used as a second-line intervention and are associated with short 4 term relief of symptoms. A small proportion of patients will have rapidly progressive signs and symptoms, thus putting them at risk for irreversible neurologic deficits. These patients are considered to be surgical emergencies, and expedient surgery is intended to prevent further neurologic deterioration and allow for nerve recovery. Other patients will not progress but will have the persistence of symptoms that require further intervention. It is estimated that up to 30% of patients with sciatica will continue to have pain for 5 more than 1 year. For these patients, there is a high degree of morbidity and functional disability associated with chronic back pain, and there is a tendency for recurrent pain despite treatment. Therefore, treatments that have more uniform efficacy for patients with a herniated disc and chronic back pain are needed. In particular, decreased chronic pain and decreased disability are the goals of treatment of chronic low back pain due to a herniated disc. Surgical Treatment Discectomy is a surgical procedure in which one or more intervertebral discs are removed. The primary indication for discectomy is herniation (extrusion) of an intervertebral disc. Discectomy is intended to treat symptoms by relieving pressure on the affected nerve(s). Page | 14 of 26 Lumbar Discectomy Lumbar discectomy can be performed by a variety of surgical approaches. The spinal muscles are dissected, and a portion of the lamina may be removed to allow access to the vertebral space. The extruded disc is removed either entirely or partially using direct visualization. Osteophytes that are protruding into the vertebral space can also be removed if deemed necessary. The main alternative to open discectomy is microdiscectomy, which has gained popularity. Microdiscectomy is a minimally invasive procedure that involves a smaller incision, visualization of the disc through a special camera, and removal of disc fragments using special instruments. Because less resection can be performed in a microdiscectomy, it is usually reserved for smaller herniations, in which a smaller amount of tissue needs to be removed. A few controlled trials comparing open discectomy with microdiscectomy have been published and reported that neither procedure is clearly superior to the other, but that microdiscectomy is associated with 6,7 more rapid recovery Systematic reviews and meta-analyses have also concluded that the 8-10 evidence does not support the superiority of 1 procedure over another. Adverse Events Complications of discectomy generally include bleeding, infections, and inadvertent nerve injuries. Dural puncture occurs in a small percentage of patients, leading to leakage of cerebrospinal fluid that can be accompanied by headaches and/or neck stiffness. In a small percentage of cases, worsening of neurologic symptoms can occur postsurgery. Lumbar Laminectomy Lumbar laminectomy is a surgical procedure in which a portion of the lumbar vertebra (the lamina) is removed to decompress the spinal cord. Removal of the lamina creates greater space for the spinal cord and the nerve roots, thus relieving compression on these structures. Lumbar laminectomy is typically performed to alleviate compression due to lumbar spinal stenosis or a space-occupying lesion. Associated Disorders the most common diagnosis treated with laminectomy is spinal stenosis. In spinal stenosis, the spinal canal (vertebral foramen) is narrowed, thus compressing the spinal cord. Other conditions that cause pressure on the spine and spinal nerve roots include those where a mass lesion is present (eg, tumor, abscess, other localized infection). Surgical Techniques Laminectomy is an inpatient procedure performed under general anesthesia. An incision is made in the back over the affected region, and the back muscles are dissected to expose the spinal cord. The lamina is then removed from the vertebral body, along with any inflamed or thickened ligaments that may be contributing to compression. Following resection, the muscles are reapproximated and the soft tissues sutured back into place. The extent of laminectomy varies, 16 but most commonly extends 2 levels above and below the site of maximal cord compression. It can be performed by minimally invasive techniques, which minimizes the extent of resection. Laminoplasty is a more limited procedure in which the lamina is cut but not removed, thus allowing expansion of the spinal cord. Foraminotomy and/or foramenectomy, which involve partial or complete removal of Page | 16 of 26 the facet joints, may be combined with laminectomy when the spinal nerve roots are compressed at the foramen. Spinal fusion is combined with laminectomy when instability of the spine is present preoperatively, or if the procedure is sufficiently extensive to expect postoperative spinal instability. Surgical Variations Hemilaminotomy and laminotomy, sometimes called laminoforaminotomy, are less invasive than laminectomy. These procedures focus on the interlaminar space, where most of the pathologic changes are concentrated, minimizing resection of the stabilizing posterior spine.
Diseases
- Narrow oral fissure short stature cone shaped epiphyses
- Nemaline myopathy
- Revesz syndrome
- Scleredema
- Hereditary sensory and autonomic neuropathy 3
- Chromosome 11, deletion 11p
Discount fincar 5mg amex
Therefore prostate 22 order 5 mg fincar free shipping, treatment involves learning to identify when your thoughts contain distortions or errors that contribute to your misery. Soon after it was adopted for treating depres sion, cognitive therapy was applied quite successfully to anxiety disorders and, ultimately, to a dizzying array of emotional problems, including eating disorders, oppositional defiant disorder, and even schizophrenia. Mindfulness is the practice of existing in the present moment without judg ment or harsh evaluations. These patients had not improved with shock therapy, supportive therapy, or medication. She was told to purposefully rehearse those thoughts without doing the rituals that she had used to decrease her obsessions. Such surgery sometimes left the patient with devastating side effects, such as an inability to function normally. A small continuing remains small and the research is quite pre study at Brown University, the Cleveland Clinic, liminary. And those who do benefit find that they relapse quickly if they discontinue the medication. Those with a very mild case may want to try some of the techniques described in this book on their own. Please read Chapter 22 to find out how to devise alternatives to giving reassurance. For example, they may ask someone to recheck that the doors are locked or that the oven is turned off. Though complying with the request may seem caring, doing so only makes matters worse. Moreno, indicated that daily ingestion of reported on a study involving psilocybin, the this drug would likely be problematic. You see, psychoactive substance found in psychedelic psychedelic mushrooms can also trigger trips mushrooms. All nine participants is not a treatment that we would recommend reported that they were symptom-free for peri at this time. For example, you may worry about whether you turned off the coffeepot, put the boarding pass in your briefcase, or left a light on as you rush off to the airport for an impor tant business trip. Occasionally feeling compelled to count steps, knock on wood, or arrange items on your nightstand in a particular pattern is also normal. These thoughts and behaviors may look downright bizarre, and occasionally funny, but we assure you that they are real and serious. These obsessions and compulsions can vary in both intensity and content over time. Thus, someone may have a terrible problem with compulsive hand-washing for two hours every day. After a year or so passes, the hand-washing may fall off, but compulsive rituals involving exces sive cleaning of the house and arranging the furniture precisely emerge in its place. See our earlier book, Overcoming Anxiety For Dummies, for more information about anxiety disorders. Once the obsessional worry about germs pops up in response to the sneeze, the person magnifies the risk or threat that the obsession poses. For example, the sneeze may be viewed as a spew of serious pathogens sprayed in the air. Completing the compulsion results in a short period of relief, which, in turn, actually increases the likeli hood that the compulsion will be used again. Even at home she disinfects her countertops and telephone dozens of times each day. Her overestimation of risk leads Cyan to feel intense anxiety and overwhelming dread. That distress causes her to immedi ately wash her hands with sanitizer and disinfect her computer keyboard, kitchen countertops, and phones. Obsessions are interpreted as serious dangers which lead to anxi ety and a compulsion to do something to reduce the risk in order to alleviate the anxiety. But she has enough doubts that she feels compelled to continue with her compulsive ritual. He may admit in a calm discussion that his beliefs are not completely consistent with reality. Consider the common superstition that knocking on wood after stating something positive will ward off bad things happening in the future. A compulsive action, such as arranging food alphabetically in the refrigerator, can feel as necessary as breathing. The impulse often involves an intense feeling or need for things to be just right. Distinguishing between obses sions and compulsions can seem a little tricky, but here goes. The difference between an obsession and a compulsion is that obsessions are intrusive mental events that make a person feel terribly upset. Compulsions, on the other hand, are behaviors or actions someone engages in either men tally (like counting or repeating words) or physically (like washing hands) in order to feel better. In other words, obsessions start in the mind and then create a negative emotional response, while compulsions are actions (either mental or physical) targeted to soothe negative emotions. Obsessing about obsessions Obsessions are like uninvited houseguests who refuse to leave. Obsessions come in three forms: Thoughts: Thoughts are the words that clang around in your head. Other examples of obsessive urges include worries that you may shout out obscenities during a religious ceremony or that you may turn your car into oncoming traffic. Images: these are uninvited pictures that form in your mind, often depicting violent, horrifying, morally reprehensible, weird, and unwanted scenes.
Order cheapest fincar and fincar
In the intermediate to long pain coping strategies that decrease fear and catastrophizing man health sa buy 5 mg fincar fast delivery, term, there is no established diference between behavioral (5) the early resumption of normal or vocational activities, journal of orthopaedic & sports physical therapy | volume 42 | number 4 | april 2012 | a39 Low Back Pain: Clinical Practice Guidelines even when still experiencing pain, and (6) the importance of be managed at lower-intensity levels of training. This sensitizing promotion strategies for patients with chronic low back pain process has been termed central sensitization. Clinicians should routinely assess activity limitation and participation restriction through validated performance-based measures. There is moderate evidence that clinicians should not Clinicians should consider utilizing thrust manipulative procedures to reduce pain and disability in patients with mobility defcits and acute utilize intermittent or static lumbar traction for reducing symptoms in patients with acute or subacute, nonradicular low back pain or in low back and back-related buttock or thigh pain. European guide of total hip replacement surgery on low back pain in severe osteoarthri lines for the management of chronic nonspecifc low back pain. The efcacy controlled prospective study with special reference to therapy and con of a short education program and a short physiotherapy program for founding factors. Outcome assessments in the evaluation of treatment of nosis and management of the aging spine. Natural history of individuals with sectional study of the isokinetic muscle trunk strength among school asymptomatic disc abnormalities in magnetic resonance imaging: pre children. Responsiveness of the numeric pain extension-oriented treatment approach in a subgroup of subjects with rating scale in patients with low back pain. Information and ad back pain: advice for high-value health care from the American Col vice to patients with back pain can have a positive efect. Exercise back pain: a joint clinical practice guideline from the American Col for treating fbromyalgia syndrome. Reliability of the hip examination in ing after acute back pain: results of a long-term follow-up study. Clarke J, van Tulder M, Blomberg S, de Vet H, van der Heijden G, Bron for the treatment of chronic low back pain: a randomized trial with fort G. Traction for low back pain with or without sciatica: an updated one-year follow-up. Efectiveness of manual physical therapy, therapeu on pain, disability, psychological strain, and serum cortisol concentra tic exercise, and patient education on bilateral disc displacement with tions in people with chronic low back pain. Comparison of the efectiveness of ability, and Health from the Orthopedic Section of the American Physi three manual physical therapy techniques in a subgroup of patients cal Therapy Association. J infuence of spinal canal narrowing and timing of decompression on Orthop Sports Phys Ther. Five questions predicted long-term, severe, back-related functional limi tations: evidence from three large prospective studies. Pain-related fear is more chronic low back pain: a comparison with healthy subjects. Medical screening and evacuation: cauda equina tion: a comparison between healthy subjects and patients with low back syndrome in a combat zone. Chronic back pain and major depression in the gen in fbromyalgia patients during standardised muscle exercise: a contrast eral Canadian population. Development of a clinical prediction rule to identify patients with knee pain and clinical evidence 94. Relative efectiveness of an extension of knee osteoarthritis who demonstrate a favorable short-term re program and a combined program of manipulation and fexion and ex sponse to hip mobilization. Trunk muscle endurance tests: reli bed versus advice to stay active for acute low-back pain and sci ability, and gender diferences in athletes. Lumbar muscle usage in use of an extension-mobilization category in acute low back syndrome: chronic low back pain. Outcome measures patients with low back pain who demonstrate short-term improvement for studying patients with low back pain. Epub nation of the reliability of a classifcation algorithm for subgrouping ahead of print. Pragmatic application of a clinical predic treated with slump stretching: a case series. Comparison of classifcation-based avoidance-based physical therapy intervention for patients with physical therapy with therapy based on clinical practice guidelines for patients with acute low back pain: a randomized clinical trial. Investigation of elevated fear-avoidance ments of the centralization phenomenon and status change during beliefs for patients with low back pain: a secondary analysis involving movement testing in patients with low back pain. Fear-avoidance beliefs as measured subgroups of patients with acute low back pain. Interrater reliabil by the fear-avoidance beliefs questionnaire: change in fear-avoidance ity and short-term treatment outcomes. Identifying psychosocial variables in patients with acute work-related low back pain: the importance of fear-avoidance 127. Efects of exercise on hip range of motion, trunk muscle performance, and gait economy. Reliability and validity of Functional Capacity Evaluation methods: a systematic 114. Is there a subgroup of review with reference to Blankenship system, Ergos work simulator, patients with low back pain likely to beneft from mechanical trac Ergo-Kit and Isernhagen work system. Accuracy of the clinical examination to predict radiographic instability of the lumbar spine. Lumbar spine segmental mobility assessment: an examination of validity for determining intervention 132. Factors related to the inability of individuals with low back pain to improve with a spinal 133. Responsiveness of a patient specifc outcome measure compared with the Oswestry Disability 134. Screening for symptoms of a clinical prediction rule for determining which patients with low back depression by physical therapists managing low back pain. Interrater reliability of clinical Mulligan traction straight leg raise: a pilot study to investigate efects examination measures for identifcation of lumbar segmental instability. Efects of the Mulligan trac disease in older adults: prevalence and clinical correlates. A systematic review of the relation between physical ca a predictor of reduced functional capacity in the health, aging and body pacity and future low back and neck/shoulder pain. Long-term efects of specifc stabiliz dent evaluation of a clinical prediction rule for spinal manipulative ing exercises for frst-episode low back pain. The inter-tester reliability of physical multifdus muscle wasting ipsilateral to symptoms in patients with therapists classifying low back pain problems based on the movement acute/subacute low back pain. Screening for malignancy in low laboratory and clinical tests of transversus abdominis function. Predicting the onset of widespread cise program reduces disability and improves functional performance body pain among children. Segmental lumbar mobility in intervention to treat recurrent nonspecifc low back pain in adolescents. A school-based survey of recurrent non-specifc low-back pain prevalence and consequences in 192. Interexaminer reliability of low back pain assessment using the Mc recurrent musculoskeletal pain: developing a screening instrument. Evaluation of the predictive validity of the the treatment of workers with chronic low back pain: a randomized, Orebro Musculoskeletal Pain Screening Questionnaire. Cytokines for psychologists: implications of bidi tion as a screening test for identifying occupational low back pain. J rectional immune-to-brain communication for understanding behavior, Orthop Sports Phys Ther. Endurance times for low back stabi sensitization in patients with musculoskeletal pain: application of pain lization exercises: clinical targets for testing and training from a normal neurophysiology in manual therapy practice. Interpreting change scores for Practice analysis survey: revalidation of advanced clinical practice in or pain and functional status in low back pain: towards international thopaedic physical therapy.
Order generic fincar online
The gold bath is non cyanide and is used for electroforming dental prosthetic restorations androgen hormone questionnaire buy generic fincar 5 mg. Code Addition free and filler free silicone For blocking out undercuts on the for fabricating duplication models, electroforming plaster die. Code 3 x 4g Blocset liquid Duplication fask B 6600 0458 Duplication fask C 6600 0459 Delivery form Art. Material: stainless steel tomeric impression materials, silicone duplicating materials and pattern waxes Advantages Dimensions as well as increasing the accuracy of Exceptional thixotropy O 0. Code For use with: Suitable for pouring up to Elastomeric impression materials 4 dental arches 200 pieces 6600 0463 Silicone duplicating materials and wax patterns Delivery form Art. Code aluminium bags 6600 0235 1000 ml bottle 6450 0983 in a carton Preciano special brushes For applying silver conductive lacquer Delivery form Art. Code 3 pieces 6600 0464 Preciano conductive silver lacquer For fabrication of an electrically conductive contact layer on objects set up for electroforming. Code dual curing composite for the fixation of prefabricated and tailored attachments. Special plasters, type 3 all-round hard and type 4 superhard plasters are developed, optimised and processed in close cooperation with the manufacturer. After mixing it is stable and Advantages Advantages is very good for shaping and handling. After mixing it is stable and with base formers such as the Kulzer is very good for shaping and handling. The mixed plaster is very flowable and is remarkable for its Shade very low setting expansion. Thixotropy is the phenomenon where materials With the Type 4 dental plasters from and, regain their original firm become fluid when subjected to Kulzer this means that these: consistency immediately after the mechanical forces such as stirring, flow into very thin areas under mechanical activity has ceased. Code 20kg, beige, aluminium bags 18kg, light brown, in a shipping carton aluminium bags* 6587 0807 20 kg (4 x 5 kg) 6600 0240 4 x 4. Increased expansion Increased expansion Trimming water was added to the mixing water. Low final hardness Low final hardness Trimming water was added to the mixing water. Setting acceleration Setting acceleration Set stone residue adhering to the mixing vessel, mixing paddles or spatula. Depending on the type of stone, allow 30 to 45 minutes before removing the model from the impression. Some soft areas on the surface of the model Some soft areas on the surface of the model Residual wetting agent or disinfectant in the impression. Unsatisfactory fit of removable dies in the model base Unsatisfactory fit of removable dies in the model base Grinding dust, stone particles etc. Streaky, distorted stone model surface Streaky, distorted stone model surface Deformed/damaged impression. Increase in the expansion and reduction in the strength of the set model Increase in the expansion and reduction in the strength of the set model Too much water came into contact with the model after it was removed from the impression Keep contact with water to a minimum. Reduction in detail reproduction on finished model Reduction in detail reproduction on finished model the impression was poured using a stone with reduced flowability and the stone had begun to set. Non parallel saw cuts on the model Non-parallel saw cuts on the model Saw blade was blunt. They have the surfaces of these materials greatly the plaster through repeated removal of same properties and advantages. The plastic sleeves did in Indication Metal sleeve, the initial removal of the arch after the Elastomeric impression materials Brass, 6450 0912 base plaster has set. Code Step pins with 500 pieces plastic sleeves, 6460 1105 1000 ml bottle 6450 0983 Pin drill O 1. Code Fripack is a stiff plastic container, the manufacturing of models with available in two sizes. It is the ideal optional magnet secured primary or 1 spray bottle 6450 0989 covered container for impressions, secondary bases, for plaster models, and prostheses. Blue Profile and Prepon pearl wax for crowns and bridges and Palavit G waxing material for casting. Ensuring that they work with maximum accuracy, continuously improve their knowledge and work with their colleagues to manufacture very high quality products. Code nent modelling synthetic material Manufacturing of crown and bridge formed from powder and liquid. Heravest Speed has played a major role in the development of speed investment compounds. Hera by Kulzer is subject to high standards to ensure that reproducible quality can be achieved. Advantages Heravest M print+ is recommended Outstanding flowability for fast preheating. Advantages Excellent fit Outstanding flowability Smooth surfaces Advantages Excellent fit Results oriented and clinic tested Excellent fit Smooth surfaces Clean cast object Results oriented and laboratory Indication Smooth surfaces tested Cast partial denture Indication Indication Delivery form Art. Code Cast partial denture Cast partial denture 20 kg carton Delivery form Art. Code 125 x 160 g bags 20 kg carton 20 kg carton 20 kg carton (4 x 5 kg) 6460 1439 containing 6606 9118 containing 6450 0611 50 x 400 g bags 125 x160 g bags 20 kg carton (4 x 5 kg) 6450 0612 Heravest M and Heravest M 2000 are excellent for pouring CoCr cast partial denture alloys. The disposable For speed preheating plungers save time-consuming cleaning For conventional programmed of reusable plungers. Heravest 6604 3951 Easily devested disposable plunger Indication Inlays Partial crowns Crown, small bridges Delivery form Art.
Ocimum tenuiflorum (Holy Basil). Fincar.
- How does Holy Basil work?
- What is Holy Basil?
- Diabetes, common cold, influenza ("the flu"), asthma, bronchitis, earache, headache, stomach upset, heart disease, fever, viral hepatitis, malaria, tuberculosis, mercury poisoning, use as an antidote to snake and scorpion bites, or ringworm.
- Are there safety concerns?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97047
Buy fincar 5mg with mastercard
Sometimes they want to become pregnant and worry about possible effects on the developing fetus prostate oncology 2017 order 5mg fincar amex. Other times, they experience distressing side effects, such as weight gain, dizziness, nausea, loss of sexual desire and/or inabil ity to experience orgasms. And for some, discontinuing medication simply reflects a personal philosophical preference. If you choose to go off your medication, you can reduce the risk of relapse by heeding the following advice: Continue medication for at least a year or two before considering dis continuance. If symptoms return, consider going back on medication, perhaps even for a lifetime. Most studies suggest that medication does not increase your risk of relapse following suc cessful combined treatment. Similar evidence suggests that mindfulness may also reduce the risk of depression relapse. The vast majority of people continue to have some mild symptoms that are occasionally irritating or annoying. Here are three approaches for dealing with relapse: Do what worked for you before. Treatment is usually more efficient the second time around because you already know what to expect. If you go back and find that what worked before is no longer effective, other treatment alternatives are available. Nevertheless, relapse happens no matter what the problem is or what ther apy is being used. Chapter 12: Responding to and Recovering from Relapse 189 Knowing the difference between a lapse and a relapse Chapter 8 tells you that the way you interpret events makes a huge difference in the way you end up feeling. By contrast, a relapse is considered to be a major regression toward pre-treatment functioning. He is first referred for help when his primary care provider notices that his hands are raw and bleeding. Jeremy confesses that he often spends an hour in his shower and washes his hands hundreds of times during the day. He purposely waits until the thoughts pass and does not engage in compulsive wash ing. And Jeremy had been informed that such thoughts would no doubt pop back into his mind from time to time. Armed with that information, Jeremy understands that his obsessions are normal, expected, and something that he can handle. He knows if they happen to worsen, he now has skills and tools for dealing with them. Revealing a relapse A relapse can begin with a lapse and then spiral downward from there, resulting in a full-blown return of obsessions and compulsions. In the following example, Todd initially makes a good decision to seek help for his compulsive hand-washing. Todd talks about this with his primary care doctor, who tells Todd about different kinds of treatment. Todd and his doctor choose to try an antidepressant to see whether that will help. The more he thinks about it, the more he begins to avoid public places and engage in compul sive washing. In almost all of those cases, we suggest multi-pronged treatments involving most of the strategies we discuss in this book. Chapter 12: Responding to and Recovering from Relapse 191 Phasing out your sessions gradually the relationship between you and a therapist is unique. Most of the time, this happens when the client and therapist agree that the goals of treatment have been met. Staging a fire drill If you work in a school or hospital, you probably run through fire drills from time to time. Therefore, we suggest that following successful treatment, you actually create a log and track your obsessions and compulsions. You may also find it useful to ask yourself whether these feelings are based on clear evidence that most people would agree is valid. Generally speaking, such evidence should be based on things that you can clearly see, touch, hear, smell, or taste. Feeling as if you must avoid all negative feelings Please realize that negative feelings absolutely cannot be avoided in life. If you try to avoid all such feelings, relapse may be waiting around the next corner, ready to pounce. We find that physical training provides an excellent analogy for helping you think about this issue. These benefits include: Enhanced sense of well-being Increased endurance Increased flexibility Increased mobility Increased strength Reduced pain Tolerating the discomfort associated with obsessions works exactly the same way. But the more you resist caving into the discomfort with your usual compulsions, the more your tolerance increases and the less discomfort you feel. Many of their concerns have a remote chance of happening, but a few are extremely bizarre and unrealistic. Normal body fluctuations, such as muscle soreness after exercise, turn into an esoteric, degenerative neurological disease in their minds.
Order fincar 5mg line
Because these behaviors are common among siblings prostate cancer gene buy fincar overnight delivery, they must be observed during interactions with persons other than siblings. Also, because symptoms of the disorder are typically more evident in interactions with adults or peers whom the individual knows well, they may not be apparent during a clinical examination. First, the diagnostic threshold of four or more symptoms within the preceding 6months must be met. For example, it is not unusual for preschool children to show temper tantrums on a weekly basis. The symptoms of the disorder often are part of a pattern of problematic interactions with others. Furthermore, individuals with this disorder typically do not regard themselves as angry, oppositional, or defiant. Instead, they often justify their behavior as a response to unreasonable demands or circumstances. Whether or not the clinician can separate the relative contributions of potential causal factors should not influence whether or not the diagnosis is made. In the event that the child may be living in particularly poor conditions where neglect or mistreatment may occur. Associated Features Supporting Diagnosis In children and adolescents, oppositional defiant disorder is more prevalent in families in which child care is disrupted by a succession of different caregivers or in families in which harsh, inconsistent, or neglectful child-rearing practices are common. Oppositional defiant disorder has been associated with increased risk for suicide attempts, even after comorbid disorders are controlled for. Prevaience the prevalence of oppositional defiant disorder ranges from 1% to 11%, with an average prevalence estimate of around 3. The rate of oppositional defiant disorder may vary depending on the age and gender of the child. This male predominance is not consistently found in samples of adolescents or adults. Development and Course the first symptoms of oppositional defiant disorder usually appear during the preschool years and rarely later than early adolescence. Oppositional defiant disorder often precedes the development of conduct disorder, especially for those with the childhood-onset type of conduct disorder. However, many children and adolescents with oppositional defiant disorder do not subsequently develop conduct disorder. Oppositional defiant disorder also conveys risk for the development of anxiety disorders and major depressive disorder, even in the absence of conduct disorder. Thus, it is unclear whether there are markers specific to oppositional defiant disorder. Culture-R elated Diagnostic Issues the prevalence of the disorder in children and adolescents is relatively consistent across countries that differ in race and ethnicity. Functional Consequences of Oppositional Defiant Disorder When oppositional defiant disorder is persistent throughout development, individuals with the disorder experience frequent conflicts with parents, teachers, supervisors, peers, and romantic partners. Conduct disorder and oppositional defiant disorder are both related to conduct problems that bring the individual in conflict with adults and other authority figures. Furthermore, oppositional defiant disorder includes problems of emotional dysregulation. As a result, a diagnosis of oppositional defiant disorder should not be made if the symptoms occur exclusively during the course of a mood disorder. However, the severity, frequency, and chronicity of temper outbursts are more severe in individuals with disruptive mood dysregulation disorder than in those with oppositional defiant disorder. However, individuals with this disorder show serious aggression toward others that is not part of the definition of oppositional defiant disorder. Oppositional defiant disorder must also be distinguished from a failure to follow directions that is the result of impaired language comprehension. Also, oppositional defiant disorder often precedes conduct disorder, although this appears to be most common in children with the childhood-onset subtype. Recurrent behavioral outbursts representing a failure to control aggressive impulses as manifested by either of the following; 1. The magnitude of aggressiveness expressed during the recurrent outbursts is grossly out of proportion to the provocation or to any precipitating psychosocial stressors. For children ages 6-18 years, aggressive behavior that occurs as part of an adjustment disorder should not be considered for this diagnosis. Diagnostic Features the impulsive (or anger-based) aggressive outbursts in intermittent explosive disorder have a rapid onset and, typically, little or no prodromal period. Outbursts typically last for less than 30 minutes and commonly occur in response to a minor provocation by a close intimate or associate.
Fincar 5mg without a prescription
The Premenstrual Tension Syndrome Rating Scale has a self-report and an observer version prostate cancer latest news discount 5 mg fincar with amex, both of v^hich have been validated and used widely to measure illness severity in women who have premenstrual dysphoric disorder. Functional Consequences of Prem enstrual Dysphoric Disorder Symptoms must be associated with clinically meaningful distress and/or an obvious and marked impairment in the ability to function socially or occupationally in the week prior to menses. Impairment in social functioning may be manifested by marital discord and problems with children, other family members, or friends. Premenstrual syndrome differs from premenstrual dysphoric disorder in that a minimum of five symptoms is not required, and there is no stipulation of affective symptoms for individuals who have premenstrual syndrome. This condition may be more common than premenstrual dysphoric disorder, although the estimated prevalence of premenstrual syndrome varies. While premenstrual syndrome shares the feature of symptom expression during the premenstrual phase of the menstrual cycle, it is generally considered to be less severe than premenstrual dysphoric disorder. Dysmenorrhea is a syndrome of painful menses, but this is distinct from a syndrome characterized by affective changes. Bipolar disorder, major depressive disorder, and persistent depressive disorder (dysthymia). Many women with (either naturally occurring or substance/medication induced) bipolar or major depressive disorder or persistent depressive disorder believe that they have premenstrual dysphoric disorder. However, when they chart symptoms, they realize that the symptoms do not follow a premenstrual pattern. However, because the onset of menses constitutes a memorable event, they may report that symptoms occur only during the premenstruum or that symptoms worsen premenstrually. This is one of the rationales for the requirement that symptoms be confirmed by daily prospective ratings. If the woman stops hormones and the symptoms disappear, this is consistent with substance/medication-induced depressive disorder. Comorbidity A major depressive episode is the most frequently reported previous disorder in individuals presenting with premenstrual dysphoric disorder. These conditions are better considered premenstrual exacerbation of a current mental or medical disorder. There is evidence from the history, physical examination, or laboratory findings of both (1)and(2): 1. The disturbance is not better explained by a depressive disorder that is not substance/ medication-induced. The name of the substance/medication-induced depressive disorder begins with the specific substance. For example, in the qase of depressive symptoms occurring during withdrawal in a man with a severe cocaine use disorder, the diagnosis is 292. If the substance-induced depressive disorder occurs without a comorbid substance use disorder. When more than one substance is judged to play a significant role in the development of depressive mood symptoms, each should be listed separately. In addition, the diagnosis is not better explained by an independent depressive disorder. This diagnosis should not be made when symptoms occur exclusively during the course of a delirium (Criterion D). Clinical judgment is essential to determine whether the medication is truly associated with inducing the depressive disorder or whether a primary depressive disorder happened to have its onset while the person was receiving the treatment. A substance/medication-induced depressive disorder is distinguished from a primary depressive disorder by considering the onset, course, and other factors associated with the substance use. Development and Course A depressive disorder associated with the use of substance. Most often, the depressive disorder has its onset within the first few weeks or 1 month of use of the substance. If symptoms persist 4 weeks beyond the expected time course of withdrawal of a particular substance/medication, other causes for the depressive mood symptoms should be considered. However, other potential substances continue to emerge as new compounds are synthesized. Factors that appear to increase the risk of substance/medication induced depressive disorder can be conceptualized as pertaining to the specific type of drug or to a group of individuals with underlying alcohol or drug use disorders. Environmental, There are also risks factors pertaining to a specific type of medication.

Purchase fincar overnight
The premise is that the way you interpret situations (what you think) determines your emotional response (what you feel) prostate cancer active surveillance purchase fincar 5 mg mastercard. Hundreds of studies have shown that learning to change the way you think can improve the way you feel. For example, the obsession about whether one closed the windows in the house before leaving is not connected to not having felt the windows actually click shut. Similarly, those imagined microbes emanating from the microwave cannot be seen, felt, or touched. Obsessive thoughts that cause distress are usually based on a premise that something really bad may happen. Maybe, just maybe the obsession will come true if action is not taken to prevent it. And if something is burning on your stove, you can see or smell smoke coming from the kitchen. Those warning signs are put there by people who are knowledgeable about the risks and whose senses (often aided by scientific instruments) enable them to assess specific risks that others might not be aware of. But as the story departs from that which can be confirmed by your senses, it also drifts far from any likely reality. Dismissing unrealistic doubts the first step toward changing the way you think is becoming aware of the basis for your thoughts. Does your doubt seem to have a life of its own and keep coming back, even without new evidence to support it A few months earlier, they both came down with a case of food poisoning after eating hamburgers in a messy airport restaurant. She no longer eats at restaurants, opting to carry her own food wherever she goes. At a sales conference, Pam and Debbie are seated at the same table for a company luncheon. Debbie tells Pam that she had a few qualms and doubts for a little while about eating in airport restaurants, and tends to avoid ordering rare hamburgers now; plus she checks the place out for general cleanliness. She now takes precautions to avoid undercooked meat and messy-looking restaurants. She avoids all restaurants and imagines microbes and diseases that cannot be seen. Filtering doubts through the series of questions we present earlier in this section can help you determine whether your doubts are reasonable or not. She ate an direct information from your undercooked, bad undercooked ham senses (sight, sound, smell, hamburger in a burger in a messy taste, or touch) She cannot see the microbes she imag ines and cannot tell whether her waiters have diseases. The more Pam have a life of its own and keep occasional qualm, thinks about her coming back even without new but those have doubts, the more they evidence to support it Most people doubt that other people would to avoid unclean know that eating in see as illogical But doubt and uncertainty can never be fully eliminated and must be accepted as an inherent part of life. However, they proceed to touch many door knobs each day knowing that the actual risk they incur each time is rather small. These sirens urge the person to take immediate action to eliminate the viruses and avoid illness. Jesus was crucified, Thomas did not believe Faith is known to be extremely helpful for bil that Jesus had risen from the dead. So if you want to act on faith, do it with following week, Jesus appeared to Thomas respect to spirituality, not to deal with obses and allowed him to touch his wounds. Consider answer ing these questions: Do I have any direct evidence that is contrary to my fears How often have my fears of this risk come true (versus not coming true) in the past There is a clinic near her workplace, and she walks several blocks out of her way in order to avoid coming close to the clinic. Her therapist asks her to estimate the probability that serious, potentially lethal contaminates could be picked up simply by walking near the clinic. He asks her to search for any evidence or logic she can think of that might change her estimated risks. She comes up with the following evidence and logic: If the real risk was 10 percent, that would mean that a full 10 percent of those who walk by the clinic would die. If walking by a clinic incurs a 10 percent risk, then working there would probably kill off half of the employees within a short time. Just because you think something weird, strange, immoral, or cruel, does not mean that you are bad, crazy, or mean. When that happens to most people, the thoughts are quickly dismissed or forgotten. Calculating real probabilities About 5,000 people die each year from food you have almost a 40 percent chance of dying poisoning in the United States. At last every outbreak of salmonella and such every count, over 304 million people lived in the United time one occurs. So take 304 million 3 365, and you get 332,880,000,000 (a little more than Obviously, you want to avoid buying tomatoes 332 billion) meals consumed each year. Five thou or spinach when there is a sudden, known out sand of these meals kill someone. And you should wash your vegetables of dying from any given meal are about one in thoroughly and avoid leaving your mayonnaise 6,657,600. In fact, you may not think about the thought at all and go get yourself a cold drink instead. I better start counting the ceiling tiles to distract myself from that horrible thought.
5mg fincar with mastercard
While ture may normally improve after 6 months to a year prostate cancer gleason scale fincar 5mg sale, the vast majority of complications are minor, some se the contribution of the pump implant to the reduc rious complications can occur (27,225,506,2077,2099 tion in pain scores in this study is unclear. An increased mortality rate in vertebroplasty and kyphoplasty are less expensive op patients with non-cancer pain receiving intrathecal tions compared to an intrathecal infusion pump. Kumar et serious complications include granuloma formation al (2012) looked at the cost of implanting a program that may be related to the amount and concentra mable drug delivery pump versus conservative treat tion of opiates, mostly morphine and hydromor ment of chronic pain. Granulomas may oc of equipment required for intrathecal drug delivery cur in as many as 3% of implanted patients and were recovered by 28 months. The earliest sign of patients in the intrathecal drug delivery group, com granuloma may be increased pain despite increasing pared with a 12% improvement in the control group. Study Pain Relief and Results Function Study Short Long Characteristics Participants Outcome Measures Term Term < 12 mos. Intrathecal infusion systems for long-term management of chronic non-cancer pain: An update of assessment of evidence. Otherwise, of various identifiable sources of chronic spinal pain an algorithmic approach should include diagnostic in (8,2155). However, this may not time, lumbar discography time suffers from significant be applicable in each and every patient. In contrast, there is of the described algorithmic approach is to provide a good evidence to support facet joint nerve blocks in the disciplined approach to the use of spinal interventional diagnosis of lumbar facet joint pain and sacroiliac joint techniques in managing spinal pain. Furthermore, with illustrated the prevalence of lumbar facet joint pain in space constraints, comprehensive initial evaluations 15% to 45% of patients and false-positive rates of 27% and all the findings are not provided. Appropriate history, physical examination, and Furthermore, among all the diagnostic approaches in medical decision-making are essential to the provision the lumbosacral spine, medial branch blocks have the of appropriate documentation and patient care. Not best evidence of accuracy with their ability to rule out covered in this algorithm are socioeconomic issues false-positives and demonstrated validity with multiple and psychosocial factors that may be important in the compounding factors, including psychological factors, clinical decision-making process. In this complete evaluation will assist in complying with regu approach, the investigation of facet joint pain is con lations, providing appropriate care, and fulfilling an sidered as a prime investigation, ahead of disc provoca algorithmic approach. In the United States, commonly proach for chronic low back pain without disc hernia performed diagnostic blocks are often accomplished tion (8,2155). If a patient expe algorithmic approach for chronic low back pain without riences at least 75% relief with the ability to perform disc herniation is based on the best available evidence previously painful movements within a timeframe that on the epidemiology of various identifiable sources of is appropriate for the duration of the local anesthetic chronic low back pain. Facet joint pain, discogenic pain, used and the duration of relief with the second block and sacroiliac joint pain have been proven to be com relative to the first block is commensurate with the re mon causes of pain with proven diagnostic techniques spective local anesthetic employed in each block, then, (8,11,13,15,17,33,36-38,644,1250,1325,1469,1471,2155). However, based on patient If there is evidence of radiculitis, spinal stenosis, condition and regulations, the criterion standard of A comprehensive algorithm for the evaluation and management of chronic spinal pain. An algorithmic approach to diagnosis of chronic low back pain without disc herniation. In that case, only one negative disc is needed with tenderness over the sacroiliac joint (8,17,1461). Lumbar provocation discography is the the ability to perform previously painful movements last step in the diagnostic algorithm and is utilized only and also should be concordant based on the local anes when appropriate treatment can be performed if disc thetic injection with a bupivacaine injection outlasting abnormality is noted (8,2155). Caudal and lumbar inter low back pain without disc herniation or spinal stenosis. Pro Even though, disc protrusion, herniation, and pro vocative lumbar discography is performed as the first lapse resulting in sciatica are seen in less than 5% of the test in only specific settings of suspected discogenic patients with low back pain (374,554,1559), many patients pain and availability of a definitive treatment is offered with post surgery syndrome, spinal stenosis, and radiculitis or solely for diagnostic purposes prior to fusion. Other without disc protrusion may respond to epidural injections wise, once facet joint pain, and if applicable sacroiliac (8-10,28,30,31,722,765,766,906,968,1037,1038,1759). Pa joint pain, is ruled out and the patient fails to respond tients non-responsive to epidural injections will require to at least 2 fluoroscopically directed epidural injec either mechanical disc decompression (21-24), percuta tions, discography may be pursued if determination of neous adhesiolysis (19), or implantation of a spinal cord the disc as the source of pain is crucial. Provocation dis lumbar transforaminal epidural injections in managing cography continues to be controversial with respect to radicular pain or disc herniation (28,30,31). In addition, diagnostic accuracy and its impact on surgical volume the evidence is fair for caudal, lumbar interlaminar, and (39). Lumbar discography has been refined substantially transforaminal epidural injections in managing spinal ste since its inception and its diagnostic accuracy is fair (39). The evidence for lumbar interlaminar to good for lumbar facet joint nerve blocks and good for epidural injections in post surgery syndrome is not avail lumbar radiofrequency neurotomy (12). The evidence assessment is based on contemporary the next modality of treatment is epidural injec practice in interventional pain management settings for tions. Epidural injections show variable evidence in all the procedures performed under fluoroscopy. The as Consequently, a patient without previous surgical sessment of the evidence from these guidelines and intervention with unilateral, single, or 2 level involve systematic reviews (28,30,31) is fair with caudal and ment may be treated with transforaminal, caudal, or interlaminar epidural injections and limited with trans interlaminar approaches. However, bilateral or involve foraminal epidural injections in managing axial or dis ment of multiple segments will lead to either interlami cogenic pain without disc herniation, radiculitis, facet nar or caudal epidural injections based on the upper or joint pain, or sacroiliac joint pain. In case of extensive stenosis the evidence for therapeutic sacroiliac joint inter or lack of response to caudal or interlaminar approaches, ventions is fair for cooled radiofrequency neurotomy, transforaminal epidural approach may be appropriate. Figure 10 illustrates therapeutic algorithmic man the assessment of evidence for intradiscal proce agement. In contrast, based on the re may be considered for mechanical disc decompression, Chronic Low Back Pain Somatic Pain Radicular Pain I. Post surgery Cooled radiofrequency thermoneurolysis Step 4: Spinal cord stimulation *Evidence is limited **Evidence available only for post surgery syndrome and spinal stenosis Fig. A suggested algorithm for therapeutic interventional techniques in management of chronic low back pain. Only recently, one randomized trial dural injections is good for radiculitis secondary to disc was conducted for nucleoplasty providing fair evidence. In contrast, cervical transforaminal epidural injec In patients with post-lumbar surgery syndrome tions have been associated with high risk and without after failure to respond to fluoroscopically directed evidence either for diagnostic or therapeutic purposes epidural injections, percutaneous adhesiolysis is con (934,1010,1023-1031,1646,1758). Based on the current literature, the approach should include the diagnostic interventions evidence is fair to good for percutaneous adhesiolysis with facet joint blocks, therapeutic epidural injections, in managing post lumbar surgery syndrome and spinal followed by discography. Thus, the facet joints are been tried without sufficient improvement in pain con entertained first in the algorithm in patients without trol. Multiple studies have cancer pain may be achieved with intrathecal infusion indicated the facet joint pain to be bilateral in 69% to systems (27). The 72% of cases and involving at least 3 joints in 50% to literature continues to be scant with no randomized trials 85% of patients (14,1345-1347,1857). This with 2 different local anesthetics, a positive diagnosis is represents an algorithmic approach for the investigation made. However, based on patient condition and regula of neck pain based on the best available evidence on the tions, the criterion standard of pain relief and either a S186 An algorithmic approach to diagnosis of chronic neck pain without disc herniation. Once facet joint pain is ruled out and the is the last step in the diagnostic algorithm and is utilized patient fails to respond to at least 2 fluoroscopically only when appropriate treatment can be offered if the directed epidural injections, discography may be pur disc abnormality is demonstrated. However, to be valid, the provocation sions if the patient does not improve with any other discography must be performed utilizing criteria with modalities of treatment. Thus far, studies have demon concordant pain in one disc with at least 2 negative strated the effectiveness of epidural injections in the discs, with evoked intensity of pain of 7 of 10 or 70% of cervical region in discogenic pain (9,13,38,251,746,772, worst spontaneous pain. These modalities in managing spinal stenosis are less common in the cervical spine chronic intractable neck pain have not been evaluated. Ra diculitis may also result from cervical spinal stenosis, post surgery syndrome, and discogenic pain without 4. The current evidence indicates lack of Figure 13 illustrates the diagnostic algorithmic ap evidence for transforaminal epidural injections and proach for chronic thoracic pain without disc herniation high risk with good evidence for cervical interlaminar or radiculitis.