
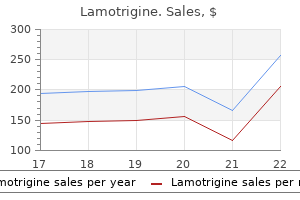
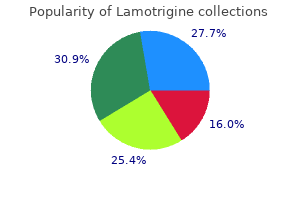
Lamotrigine
Order 200mg lamotrigine mastercard
They see pa learning how to perform surgery may tients in the hospital requiring sur seem daunting medicine for stomach pain buy lamotrigine 50 mg without prescription, in reality anyone in a gical consult and master the es solid residency program and with a mod sentials of postoperative care of icum of dedication can learn the techni patients on the surgical wards cal aspects of surgery. Operating In the operating room, surgeons room time increases throughout learn the proper use of hundreds of in the year. Residents spend the struments, from scalpels and scissors to rst 2 years primarily in general retractors and needle drivers. To give res surgery but also rotating through idents even more experience with these surgical subspecialties like neuro tools, surgical skills laboratories have be surgery, urology, and orthopedics. The remaining 3 years are dedi They incorporate inanimate models, vir cated to improving operating tual reality, animal labs, and cadavers skills through rotations in general, into surgical training. For example, rst vascular, cardiothoracic, pediatric, year residents often complete sessions on and transplant surgery. Additional tying knots or performing laparoscopic months of training include surgi appendectomy in pigs, while the senior cal intensive care and endoscopy. This type of surgery seeks to provide alter natives to open surgery, including laparoscopic surgery and robotic surgery. La paroscopy involves making small incisions and inserting ports to gain access to the abdomen or chest and to place cameras and instruments. By not opening up a patient, this approach shortens recuperation time and reduces potential post operative complications. It also provides a different point of view from which to see the anatomy and attack the problem at hand. Learning the latest operative techniques, therefore, means a lifetime of constant reeducation and self-disci pline. This does not imply, though, that surgeons are simply technicians who only make incisions and tie knots. Remember: many patients undergoing surgical evaluation may not end up needing an operation. A thorough understanding of countless as pects of clinical medicine, therefore, is necessary for surgeons to make these to-cut or-not-to-cut decisions. An old cliche is that you can teach a monkey to operate, the problem is teaching him when not to . Surgeons cannot always predict problems during an opera tion, so they must be levelheaded and ready for anything. This requires a mas tery of anatomy and common anatomic abnormalities, physiology and patho physiology of disease, as well as of proper surgical technique and options for treatment. For example, to safely perform a laparoscopic cholecystectomy, sur geons must know the common anatomic variations of cystic artery, hepatic ar teries, and the ductal system. They have to understand unusual disorders of the biliary tract like Mirizzi syndrome and parasitic diseases like Clonorchis sinensis infection to accurately interpret the clinical, radiographic, and intra-operative ndings. Surgeons must know when it is appropriate to perform cholecystectomy rather than simply placing a cholecystostomy tube. This question often arises with the elderly and debilitated or those who refuse surgical intervention. You have to feel comfortable managing co morbid medical problems like diabetes as well as any medical complications of surgery. For instance, the administration of general anesthesia and the physio logic demands of major surgery increase the risk for myocardial infarction. Surgeons also identify common and dire diseases of the lung, includ ing pulmonary embolism and edema. Other common peri-operative issues include abscess formation, sepsis, systemic in ammatory response, and multi organ system failure. Likewise, they often perform their own bronchoscopies and upper and lower gas trointestinal endoscopies. Or perhaps an intra-abdominal abscess that could be safely drained percutaneously by col leagues in interventional radiology Although radiologists are usually available to interpret the appropriate imaging studies, surgeons like to read their own lms, too. Like all other doctors, surgeons always begin with a focused history and phys ical before making the diagnosis and the decision to operate. In a typical day, sur geons may receive a page from the emergency department regarding an elderly pa tient with abdominal pain, emesis, and increased white blood cell count. The surgeon must ask focused questions to determine the acuity of the consult and pri oritize the order in which patients will be seen. Proper clinical judgment deter mines what tests must be ordered, if further radiographic studies are appropriate, or if the patient should proceed directly to the operating room. What differentiates surgical disciplines from other elds is the limited time available to assimilate reams of information from the history, physical, laboratory results, and radiologic studies to come to the correct diagnosis and implement the proper course of action. Rather, surgeons typically have close long-term rela tionships with their patients. In other specialties of medicine, patients play an active role in their treatment simply by being compliant with their prescribed medication regimen. When it comes to surgery, however, patients have to bestow their undivided trust on their surgeon and give up all control over their care once the operation begins. Pa tients are entrusting their welfare and their lives to your clinical judgment and technical skill. They are apprehensive about undergoing even simple operations like removing an obstructed gallbladder or an in amed appendix. It is a daunt ing, frightening experience to allow another person to cut them open and ma nipulate their internal organs. At this point, patients are unable to answer ques tions, express their wants or beliefs, or provide any input regarding their care. As a patient, you must trust that in an emergency your surgeon will have the knowledge, presence of mind, and skill to do what it takes to save your life. De spite all the technology involved in an operation, surgeons still have a great deal of interaction with their patients. Many procedures end up having a long-term emotional impact, such as a mastectomy, so you must be prepared to address these concerns as well. Before ever doing a surgical rotation, students hear tales of screaming chief residents and attending surgeons who throw instruments. There are many stereotypes about the typical surgeon personality, perhaps more than in any other specialty. Others have the misperception that surgeons are overbearing, overworked, and often cold physicians. These qualities re ect the level of dedication and personal responsibility the surgeon takes over the care of her or his patients. After all, surgeons need the con dence and ability to be assertive when necessary. Remarkably, these characteristics have been ex tensively studied and well represented in the surgical literature. A recent study, for instance, examined the traits that are more common in surgeons than in the general population. They also concluded that sur geons are more likely to be aggressive, prefer competition, and express their anger when necessary. Given these observations about the so-called surgical personality, what does it actually take to be a surgeon A professor of surgery once commented: You dont have to be smart; you just have to care enough and work hard. It is ironic that the typical surgeon perceived by young doctors-in-training is a lone wolf, self directed and independent, whereas the success of the individual surgeon de pends on working well as a member of the team.
Order lamotrigine with amex
Passive lateral flexion of the neck to the right is limited symptoms inner ear infection lamotrigine 100 mg free shipping, and there is a firm, well circumscribed mass palpable on the left inferolateral aspect of the neck. Congenital muscular torticollis is the most common cause of torticollis in infants. The etiology of the muscular trauma is uncertain, but experts theorize that it results from positioning during fetal head descent or abnormal intrauterine positioning. Others suggest that it is due to direct trauma to the muscle during difficult deliveries. It is a prominent cause of positional plagiocephaly, and prompt treatment early in infancy can prevent this deformity. In infants with congenital muscular torticollis, the head is usually tilted toward the side of the injured muscle. There may be skull and facial asymmetry, including jaw asymmetry, and the ear and eye ipsilateral to the injured side can appear smaller. A cephalocaudal view of the infant can highlight the asymmetry on physical examination (Item C231). In infants, full passive range of motion in rotation is 100 degrees to 110 degrees, and full cervical passive range of motion in lateral flexion is between 65 degrees and 75 degrees. Most infants respond to a home exercise program, which can be taught to caregivers by pediatricians or physical therapists. Prone positioning while awake (tummy time) may decrease the risk of positional plagiocephaly. Affected infants commonly exhibit fussiness with movement of the arm on the involved side. The fracture is self-resolving, but can be associated with brachial plexus injury. Affected infants commonly develop head tilt in an attempt to improve vision; however, a sternocleidomastoid muscle mass is not associated with this condition. The efficacy of topiramate in benign paroxysmal torticollis of infancy: report of four cases. The newborn required resuscitation with positive pressure ventilation in the delivery room. He has warm, pink extremities with capillary refill time of 3 seconds, clear and equal lung sounds bilaterally, and a right flank mass. Ultrasonographic examination is significant for an enlarged right kidney with loss of corticomedullary differentiation. In a full-term neonate, the serum creatinine concentration normalizes in 7 to 10 days, whereas in a preterm infant, it may take up to 1 month to normalize. For management of neonatal acute kidney injury, it is important to evaluate the urine output. Placement of a urinary catheter is useful in evaluating neonates with oliguria/anuria as the catheter bypasses the urethral/bladder outlet obstruction (eg, posterior urethral valves in boys) and also provides an accurate estimate of urine output. Initial evaluation in an infant with acute renal failure should include a detailed history and physical examination. The obstetric history should focus on presence or absence of oligohydramnios, polyhydramnios, renal anomalies on antenatal ultrasonography, drug exposure, and family history of renal failure. Physical examination should evaluate genitalia, abdomen (flank mass or palpable bladder), and signs of oligohydramnios/Potter sequence. Initial laboratory evaluation will include electrolytes, serum urea nitrogen, creatinine, complete blood cell count, and urinalysis. Renal ultrasonography allows diagnosis of congenital anomalies of the kidney and urinary tract, urinary obstruction (hydronephrosis, hydroureter, enlarged bladder), or abnormal renal blood flow (arterial or venous) as the underlying etiology for acute renal failure. In the neonatal period, asphyxia, hypovolemia, sepsis, and vascular thrombosis are risk factors for acute kidney injury. Renal vein thrombosis is the most common cause of noncatheter associated thrombosis in the newborn and is the most likely cause of the findings in the newborn described in this vignette. Prematurity, perinatal asphyxia, shock, dehydration, sepsis, polycythemia, cyanotic congenital heart disease, and maternal diabetes have all been associated with an increased risk for renal vein thrombosis. Flank mass, thrombocytopenia, and hematuria (as present in this patient) are the classic features associated with renal vein thrombosis. Renal vein thrombosis may also be associated with elevated blood pressure, laboratory features of disseminated intravascular coagulation, and leukocytosis. Ultrasonography of the kidney is the imaging modality of choice for diagnosing renal vein thrombosis in a newborn. Color Doppler examination on renal ultrasonography will show absent intrarenal and renal venous flow in the early stages of thrombosis. Renal dysplasia is one of the disorders of renal development categorized under the broader category of congenital anomalies of the kidney and urinary tract. Congenital anomalies of the kidney and urinary tract and and cystic kidney diseases (nonglomerular) account for nearly 60% of pediatric chronic kidney disease. Patients with congenital anomalies of the kidney and urinary tract may develop acute renal failure in the presence of severe bilateral hypoplasia or dysplasia, risk factors of neonatal acute renal failure (perinatal asphyxia, hypovolemia, sepsis, and vascular thrombosis), or urinary obstruction. Dysplastic kidneys are usually small because of the reduced number of nephrons, resulting in renal hypodysplasia. Renal dysplasia is often diagnosed during routine antenatal ultrasonography screening or postnatal ultrasonography performed in a dysmorphic infant. Renal dysplasia on ultrasonography is characterized by increased echogenicity, poor corticomedullary differentiation, and parenchymal cysts. Neonates with oligohydramnios and bilateral dysplasia are more likely to be identified earlier. Patients with unilateral renal dysplasia with a normal contralateral kidney showing compensatory growth have excellent outcomes with decreased risk for chronic kidney disease. This contrasts to increased risk for chronic kidney disease in patients with suboptimal compensatory hypertrophy of the contralateral kidney. Chronic kidney disease in such patients may lead to elevated blood pressure, growth retardation (height less than the fifth percentile), and pallor. Tubulointerstitial injury associated with congenital anomalies of the kidney and urinary tract leads to reduced urinary concentration (acquired nephrogenic diabetes insipidus). Blood pressure, urinalysis results, and serum creatinine levels should be initially monitored yearly and subsequently monitored more frequently depending on the stage of chronic kidney disease. Multicystic dysplastic kidney is suspected based on renal abnormalities detected on antenatal ultrasonography or in neonates with an abdominal mass detected by physical examination. Classic findings on renal ultrasonography include multiple noncommunicating cysts with intervening dysplastic renal tissue. The contralateral normal kidney has increased risk for congenital renal anomalies such as vesicoureteral reflux. Posterior urethral valves are identified by antenatal ultrasonography in most cases. Older boys may develop urinary tract infections or voiding dysfunction (urinary frequency, daytime and nocturnal enuresis, and poor urinary stream). This condition would lead to pulmonary hypoplasia because normal amniotic fluid levels between 16 and 28 weeks of gestation are required for normal lung development. Congenital ureteropelvic junction obstruction is most commonly diagnosed upon postnatal evaluation of antenatal hydronephrosis detected on maternal ultrasonography screening. Other less common presentations include urinary tract infection, hematuria, or failure to thrive. Ureteropelvic junction obstruction in older children presents with episodes of flank or abdominal pain (Dietl crisis) accompanied by nausea and vomiting. Children may also rarely exhibit renal injury to the enlarged obstructed kidney after minor trauma, hematuria, renal calculi, or hypertension. It is important to perform ultrasonography during episodes of acute pain because the ultrasonography results may be normal once the pain subsides.
Diseases
- Lung cancer
- Diabetes insipidus, nephrogenic, dominant type
- Arachindonic acid, absence of
- Maroteaux Fonfria syndrome
- Muscle-eye-brain syndrome
- Tuberculosis, pulmonary
- Ganglioglioma
- Adenomelablastoma
- Noma
Discount 200 mg lamotrigine with visa
There is probably 3 or 4% of the population [that] has psoriasis xerostomia medications side effects purchase generic lamotrigine from india, but significant numbers of those have mild disease and do not require biologics. For psoriasis, there are other treatment options in the beginning, but psoriatic arthritis patients usually also suffer from a rheumatic disease, and in those cases the new products are more likely to be used if what is used in the first line proves not to be as effective. In terms of treatment costs, there are fewer patients treated for more money with psoriatic arthritis. What concerns me is the launch of new drugs, which have to be incorporated somehow and the costs are high. Well, the size of the costs is a concern but we have also found that the use of these products has increased. Consequently, many payers and physicians would welcome a reduction in the high prices of biologics in order to enable greater patient access and control spend. Generating pressure to reduce prices also offers payers an opportunity to control the budget impact of biologics, as controlling spend is unlikely to happen by decreasing utilization, especially given the imminent launches of new pipeline biologics. Payers and physicians alike see price reductions as the most plausible way of controlling costs and expanding patient coverage. Datamonitor Healthcare expects that payers will instate more access control strategies to ensure that patients are treated with the least expensive options first, and to leverage the entry of biosimilars to further reduce treatment costs. Manufacturers wanting to remain competitive will need to reduce prices or offer discounts for biologic products to maintain share in an increasingly saturated market. The decision was the result of head-to-head clinical trials demonstrating superior efficacy to both Enbrel and Stelara. Cosentyx also had a more rapid onset of action and greater efficacy in all endpoints in the study up to week 16. It could be a first line even, also before traditional therapy, ie biologic used in first line in absolute in some psoriasis [cases] if particularly aggressive. At the clinic we also used it for some really difficult indications and it works very well for those as well. Traditional first-line therapies are considerably less expensive than biologics and payers do not consider the first-line use of Cosentyx to be a good use of healthcare resources. Datamonitor Healthcare does not expect payers to allow the use of Cosentyx in place of methotrexate or light therapy unless there are severe extenuating circumstances. So the wording is that outside these indications the [service medical rendu] is insufficient to be funded [] For example the reimbursement of Cosentyx published in October 2015 needs the failure [of] the two other treatments, while the license says it can be used as soon as a systemic treatment is needed. When there is a failure of a biologic we then rotate [] I cant imagine [Cosentyx] will replace cyclosporine or Methotrexate in the short term in France. It cannot be first line and also if it were the case, I have the budget to respect and I could not, the hospital will go [to] bankruptcy. The exception is in very severe patients, where physicians tend to use more efficacious options sooner. Datamonitor Healthcare expects that most physicians are likely to prescribe Cosentyx conservatively due to the absence of long-term safety and efficacy results, which will result in slow initial market uptake. It seems to be more expensive than ustekinumab, theoretically, and safer, but I cannot say more, because I have not tried it. Payers report that aside from an absence of real-world safety and efficacy data, a combination of expected high price and unfavorable contract arrangements will prevent Cosentyx from being positioned as a first-line biologic in the near term. Most payers conduct contracts and tenders based on the drug and not on separate indications. As Cosentyx has only received approval in psoriasis and psoriatic arthritis, contracting for the drug may mean more unfavorable negotiating terms for large-volume market leaders like Enbrel and Humira. It remains to be seen, however, if payers are likely to place Cosentyx prior to Stelara without competitive discounting. I think probably it is very useful in psoriasis and they did their homework by doing head-to-head trials. The bad news for them is they are running into the contracting issue and it is hard to break into a preferred status. Well, it is yet to be assessed, but at the moment the patients who are on it are those who have failed first or second line. Because of what I have read about it and its efficacy/safety/cost profile, which is similar to Stelara. Unless when it comes to negotiations with the lab, although I think it unlikely, there is a shared risk arrangement for use at first line. As soon as it has a price I think Cosentyx will become the first line for psoriasis in France. It would be silly to prescribe a product that is less effective, unless there is a contraindication to this one. Cosentyx is likely to face similar problems as Stelara in displacing drugs that have long-term familiarity among physicians and patients. I would prescribe it after Stelara, because with Stelara I have much more personal experience. But the same happened with Stelara at first, [in] that it was not prescribed in early lines. I dont know, as current molecules are already active compared to 10 years ago when we didnt have anything. Now we bring a faster onset and more responders, but I dont think it will change things fundamentally. Without additional head-to head data against Cosentyx, it will be difficult for Taltz to gain premium or favorable positioning in the therapeutic pathway, with most payers and physicians viewing the drug as a Cosentyx me-too. In this scenario, both French and German physicians may be discouraged to use Taltz in their practice due to the unfavorable assessments. Datamonitor Healthcare expects that discounts offered to national, regional, or local payers in these markets could help Eli Lilly to attract market share away from Cosentyx. This is very similar to secukinumab in terms of the skin and since this has a similar mechanism of action that makes sense. It would be difficult to justify having two of the same if they are both expensive. For a patient with only psoriasis there is a better response and probably fewer side effects. There are different features, maybe it is a bit more effective even, it is clear it is a duplicate. While some physicians consider the oral small molecule to be suitable for patients seeking a treatment after failure with first-line agents such as methotrexate, payers perceive its price as excessive. Otezla is priced at around 30% discount to biologics but still substantially above methotrexate, and given that it is a small molecule, many payers consider it overpriced. The Spanish Agency of Medicines and Medical Devices (Agencia Espanola de Medicamentos y Productos Sanitarios) recommended Otezla for use in milder patients who have failed systemic therapies. If I can say, in [the] case of Otezla there are concerns to the Ministry because it is not so effective. Why do I have to approve a drug excluding 30% of patients, costing 10,000/year, when I have another treating 99% of patients at 13,000/year For patients who tolerate it and doctors who want to use it, it will be positioned before the biologics. For efficacy it doesnt have any added value as we have many effective treatments [] [Otezla is] inferior, very clearly inferior [to other biologic agents]. But maybe it can fill the gap for mild to moderate psoriasis [patients] that are not treated systemically but fail with local treatments. And as it is cheaper than biologics it could delay the prescription of these biologics and save the health system money. It is very safe [] It is not a biologic; it is a small molecule product, so even though it is less expensive than the biologics, it is markedly overpriced for what it is. I may be wrong, but certainly based on our experience, it has not been a highly used drug. Further, physicians are not likely to prescribe new drugs over more established candidates unless superior efficacy has been demonstrated, as they tend to be conservative in prescribing new medicines without long-term safety data. However, head-to-head trials themselves are often impossible to conduct for competitors within the same class as they are usually launched near or at the same time. Datamonitor Healthcare expects that manufacturers will need to discount products that do not have head-to-head trial data upon launch to promote uptake. To maintain competitiveness and favorable formulary positioning, however, manufacturers need to conduct post-marketing follow-up trials establishing superior efficacy against gold-standard comparators. Because they will give us safety and efficacy data for biological treatments, so at least we will be advancing in this area, with this subgroup of patients who need a biological treatment.
Order lamotrigine 200mg fast delivery
Clinically treatment ulcer purchase discount lamotrigine line, nail disease has many presentations depending on Results of Article Review the location of the inflammatory process. Nail pitting (the most Although data are limited and placebo-controlled trials rare, there common finding in nail psoriasis), nail dystrophy, and leukonychia are data to support the efficacy of topical cyclosporine, topical ta are due to nail matrix involvement. Nail bed psoriasis is character crolimus, clobetasol propionate nail lacquer, calcipotriol, a combi ized by onycholysis, oil drop patches, subungual hyperkeratosis, nation of calcipotriol and betamethasone dipropionate, tazaro and splinter hemorrhages. No previous therapy has are poor penetration of topical therapy into the nail and surround been used. Because many of the treatments most commonly tralesionalcorticosteroidswererecommended. Systemicandbio used to treat psoriasis do not have published, randomized, logic treatments were not recommended for this patient sce double-blind, placebo-controlled trials addressing nail disease, the nario. Patients with psoriasis limited to the nails for whom topical informed decision regarding the best treatment for a patient with therapyhasfailed. TopicalandProceduralInterventionsinNailPsoriasis Trial Patients, Treatment Evidencea Type Duration No. Repeated injections into 109 nails resulted in 80% treatment success jamadermatology. TopicalandProceduralInterventionsinNailPsoriasis(continued) Trial Patients, Treatment Evidencea Type Duration No. OralSystemicsintheTreatmentofNailPsoriasis Trial Duration, Patients, Treatment Evidencea Type wk No. Intralesional injection of corticosteroids is an accepted clinical the board recommended adalimumab, etanercept, and treatment for localized nail psoriasis and is recommended here ustekinumabwithhighenthusiasm;methotrexate,acitretin,in for patients with psoriasis limited to the nails. Techniques vary but disease on 8% of their body surface area, a history of dactylitis generally involve injection of triamcinolone acetonide, 0. Adverse effects from intralesional fliximab, methotrexate, apremilast, and golimumab. BiologicsintheTreatmentofNailPsoriasis Duration, Patients, Treatment Evidencea Trial Type wk No. BiologicsintheTreatmentofNailPsoriasis(continued) Duration, Patients, Treatment Evidencea Trial Type wk No. Theremaybedif of-life measures validated in onychomycosis and applied these to ferential effects of treatment on these 2 components of nail psoria psoriasis. Inacomparisonofmethotrexateandcyclosporine,methotrexate psoriasis quality of life scale, has been published. There are limited data to evaluate or infliximab, there was some indication that nail bed disease may im support the use of combination therapy in nail psoriasis. Improvements in nail psoriasis often lag behind the improve Conclusions ments in skin and joint disease. Fingernails grow at a rate of 3 to 4 mm/mo;thus,ittakes5to7monthsforanailtogrowfromthema Nail psoriasis poses a significant burden to our patients with pso trix to the distal fingertip. Clinicaldataarelimitedinnailpsoriasis,andclini ment before 12 weeks, and several studies with etanercept, inflixi caloutcomesarenotstandardized. Thus,comparisonamongtreat mab, and ustekinumab demonstrate continued improvement be ment options is virtually impossible based on the current litera yond 6 months. For patients with disease limited to the nails, high-potency One of the problems in reviewing data on nail psoriasis is the topical corticosteroids with or without calcipotriol are initial op lack of consistent outcome reporting among the studies. The recommended dose is 160 mg (two 80 mg injections) at Week 0, followed by 80 mg at Weeks 2, 4, 6, 8, 10, and 12, then 80 mg every 4 weeks. The recommended dose in pediatric patients from 6 to less than 18 years of age with moderate-to-severe plaque psoriasis is based on the following weight categories. For psoriatic arthritis patients with coexistent moderate-to-severe plaque psoriasis, use the dosing regimen for adult plaque psoriasis [see Dosage and Administration (2. Do not use if the liquid contains visible particles, is discolored or cloudy (other than clear and colorless to slightly yellow). Administer each injection at a different anatomic location (such as upper arms, thighs or any quadrant of abdomen) than the previous injection, and not into areas where the skin is tender, bruised, erythematous, indurated or 4 affected by psoriasis. A similar increase in risk of infection was seen in placebo-controlled trials in patients with pediatric psoriasis, psoriatic arthritis, ankylosing spondylitis, and non-radiographic axial spondyloarthritis [see Adverse Reactions (6. Specific Adverse Drug Reactions: Injection Site Reactions 6 the most frequent injection site reactions were erythema and pain. In the 12-week, placebo-controlled period, neutropenia Grade 3 (<1,000 cells/mm) occurred in 0. Active Comparator Trials In the two clinical trials that included an active comparator, the rate of serious adverse events during weeks zero to twelve was 0. The assay to test for neutralizing antibodies has limitations detecting neutralizing antibodies in the presence of ixekizumab; therefore, the incidence of neutralizing antibodies development could be underestimated. The clinical effects of antibodies to ixekizumab are dependent on the antibody titer; higher antibody titers were associated with decreasing drug concentration and clinical response. Neutralizing antibodies were associated with reduced drug concentrations and loss of efficacy. In pediatric psoriasis subjects treated with ixekizumab at the recommended dosing regimen up to 12 weeks, 21 subjects (18%) developed anti-drug antibodies, 5 subjects (4%) had confirmed neutralizing antibodies associated with low drug concentrations. No conclusive evidence could be obtained on the potential association of neutralizing antibodies and clinical response and/or adverse events due to small number of pediatric subjects in the study. Immune system disorders: anaphylaxis [see Contraindications (4) and Warnings and Precautions (5. Data Animal Data An embryofetal development study was conducted in cynomolgus monkeys administered ixekizumab. Neonatal deaths occurred in the offspring of two monkeys administered ixekizumab at 1. These neonatal deaths were attributed to early delivery, trauma, or congenital defect. No ixekizumab-related effects on functional or immunological development were observed in the infants from birth through 6 months of age. Although no differences in safety or efficacy were observed between older and younger subjects, the number of subjects aged 65 and over is not sufficient to determine whether they respond differently from younger subjects [see Clinical Pharmacology (12. Ixekizumab is comprised of two identical light chain polypeptides of 219 amino acids each and two identical heavy chain polypeptides of 445 amino acids each, and has a molecular weight of 146,158 Daltons for the protein backbone of the molecule. The prefilled autoinjector and prefilled syringe each contain a 1 mL glass syringe with a fixed 27 gauge inch needle. Steady-state concentrations were achieved approximately 10 weeks after switching from the 80 mg every 2 weeks dosing regimen to the 80 mg every 4 weeks dosing regimen at Week 12. In studies of subjects with plaque psoriasis, ixekizumab bioavailability ranged from 60% to 81% following subcutaneous injection. Administration of ixekizumab via injection in the thigh achieved a higher bioavailability relative to that achieved using other injection sites including the arm and abdomen. As a humanized IgG4 monoclonal antibody ixekizumab is expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous IgG. Weight Ixekizumab clearance and volume of distribution increase as body weight increases. Dose Linearity Ixekizumab exhibited dose-proportional pharmacokinetics in subjects with plaque psoriasis over a dose range from 5 mg (not the recommended dose) to 160 mg following subcutaneous administration. Specific Populations Age: Geriatric Population Population pharmacokinetic analysis indicated that age did not significantly influence the clearance of ixekizumab in adult subjects with plaque psoriasis. Subjects who are 65 years or older had a similar ixekizumab clearance as compared to subjects less than 65 years old. Pediatric Population Pediatric psoriasis subjects (6 to less than 18 years of age) were administered ixekizumab at the recommended pediatric dosing regimen for 12 weeks. Renal or Hepatic Impairment No formal trial of the effect of hepatic or renal impairment on the pharmacokinetics of ixekizumab was conducted. The relevance of experimental findings in mouse models for malignancy risk in humans is unknown. In the two active comparator trials (Trials 2 and 3), subjects were also randomized to receive U. Of all subjects, 44% had received prior phototherapy, 49% had received prior conventional systemic therapy, and 26% had received prior biologic therapy for the treatment of psoriasis.
Buy lamotrigine 100 mg free shipping
Without vitamin A substitution symptoms 8 days after iui generic lamotrigine 100 mg with visa, the disorder will lead to blindness within a few years. Onset is abrupt and initially unilateral with inflamma tion of the second eye within one week. Etiology: Causes of conjunctivitis may be fall into two broad categories: O Infectious (see. Symptoms: Typical symptoms exhibited by all patients include reddened eyes and sticky eyelids in the morning due to increased secretion. Any con junctivitis also causes swelling of the eyelid, which will appear partially closed (pseudoptosis). Foreign-body sensation, a sensation of pressure, and a burning sensation are usually present, although these symptoms may vary between individual patients. Photophobia and lacrimation (epiphora) may also be present but can vary considerably. Simultaneous presence of blepharospasm suggests cor neal involvement (keratoconjunctivitis). This makes it all the more important to note certain characteristic findings that permit an accurate diagnosis, such as the type of exudation, con junctival findings, or swollen preauricular lymph nodes (Table 4. The conjuncti val injection is due to increased filling of the conjunctival blood vessels, which occurs most prominently in the conjunctival fornices. However, the visibility of the hyperemic vessels and their location and size are important criteria for differential diag nosis. One can also distinguish conjunctivitis from other disorders such as scleritis or keratitis according to the injection. O Conjunctival injection (bright red, clearly visible distended vessels that move with the conjunctiva, decreasing toward the limbus;. O Pericorneal injection (superficial vessels, circular or circumscribed in the vicinity of the limbus). O Ciliary injection (not clearly discernible, brightly colored nonmobile ves sels in the episclera near the limbus). The quantity and nature of the exudate (mucoid, purulent, watery, ropy, or bloody) depend on the etiology (see Table 4. This may range from the absence of any conjunctival thickening to a white glassy edema and swelling of the conjunctiva projecting from the palpebral fissure (chemosis this severe occurs with bacterial and allergic conjunctivitis). Illacrimation is usually reflex lacrimation in reaction to a conjunc tival or corneal foreign body or toxic irritation. Lymphocytes in the palpebral and bulbar conjunctiva accumulate in punctate masses of lymph tissue cells that have a granular appearance. Papillae appear as polygonal cobblestone conjunctival projections with a central network of finely branching vessels. They form from necrotic epithelial tissue and either can be easily removed without bleeding (pseudomem branes) or leave behind a bleeding surface when they are removed (mem branes; Figs. Lymph from the eye region drains through the preauricular and submandibular lymph nodes. Swollen lymph nodes are an important and frequently encountered diagnostic sign of viral conjunctivitis. The combination and severity of individual symptoms usually provide essential information that helps to identify the respective presenting form of conjunctivitis. These are inflamed nodes of conjunctival stroma with circum scribed areas of reddening and vascular injection. They can occur with sys temic disorders such as tuberculosis or sarcoidosis or may be exogenous, such as postoperative suture granulomas or other foreign-body granulomas. Granulomas are not a sign of conjunctivitis in the strict sense and for that reason have not been included as symptoms or findings in Table 4. The nature and extent of vascular injections, discharge, conjunctival swelling, etc. This is performed to examine the upper and lower eyelids for the presence of follicles, papillae, membranes, and foreign bodies. If the diagnosis is uncertain or what appears to be bacterial conjunctivitis does not respond to antibiotics, a conjunctival smear. Cotton swabs with sterile shipping tubes are commercially available; special test kits with specific cultures are available for detecting chlamydiae. An antibiotic that is not effective in treating what appears to be bacte rial conjunctivitis should be discontinued. Microbiological examination to iden tify the pathogen is indicated for any conjunctivitis in children. This is used to detect chlamydiae in particular and to more clearly identify the pathogen in general. Cyto logic findings provide important information about the etiology of the con junctivitis. O bacterial conjunctivitis: granulocytes with polymorphous nuclei and bac teria; O viral conjunctivitis: lymphocytes and monocytes; O chlamydial conjunctivitis (special form of bacterial conjunctivitis): com posite findings of lymphocytes, plasma cells, and leukocytes; characteris tic intracytoplasmic inclusion bodies in epithelial cells may also be present (see. O allergic conjunctivitis: findings primarily include eosinophilic granulo cytes and lymphocytes; O mycotic conjunctivitis (very rare): the Giemsa or Gram stain will reveal the hyphae. The lower lacrimal system should always be irrigated in the presence of inflammation that recurs or resists treatment to verify or exclude that it is the source of the inflammation. Inflammation usually occurs as a result of infection from direct contact with pathogens (such as from a finger, towel, or swimming pool) but also from complicating factors (such as a compromised immune system or injury). Etiology: Staphylococcus, streptococcus, and pneumococcus infections are most common in temperate countries. Diagnostic considerations: Bacterial conjunctivitis can usually be reliably diagnosed from the presence of typical symptoms. Laboratory tests (conjunc tival smear) are usually only necessary when the conjunctivitis fails to respond to antibiotic treatment. Treatment: Bacterial conjunctivitis usually responds very well to antibiotic treatment. A wide range of well tolerated, highly effective antibiotic agents is available today. Most of these are supplied as ointments (which are longer acting and suitable for overnight therapy) and as eyedrops for topical therapy. Substances include gentamicin, tobramycin, Aureomycin, chloramphenicol,1 neomycin, polymyxin B in combination with bacitracin and neomycin, Ter ramycin, kanamycin, fusidic acid, ofloxacin, and acidamphenicol. These include medications such as gentamicin and dexamethasone; neomycin, polymyxin B, and dexamethasone; or tetracycline, polymyxin B, and hydro cortisone. In severe, uncertain, or persistent cases requiring microbiological exami nation to identify the pathogen, treatment with broad-spectrum antibiotics or topical antibiotic combination preparations that cover the full range of Gram-positive and Gram-negative pathogens should begin immediately. This method is necessary because microbiological identification of the pathogen and resistance testing of the antibiotic are not always successful and may require several days. In the presence of severe, uncertain, or persistent conjunctivitis, treat ment with broad-spectrum antibiotics or topical antibiotic combination preparations should be initiated immediately, even before the labora tory results are available. Clinical course and prognosis: Bacterial conjunctivitis usually responds well to antibiotic treatment and remits within a few days. In the newborn (see neonatal conjunctivitis), this occurs at birth through the cervical secretion. In adults, it is primarily transmitted during sexual intercourse, and rarely from infection in poorly chlorinated swimming pools. Symptoms: the eyes are only moderately red and slightly sticky from viscous discharge. Diagnostic considerations: Tarsal follicles are observed typically on the upper and lower eyelids, and pannus will be seen to spread across the limbus of the cornea. As this is an oculogenital infection, it is essential to determine whether the mother has any history of vaginitis, cervicitis, or urethritis if there is clinical suspicion of neonatal infection.
Discount 200 mg lamotrigine fast delivery
Ocular Regenerative Medicine and Immunology medicine 4h2 pill purchase lamotrigine online, Ophthalmology and Vision Science, Washington 2 1 Yappert. Ophthalmology, University of Louisville, Seoul Artifcial Eye Center, Seoul National University School of Medicine, St. Chae University of Science and Technology, Pohang, 5 1 2 7 regulators of fuid hydration on the eye. The Ohio meibum according to dry eye type classifed by Ophthalmology and Anatomy/Cell Biology,Kresge State University College of Optometry, Columbus, 1 2 tear flm interferometer. The School of Optometry, Medicine, University of Southern California, ophthalmic solutions stabilize tear flm Korea (the Republic of) Lacritin, the Shed Form of Lacritin Co-Receptor Dubald, A. Yuriko University, Gwangju, Korea (the Republic of) 1, 2 3 2 4 Intraductal Probing for the Treatment of Ban, N. A induced Dry Eye Disease in Rabbits using Nantan, Kyoto, Japan; 2Ophthalmlogy, Kyoto Orlin1, M. Yukihisa School of Pharmacy, Chapman University, Irvine, Adiponectin-Derived Short Peptides and Takada, O. Ophthalmology, Yonsei University Wonju 3 Ophthalmology, Chosun University Hospital, Islands (U. Chang Gung Memorial Hospital, the First Affliated Hospital of Nanchang Universi, enhances the ocular mucin secretion in the Taoyuan, Taiwan Nanchang, China desiccation stress-mediated dry eye disease. Meri Ophthalmology, Oslo University Hospital, Oslo, Ophthalmology, Massachusetts Eye and Ear Vattulainen, T. Mary Ann Conservation Mechanisms in Cultured Sheets Stem Cell Defciency and Neovascularization. Low Vision Group / Visual Psychophysics/ cells and organ-cultured diabetic corneas for 1, 2 3 Bagherinia, A. Department Ophthalmology, University of Illinois at Chicago, Victoria, Australia; 2Bionic Eye Technologies, Inc. Huiyu Biosciences, Latrobe University, Bundoora, Victoria, Australia; 5Department of Ophthalmology, cell function in healthy and diabetic cornea. Department of Ophthalmology and Visual 1 1 University of Bonn, Bonn, Germany; 6L V Prasad Aleksandra Leszczynska, M. Stout, 3 1 1 1 1, 3 Ophthalmology and Visual Sciences, University of Department of Electrical and Electronic M. Choi, 8 1 1 1 4 Alberta, Edmonton, Alberta, Canada; Department Engineering, Jerusalem College of Technology, L. Hirota, 4 of Ophthalmology & Visual Sciences, University 2 2 3 1 Institut de la Vision, Sorbornne Universites, Paris, 12 H. Trainees, students and junior faculty will beneft from this unique opportunity to network and gain valuable information from those who have been in your shoes! This very popular program offers informal discussions over breakfast on a wide range of topics to provide personal guidance, insight and skills to help you advance your career! Topics will focus on professional development, career guidance, and best practices of interest to basic and clinical trainees and clinician-scientists. A number of the roundtable topics will be specifcally tailored to the needs of clinician-scientists. Lorie St-Amour, University of British Columbia, Vancouver, British Columbia, Canada; 6Population Health, Singapore J. Science, Friedrich-Alexander-Universitat Erlangen University, Adelaide, South Australia, Australia; Afshari. Netherlands; Ophthalmology, Radboud University and Informatics, University of Pennsylvania, 1 2 1 1 5 Bonfglio, M. Pavlou1, Seng Hospital, Singapore, Singapore; 2Department Western Australia, Perth, Western Australia, I. Osamah Saeedi1, (Centre for Vision Research), Westmead Hospital) Photoreceptor Survival in Mouse Models of B. Tsai1, and Westmead Millennium Institute, Westmead, 1 3 1 New South Wales, Australia; 7Melbourne School Retinitis Pigmentosa. Cardiff, England, United Kingdom; 2School of Biochemistry/Molecular Biology Gesualdo3, S. Connectomics, Korea Institute of Science and and Division of Preventive Ophthalmology, Guy. Bonilha complement C3 activation in models of macular Assitance Publique Hopitaux de Paris, Paris, France 1, 2 1, 3 degeneration. Shuster2, Sciences, University of Wisconsin-Madison, Department of Regenerative Medicine, Tongji Eye E. Mohamed1, 2, 1Ophthalmology and Vision Science, University potential role of age-related synuclein in the 1 S. Franziskus Hospital Munster, Munster, (the Republic of); 2 University of Ulsan College of Stepicheva1, S. Germany; 5Faculty of Medicine, University of 3 2 2, 1 1 Medicine, Ulsan, Korea (the Republic of); College S. Mukherjee, Ophthalmology, University of Pittsburgh School of Reproductive Medicine and Andrology, Wesfalian N. Aleksander Ireland, Belfast, Northern Ireland, United Institute, the Johns Hopkins University School of Tworak1, C. Department of Clinical Neuroscience, Neuroscience, Cell Biology & Anatomy, the Zhang, A. Department of Medicine Huddinge, Center for retinal pigment epithelium in the mouse. State Key Laboratory of Institutet, Stockholm, Sweden; Department of 2 2 2 1 Chrenek, J. Pham, Astronomy, Texas A&M University, College Station, Yamaguchi, Japan; 2Kyushu University School of 4 Z. Ishikawa, Biology, University of Iceland, Reykjavik, Iceland; 2, 3 1 4 mitochondrial dynamics in the retinal pigment D. Ophthalmology, Doheny Eye Clinical Neurosciences, St Erik Eye Hospital, 1 1, 2 2 epithelium. Epithelial Cells: An Alternative Metabolic Semmelweis University, Budapest, Hungary 1 1 1 Wils, J. Netherlands; Institute of Cellular and integrative 1 1 1 1 Mitochondria Depletion and Rescue by Platelet Schulz, I. Biochemistry, University Astrophysics, Optics and Electronics, Tonantzintla, Cepko1, 2, D.
Hornseed (Ergot). Lamotrigine.
- Are there any interactions with medications?
- Reducing bleeding in childbirth, assisting delivery, menstrual pain, and other conditions.
- How does Ergot work?
- What is Ergot?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96442
Order 50 mg lamotrigine with amex
Retinal detachment (simple) is always due to break in the retina through which fluid seeps in symptoms in dogs order lamotrigine 50mg otc, raising the retina from its bed. Complicated cataract (posterior cortical) is due to the disturbance to the nutrition of the lens. In pathological myopia, the patient should avoid an occupation where close work is necessary. In low degree of myopia, spectacles are rarely required for near work (after the Errors of Refraction 51 Temporal and supertractional nasal crescent presbyopic age). It should be undercorrected to avoid very bright and clear retinal images which are uncomfortable. Regular Astigmatism Normally cornea is flatter from side to side (horizontal meridian) perhaps because of the pressure of the eyelids. Regular astigmatism is present when the two principal meridians are at right angles. Thus, the more curved meridian will have more convergent power than the less curved. Retinal plane at A Compound hypermetropic astigmatism Both the foci are behind the retina. Partial or full thickness keratoplasty may be done depending on the depth of opacity as a last resort. When there are symptoms, suitable cylindrical lenses are prescribed for constant use. Mixed astigmatism has good prognosis as circle of least diffusion falls upon or near the retina. Aphakic eye Correction with convex lens Symptom There is gross dimness of vision because of acquired high hypermetropia. A linear semicircular corneo-scleral scar mark is seen in the upper half of cornea. There is greater refraction at the periphery of spherical lens than near the centre. Contact Lens Advantages There is minimum retinal image magnification, therefore it is useful in unilateral aphakia. Diplopia or seeing double objects may be present in severe cases and unilateral aphakia. It is treated by prescribing suitable correcting lenses for refractive difference of up to 2-3 D. The vision improves if the book is held further away from the ordinary reading distance, i. Presbyopia is treated by prescribing suitable convex spherical lenses for near work. This correction for near work is added to the correcting lenses for the distant vision. Mydriatics in Refraction the pupil is dilated by a suitable mydriatic depending on the age of patient. Streak retinoscopy Neutralisation When the shadow moves with the mirror, progressively stronger convex lenses are put in the trial frame until, i. Similarly, when the shadow moves against the mirror, progressively stronger concave lenses are put in the trial frame until the point of reversal is reached. The correction for near vision by convex spherical lenses is made over 40 years of age usually. When the lens is moved in front of the eye, the objects move in the opposite direction. When the lens is moved in front of the eye, the objects move in the same direction ii. The axis of a cylindrical lens is parallel to that of the cylinder of which it is a part. When the lens is moved in the direction of the axis, there is no movement of the objects. Contact Lenses Principle Contact lens alters the vergence power of the anterior surface of the eye. Cosmetic It improves the cosmetic appearance specially in young marriageable girls. Each surgeon may have a preference for a particular procedure depending on economic reasons, availability factor or his own personal satisfaction with the end results. The aim of astigmatic keratotomy is to flatten the more curved meridian by asymmetrical incisional surgery. To achieve this various considerations are kept in mind such as the number and position of the transverse incisions.
Effective lamotrigine 50 mg
Do not sign this consent and do not take isotretinoin if there is anything that you do not understand symptoms 9 days past iui discount lamotrigine 200 mg free shipping. I understand that there is a very high chance that my unborn baby could have severe birth defects if I am pregnant or become pregnant while taking isotretinoin. I understand that I must not get pregnant 1 month before, during the entire time of my treatment, and for 1 month after the end of my treatment with isotretinoin. I understand that I must avoid sexual intercourse completely, or I must use 2 separate, effective forms of birth control (contraception) at the same time. The only exceptions are if I have had surgery to remove the uterus (a hysterectomy) or both of my ovaries (bilateral oophorectomy), or my doctor has medically confirmed that I am post-menopausal. I understand that hormonal birth control products are among the most effective forms of birth control. That is why I must use 2 different birth control methods at the same time, starting 1 month before, during, and for 1 month after stopping therapy every time I have sexual intercourse, even if 1 of the methods I choose is hormonal birth control. I will talk with my doctor about any medicines including herbal products I plan to take during my isotretinoin treatment because hormonal birth control methods may not work if I am taking certain medicines or herbal products. I may receive a free birth control counseling session from a doctor or other family planning expert. My isotretinoin doctor can give me an isotretinoin Patient Referral Form for this free consultation. I must begin using the birth control methods I have chosen as described above at least 1 month before I start taking isotretinoin. I cannot get my first prescription for isotretinoin unless my doctor has told me that I have 2 negative pregnancy test results. The first pregnancy test should be done when my doctor decides to prescribe isotretinoin. The second pregnancy test must be done in a lab during the first 5 days of my menstrual period right before starting isotretinoin therapy treatment, or as instructed by my doctor. I was told about a private counseling line that I may call for more information about birth control. I must stop taking isotretinoin right away and call my doctor if I get pregnant, miss my expected menstrual period, stop using birth control, or have sexual intercourse without using my 2 birth control methods at any time. I must have a negative result from a urine or blood pregnancy test done in a lab repeated each month before I receive another isotretinoin prescription. At least 1 method must be a primary form of birth control, unless I have chosen never to have sexual contact with a male (abstinence), or I have undergone a hysterectomy. I must use 2 forms of birth control for at least 1 month before I start isotretinoin therapy, during therapy, and for 1 month after stopping therapy. I must receive counseling, repeated on a monthly basis, about birth control and behaviors associated with an increased risk of pregnancy. Initial: 34 My doctor has answered all my questions about isotretinoin and I understand that it is my responsibility not to get pregnant 1 month before, during isotretinoin treatment, or for 1 month after I stop taking isotretinoin. Initial: I now authorize my doctor to begin my treatment with isotretinoin. Patient Signature: Date: Parent/Guardian Signature (if under age 18): Date: Please print: Patient Name and Address Telephone I have fully explained to the patient, the nature and purpose of the treatment described above and the risks to female patients of childbearing potential. I have asked the patient if she has any questions regarding her treatment with isotretinoin and have answered those questions to the best of my ability. A parent or guardian of a patient under age 18 must also read and understand each item before signing the agreement. Do not sign this agreement and do not take isotretinoin if there is anything that you do not understand about all the information you have received about using isotretinoin. I understand that there are serious side effects that may happen while I am taking isotretinoin. I understand that some patients, while taking isotretinoin or soon after stopping isotretinoin, have become depressed or developed other serious mental problems. Some patients taking isotretinoin have had thoughts about hurting themselves or putting an end to their own lives (suicidal thoughts). There have been reports of patients on isotretinoin becoming aggressive or violent. No one knows if isotretinoin caused these behaviors or if they would have happened even if the person did not take isotretinoin. Some 36 people have had other signs of depression while taking isotretinoin (see #7 below). Before I start taking isotretinoin, I agree to tell my doctor if I have ever had symptoms of depression (see #7 below), been psychotic, attempted suicide, had any other mental problems, or take medicine for any of these problems. Being psychotic means having a loss of contact with reality, such as hearing voices or seeing things that are not there. Before I start taking isotretinoin, I agree to tell my doctor if, to the best of my knowledge, anyone in my family has ever had symptoms of depression, been psychotic, attempted suicide, or had any other serious mental problems. Once I start taking isotretinoin, I agree to stop using isotretinoin and tell my doctor right away if any of the following signs and symptoms of depression or psychosis happen. I agree to return to see my doctor every month I take isotretinoin to get a new prescription for isotretinoin, to check my progress, and to check for signs of side effects. I will not give blood while taking isotretinoin or for 1 month after I stop taking isotretinoin. I understand that if someone who is pregnant gets my donated blood, her baby may be exposed to isotretinoin and may be born with serious birth defects. Initials: I now allow my doctor to begin my treatment with isotretinoin. Patient Signature: Date: Parent/Guardian Signature (if under age 18): Date: Patient Name (print) Patient Address Telephone (. This information does not take the place of talking with your doctor about your medical condition or your treatment. Birth defects (deformed babies), loss of a baby before birth (miscarriage), death of the baby, and early (premature) births. Female patients who are pregnant or who plan to become pregnant must not take Accutane. If you get pregnant while taking Accutane, stop taking it right away and call your doctor. Some patients taking Accutane have had thoughts about hurting themselves or putting an end to their own lives (suicidal thoughts). Accutane is a medicine taken by mouth to treat the most severe form of acne (nodular acne) that cannot be cleared up by any other acne treatments, including antibiotics. Accutane can cause serious side effects (see What is the most important information I should know about Accutane See the end of this Medication Guide for a complete list of ingredients in Accutane. Tell your doctor about all of the medicines you take including prescription and non-prescription medicines, vitamins and herbal supplements. Accutane and certain other medicines can interact with each other, sometimes causing serious side effects. Tetracycline antibiotics taken with Accutane can increase the chances of getting increased pressure in the brain. These medicines should not be used with Accutane unless your doctor tells you it is okay. Accutane can hurt the tube that connects your mouth to your stomach (esophagus) if it is not swallowed whole. You must talk about effective birth control methods with your doctor or go for a free visit to talk about birth control with another doctor or family planning 42 expert. Your doctor can arrange this free visit, which will be paid for by the company that makes Accutane.
Cheap lamotrigine 100 mg overnight delivery
About 10% of psychiatric patients with pain have rectal medications given before surgery buy lamotrigine 100 mg amex, Relieving Agents perineal, or genital pain. This is usually mentioned as a the onset of action of most drugs is too slow to be of secondary site of pain. Others assume the knee-chest position and then rectal pain is usually associated with severe depressive firmly pull the buttocks apart. There is no accepted or schizophrenic illness but may also be associated with method of preventing or treating this condition. Complications Nausea and sweating and/or fainting may occur during Conversion pain in these patients is usually accompanied an attack. Marital disharmony due to the fear of sexual inter course precipitating an attack has been described. X5 Pathology or Other Contributing Factors Proctalgia is thought by some to occur more commonly in sufferers from irritable bowel symptoms. Severe brief episodic pain, seemingly arising in the rec tum, occurring at irregular intervals. Diagnostic Criteria Episodic pain in the rectal area occurring in otherwise Site well subjects. Proctalgia fugax has been attributed to spasm pain with each bowel movement and can be seen at ano of the sigmoid colon or levator ani. The pain is sudden in onset, without warning, References lasting from several seconds to 20 minutes. Most sufferers have fewer than six irritable bowel, peptic ulcer or inflammatory bowel disease, single episodes per year. Harvey, R, Colonic modality in proctalgia fugax, Lancet, 2 Prevalence (1979) 713-714. For explanatory material on this section and on section D, Spinal and Radicular Pain Syndromes of the Cervical and Thoracic Regions, see pp. Clinical Features Clinical Features Lumbar spinal pain with or without referred pain. Lumbar spinal pain with or without referred pain, asso ciated with pyrexia or other clinical features of infection. Diagnostic Features Radiographic or other imaging evidence of a fracture of Diagnostic Features one of the osseous elements of the lumbar vertebral col A presumptive diagnosis can be made on the basis of an umn. Absolute confirmation relies on histologi Fracture of a Vertebral Body cal and/or bacteriological confirmation using material Code 533. Absolute confirmation relies on Definition obtaining histological evidence by direct or needle bi Lumbar spinal pain associated with a metabolic bone opsy. I (S)(R) Clinical Features Primary Tumor of a Vertebral Body Lumbar spinal pain with or without referred pain. Definition Lumbar spinal pain associated with a congenital verte Clinical Features bral anomaly. Clinical Features Diagnostic Features Lumbar spinal pain with or without referred pain. Imaging or other evidence of arthritis affecting the joints of the lumbar vertebral column. Diagnostic Features Imaging evidence of a congenital vertebral anomaly Schedule of Arthritides affecting the lumbar vertebral column. Although they may be associated with pain, Ankylosing Spondylitis the specificity of this association is unknown. Definition the alternative classification to lumbar spinal pain due Lumbar spinal or radicular pain stemming from a pseu to osteoarthrosis should be lumbar zygapophysial joint darthrosis formed by a transitional vertebra. Consequently, the radiographic whose cause or source cannot be or has not been deter presence of a pseudarthrosis in a patient with spinal pain mined by special investigations. Anomalous Lumbar spinal pain for which no other cause has been lumbosacral articulations and low-back pain: evaluation found or can be attributed. Lumbar spinal pain associated with disease of an ab Patients given this diagnosis could in due course be ac dominal viscus or vessel that reasonably can be inter corded a more definitive diagnosis once appropriate di preted as the source of pain. In some Clinical Features instances, a more definitive diagnosis might be attain Lumbar spinal pain with or without referred pain, to able using currently available techniques, but for logistic gether with features of the disease affecting the viscus or or ethical reasons these may not have been applied. Diagnostic Features Upper Lumbar Spinal Pain of Reliable evidence of the primary disease affecting an Unknown or Uncertain Origin abdominal viscus or vessel. Clinical Features Diagnostic Criteria Spinal pain located in the lower lumbar region. Conjectures may be raised as to the possible origin of this form of pain, such as neuroma formation, deafferen Lumbosacral Spinal Pain of tation, epidural scarring, etc. X7cS Dysfunctional Lumbar spinal pain, with or without referred pain, stemming from a lumbar intervertebral disk. The pathology of internal disk disruption is believed to be due to enzymatic degradation of the internal disk ma Remarks trix. Initially, the degradation is restricted to the nucleus Provocation diskography alone is insufficient to estab pulposus, but eventually it progresses in a centrifugal lish conclusively a diagnosis of discogenic pain because pattern along radial fissures into the anulus fibrosus. If analgesic tion and deaggregation of proteoglycans and diminished diskography is not performed or is possibly false water-binding capacity of the nucleus pulposus. Oth erwise, the diagnosis of discogenic pain cannot be the causes of disk degradation are still speculative but sustained, whereupon an alternative classification must possibly involve disinhibition of proteolytic enzymes be used. X7*S Dysfunctional Local anesthetic blockade of the nerves supplying a tar References get zygapophysial joint may be used as a screening pro Bernard, T. May be due to small fractures not evident on plain radiography or conventional computerized to Vanharanta, H. May be due to osteoarthrosis, but the radiographic pres ence of osteoarthritis is not a sufficient criterion for the diagnosis to be declared. Definition Sprains and other injuries to the capsule of zyga Lumbar spinal pain, with or without referred pain, pophysial joints have been demonstrated at post mortem stemming from one or more of the lumbar zyga and may be the cause of pain in some patients, but these pophysial joints. Diagnostic Criteria Code No criteria have been established whereby zyga pophysial joint pain can be diagnosed on the basis of the Trauma 533. X6aR the condition can be diagnosed only by the use of diag nostic, intraarticular zygapophysial joint blocks. For the References diagnosis to be declared, all of the following criteria Bough, B. Arthrography must demonstrate that any injection of corticosteroid injections into facet joints for chronic low has been made selectively into the target joint, and back pain, New Engl. The response must be validated by Apophyseal injection of local anesthetic as a diagnostic aid in an appropriate control test that excludes false primary low-back pain syndromes, Spine, 6 (1981) 598-605. Definition Lumbar spinal pain stemming from a lesion in a speci fied muscle caused by strain of that muscle beyond its Lumbar Trigger Point Syndrome normal physiological limits. Diagnostic Criteria Clinical Features the following criteria must all be satisfied. Lumbar spinal pain, with or without referred pain, asso ciated with a trigger point in one or more muscles of the 1. Elimination may be achieved by stretching the nous junction, that elicits and inflammatory repair re affected muscle, dry needling the trigger point, or in sponse. Remarks Pathology this nosological entity has been included in recognition Unknown. Trigger points are believed to represent areas of its frequent use in clinical practice, and because of contracted muscle that have failed to relax as a result muscle sprain is readily diagnosed in injuries of the of failure of calcium ions to sequestrate. However, in the context of spinal pain this entity result of the accumulation of algogenic metabolites. Page 183 Remarks with low-back pain, but although it is associated with For the diagnosis to be accorded, the diagnostic criteria back pain a causal relationship between this type of for a trigger point must be fulfilled. In: the Trigger Point Manual, Williams & Wilkins, spasm-pain cycle in spinal disorders, Clin. Lumbar spinal pain ostensibly due to excessive strains imposed on the restraining elements of a single spinal Clinical Features motion segment. Lumbar spinal pain for which there is no other underly ing cause, associated with demonstrable sustained mus Clinical Features cle activity. Lumbar spinal pain, with or without referred pain, that can be aggravated by selectively stressing a particular Diagnostic Features spinal segment. Palpable spasm is usually found at some time, most of ten in the paravertebral muscles. Remarks While there are beliefs in a pain-muscle spasm-pain cy Pathology cle, clinical tests or conventional electromyography have Unknown.
Order 200 mg lamotrigine with amex
German edition published and copyrighted 1998 by Georg Thieme Verlag treatment nail fungus purchase lamotrigine 50 mg free shipping, Stuttgart, Some of the product names, patents, and Germany. Thieme New York, 333 Seventh Avenue this book, including all parts thereof, is New York, N. Definition: the concept behind this book was to organize content and layout according to a uniform structure. This enhances the clarity of the presenta tion and allows the reader to access information quickly. Each chapter has its own header icon, which is shown on every page of the chapter. Figure headings summarize the key information presented in the respective figure, eliminating the need for the reader to read through the entire legend. Epidemiology: In the absence of precise epidemiologic data, the authors state whether the disorder is common or rare wherever possible. Etiology: this section usually combines information about the etiology and pathogenesis of a disorder and in so doing helps to illuminate important rela tionships. Symptoms and diagnostic considerations: these items are usually dis cussed separately. The section on symptoms includes only the phenomena with which the patient presents. How and by which methods the examiner proceeds from these symptoms to a diagnosis is only discussed under diag nostic considerations. These may be facts that one is often required to know for exami nations, or they may be practical tips that are helpful in diagnosing and treating the disorder. Differential diagnosis: Wherever possible, this section discusses not only other possible diagnoses but also important criteria for differentiating the disorder from others. Treatment: this section goes beyond merely documenting all possible ther apeutic options. It also explains which therapeutic measures are advisable and offer a prospect of success. The discussion of medical treatment occa sionally includes dosage information and examples of preparations used. This is done where such information is relevant to cases students will encounter in practice. Prognosis and clinical course: the further development of the book depends in no small measure on your criticism. We are happy to receive any suggestions for improvements as this will help us tailor the next edition to better suit yor needs. Director, Department of Medical Retina and Laser Surgery, University Eye Hospital, Ulm Doris Recker Orthoptist, University Eye Hospital, Ulm C. V Preface When my coworkers and I first took up the task of writing a textbook of ophthalmology that was aimed at medical students but would also be suita ble for interns and ophthalmology residents, we did not know exactly what we were getting ourselves into. We did not merely intend to design a book according to the maxims understand it in medical school, learn it for the examination, and use it during your internship. In an age in which teaching is undergoing evaluation, we felt this was particularly important. In pursuing this admittedly ambitious goal, we were able to draw upon many years of teaching experience. This experience has shaped the educational concept behind this book and manifests itself in details such as the layout, which is characterized by numerous photographs and illustrative drawings. These illustrations make ophthalmology come alive and hopefully will be able to imbue the reader with some of the enthusiasm that the authors themselves have for their specialty. I would like to take this opportunity to offer my heartfelt thanks to my teacher, Prof. Naumann, Erlangen, Germany, for his sugges tions and for the slides from the collection of the Department of Ophthal mology and University Eye Hospital, Erlangen. Peter Wagner for their harmonious cooperation and exceptional initiative in writing this book. Jurgen Luthje and Sabine Bartl of Georg Thieme Verlag, whose professionalism and active and tireless support were a constant source of inspiration to us all. I would again like to thank Markus Voll, Furstenfeldbruck, Germany, for his splendid illustrations. Testing the Potential Resolving Power of the Retina in the Presence of Opacified Optic Media. O Desmarres eyelid retractor and glass rod or sterile cotton swab for eyelid eversion. O Antibiotic eyedrops for first aid treatment of injuries, sterile eye compresses, and a 1cm adhesive bandage for protective bandaging. An ophthalmologist should be consulted following any emergency treatment of eye injuries. Many eye disorders are hereditary or of higher incidence in members of the same family. Examples include refractive errors, stra bismus, cataract, glaucoma, retinal detachment, and retinal dystrophy. As ocular changes may be related to systemic disorders, this possibility must be explored. Conditions affecting the eyes include diabetes mellitus, hypertension, infectious diseases, rheumatic disorders, skin diseases, and surgery. Eye disorders such as corticosteroid-induced glaucoma, corticosteroid-induced cataract, and chloroquine-induced maculopathy can occur as a result of treatment with medications such as steroids, chloroquine, Amiodarone, Myambutol, or chlorpromazine (see table in Appendix). The examiner should inquire about corrective lenses, strabismus or amblyopia, posttraumatic conditions, and surgery or eye inflammation. Does the patient have impaired vision, pain, redness of the eye, or double vision One eye is covered with a piece of paper or the palm of the hand placed lightly over the eye. The fingers should not be used to cover the eye because the patient will be able to see between them. The general practitioner or student can perform an approximate test of visual acuity. The patient is first asked to identify certain visual symbols referredtoasoptotypes(seeFig. These visual symbols are designed so that optotypes of a cer tain size can barely be resolved by the normal eye at a specified distance (this standard distance is specified in meters next to the respective symbol). The sharpness of vision measured is expressed as a fraction: Examining visual acuity. A normal-sighted person would be able to discern the 4 at a distance of 50 meters or 200 feet (standard distance). The ophthalmologist tests visual acuity after determining objective refraction using the integral lens system of a Phoroptor, or a box of individual lenses and an image projector that projects the visual symbols at a defined distance in front of the eye. Visual acuity is automatically calculated from the fixed actual distance and is displayed as a decimal value. Plus lenses (convex lenses) are used for farsightedness (hyperopia or hypermetropia), minus lenses (concave lenses) for nearsightedness (myopia), and cylindrical lenses for astigmatism. If the patient cannot discern the symbols on the eye chart at a distance of 5 meters (20 feet), the examiner shows the patient the chart at a distance of 1 meter or 3 feet (both the ophthalmologist and the general practitioner use eye charts for this examination). If the patient is still unable to discern any symbols, the examiner has the patient count fingers, discern the direction of hand motion, and discern the direction of a point light source. This allows the examiner to diagnose strabismus, paralysis of ocular muscles, and gaze paresis. Evaluating the six cardinal directions of gaze (right, left, upper right, lower right, upper left, lower left) is sufficient when examining paralysis of the one of the six extraocular muscles. The motion impairment of the eye resulting from paralysis of an ocular muscle will be most evident in these positions.