
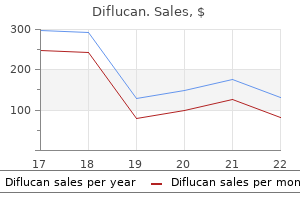
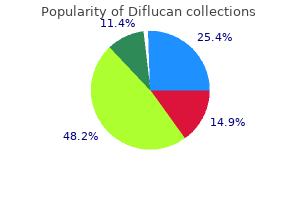
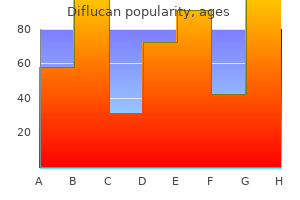
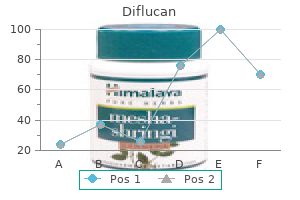
Diflucan
Buy cheap diflucan on-line
Clinical Practice Guideline on the evaluation and follow-up care of living kidney donors antifungal garlic 50 mg diflucan fast delivery. Risks of transplanting kidneys from hepatitis B surface antigen-negative, hepatitis B core antibody-positive donors. Use of renal allografts from donors positive for hepatitis B core antibody confers minimal risk for subsequent development of clinical hepatitis B virus disease. Infection and cancer screening in potential living donors: best practices to protect the donor and recipient. Membranoproliferative glomerulonephritis associated with hepatitis C virus infection. Cytomegalovirus infection after organ transplantation: an update with special emphasis on renal transplantation. Guidelines for the prevention and management of cytomegalovirus disease after solid organ transplantation. Transmission of human herpesvirus 8 infection from renal transplant donors to recipients. Diagnosis and management of tuberculosis in transplant donors: a donor-derived infections consensus conference report. Tuberculosis in solid organ transplant candidates and recipients: current and future challenges. Donor-derived Trypanosoma cruzi infection in solid organ recipients in the United States, 2001-2011. Full counselling of donor and recipient is required along with access to appropriate long-term donor follow up. The lifetime risk of recurrent kidney stones is an important consideration in evaluating the suitability for kidney donation. However, data relating to risk of further stone episodes are available for people who present with a symptomatic kidney stone (overall 50% chance of developing a further stone within 5 years) and a risk prediction tool exists (1). Risk prediction tools do not yet exist for asymptomatic stone formers, but 1 stone at presentation confers an increased risk of metabolic risk factors and future stone episodes (1). In symptomatic patients who undergo metabolic evaluation (who may be a selected group), a metabolic abnormality. The remaining 25% of stones are composed of uric acid, pure calcium phosphate, cysteine or struvite (magnesium ammonium phosphate, also called infection stones) (2, 4). Uric acid stones are often associated with a history of gout, ileostomy, diarrhoea or with the metabolic syndrome, in all of which the urine is acidic. Calcium phosphate stones may occur with hypercalciuria and are the predominant stone type formed by patients with a low urinary citrate and distal renal tubular acidosis. Cystine stones are always associated with cystinuria and people with these stones should not donate a kidney. Infection stones are commonly associated with an anatomical abnormality and people with these stones should not donate a kidney unless the anatomical abnormality is easily correctable. Small stones usually pass spontaneously but can occasionally cause ureteric obstruction leading to acute renal failure in patients with a single kidney. However, for the general population, the evidence that treating small asymptomatic stones is superior to simply observing them is mixed (6), with about 25% becoming symptomatic in 5 years and 3% developing painless silent obstruction (7). Upper or middle pole stones are more likely to become symptomatic and also to pass spontaneously. It is recognised that the natural history of small asymptomatic stones detected during a donor work-up may be very different to stones presenting with clinical features or described in the existing urological literature. A recent study of 1, 957 potential kidney donors evaluated at the Mayo Clinic from 2000 to 2008 reported that 3% had past symptomatic stones, while 11% had radiographic stones detected on screening (11). In this study, asymptomatic stone formers were not characterised by older age, male gender, hypertension, obesity, metabolic syndrome, abnormal kidney function, hyperuricaemia, hypercalcaemia or hypophosphataemia. One conclusion is that asymptomatic stone formers may lack the co-morbidities found in symptomatic stone formers and that different mechanisms may be involved in asymptomatic versus symptomatic stone formation. On balance, it is likely that the risks of recurrent stone formation are low in asymptomatic potential kidney donors. However, in the absence of a reliable evidence base, a degree of caution is warranted. Large or staghorn stones can commonly lead to chronic renal damage (2) and are usually associated with infection or a significant metabolic abnormality and people with these stones should not be considered as donors. In transplant recipients, the long-term risks associated with a small stone transferred from the donor kidney appear low (6, 7). If a probable stone is identified on imaging, a urological and radiological review should be undertaken. The number, size, position and density of the potential stones should be considered; as should the presence of any underlying structural renal abnormality. Biochemical Assessment A full metabolic and imaging screen should be carried out before donation on potential donors with a history of stone disease or radiological evidence of a current stone. This screen should include 24-hour urine collections for calcium, oxalate, citrate and urate, and early morning pH assessment. This will require two separate urine collections as calcium, oxalate and citrate analyses require an acidified collection, whereas electrolytes, urate and pH are measured in a plain urine collection. A pH measurement on an early morning urine sample is useful, together with a qualitative cystine screen for cystinuria (8), followed, if positive, by a 24-hour collection for cystine concentration. A metabolic screen (urine and plasma biochemistry) may also be indicated in potential donors with a significant family history of stone disease or with significant risk factors for the development of stones. In patients with previous calculus disease, where a stone has been retrieved, biochemical stone analysis is also of value. If a significant and uncorrectable metabolic abnormality is identified then kidney donation is contra-indicated (9). However, donation may be considered in potential donors with minor or correctable metabolic abnormalities. Donation may be considered where factors that have previously put the patient at risk of stone formation. It is recommended that advice is obtained from a clinician with a specific interest in this field. A history of a previous infection-related (struvite) or cystine renal stone is generally considered a contra indication to donation. In potential donors who have a history of previous stones but no metabolic abnormality, proceeding with donation should be considered providing the number, size and frequency of previous stones has been low. Potential donors found to have small stone(s) on imaging, or cases where there is uncertainty as to whether there is a true calculus or parenchymal calcification, may be suitable to donate. Both need to be aware of the limited data regarding long-term outcomes in these circumstances (10). The smaller the stone bulk and the older the potential donor, the lower is risk associated with proceeding to donation. If donation proceeds, it is preferable to remove the kidney containing the suspected calculus. However, it is relatively straight forward, with urological input and modern flexible ureterorenoscopes, to inspect the collecting system and remove any confirmed stones ex vivo, before implanting the donor kidney (15, 16). Leaving the donor with a single kidney containing a possible small stone is undesirable, but may be considered in exceptional circumstances. Full counselling of the donor is required in this situation and appropriate close long-term follow-up of the donor is necessary. People with bilateral kidney stones should in general not be considered as kidney donors. This situation both suggests an inherent metabolic or anatomical abnormality and would leave the individual with a single kidney containing a stone placing them at significant risk of a future stone event in a solitary kidney. Donors who have a past history of stones and those who have donated a stone bearing kidney should be counselled about symptoms of renal/ureteric colic and anuria and information should be provided regarding the availability of local urological expertise. Donors should also be advised to maintain a high fluid intake for life (at least 2. Progression of nephrolithiasis: long-term outcomes with observation of asymptomatic calculi. The natural history of nonobstructing asymptomatic renal stones managed with active surveillance. Prevalence and early outcome of donor graft lithiasis in living renal transplants at the Mayo Clinic. The evaluation of living renal transplant donors: clinical practice guidelines: Ad Hoc Clinical Practice Guidelines Subcommittee of the Patient Care and Education Committee of the American Society of Transplant Physicians.
Discount 150 mg diflucan
Monitoring strategies are designed to follow individual organ function and fungus kingdom purchase diflucan 400 mg line, to a lesser degree, the interaction between systems. However, monitors are limited in their ability to interrogate tissue health and cellular function. Furthermore, individual monitor values are often insufficient to draw conclusions about global physiology. For example, a normal 83 blood pressure may not be interpreted to signify adequate cardiac output or perfusion just as normal urine output may not equate with normal renal function. The risk of infection (~5%) starts to increase after five days and is not improved with prophylactic antibiotics. The technology makes use of the principle that increase pressure will place greater strain on the diaphragm at the distal tip which can be interpreted as pressure values using experimental norms. This drift may begin as soon as 48 hours after catheter placement, though many intensivists argue that the vast majority of intracranial hypertensive issues occur early in patient courses. Therefore, additional monitors of cerebral oxygenation and metabolism are undergoing evaluation. Monitors of Cerebral Perfusion Jugular bulb saturation is a global marker of cerebral perfusion. It is insensitive to small regional abnormalities in brain oxygenation and has largely been abandoned in clinical use. Normative values are being developed, with PbtO2 < 10mmHg in adults being considered abnormal. If the catheter is not placed into the area of injury, the data may not correlate with metabolic activity in the zone of injury. Furthermore, it remains unclear whether such monitors should be placed in the area of injury, the penumbra (area around injury at risk for spread of damage), or in a distant site. A microcatheter placed into the brain parenchyma can measure cerebral glucose, lactate, pyruvate, glutamate, aspartate, and glycerol. Differing ratios in measured diasylate concentrations are thought to reflect altered substrate delivery and/or substrate utilization. This methodology again only measures the local effects in the tissue where the catheter is placed. Furthermore, the application of a flank sensor (measuring renal/somatic perfusion) allows comparison of cerebral and somatic perfusion. Surface tonometry can be used in the neonatal population with an open anterior fontanelle. The measured pressure is influenced by the amount of external pressure, hence making the reported result less valuable than the trend. Other Methodologies for Monitoring Brain Perfusion Transcranial oxygen saturation monitors have been employed in adults to show hemispheric oxygen levels. While the absolute values may be less valuable, trends are potentially useful to evaluate hemispheric oxygenation. However, significant decline in cerebral oxygen saturation may occur once tissue damage from intracranial hemorrhage or embolism/thrombosis is established and, therefore, less likely to be reversible. Using 20 87 electrodes to be placed on the scalp for at least 12 continuous hours, one may detect subclinical seizures. Routine use in adults has been shown to decrease intraoperative awareness, but this has not been validated in children. Special Considerations in infants versus older children Many of the monitoring devices discussed above have either not been used in infants or have not been adequately validated to interpret absolute values. Therefore, while the clinician may obtain an ever expanding data set with regard to neurologic function in the neonate, enthusiasm must be matched with skepticism regarding the validity of any specific values. Pulse oximetry makes use of the principle that hemoglobin saturated with oxygen (or other gases) will exhibit different absorbance and transmittance characteristics for specific wavelengths of light. By testing normal patients in the range of tolerable oxygen saturation (75-100%) and inferring the characteristics at lower saturations, manufacturers built algorithms to report continuous oxygen saturation that approximated arterial blood gas measurements to within 2-5 percent in the higher ranges and 10% at the lower ranges. The addition of two more wavelengths has resulted in absolute values that reliably lie within 2% of blood gas measurements and can accurately report total hemoglobin, methemoglobin, and carboxyhemoglobin concentrations on a continuous basis. The arterial partial pressure of oxygen (PaO2) may be a more direct measure of the efficiency of gas exchange at the alveolar/capillary junction and is, therefore, an important tool to assess the degree of pulmonary dysfunction. Using the oxygen content equation (shown below), it becomes readily apparent that changes in SaO2 have substantially greater impact on oxygen content. Therefore, there is no mathematical threshold of oxygen saturation that signals patient risk. Many intensivists empirically target 90% or greater as the desirable values though this is neither supported by available data nor by the mathematical principles of the equation. An important, but often overlooked additional value of pulse oximetry is the presence and quality of the waveform. An astute clinician recognizes that 90 this device also reports heart rate, may be a sensitive indicator of non-perfusing dysrhythmias, and may indicate low cardiac output states. The waveform visually demonstrates beat-to beat perfusion and, though subject to artifact such as patient movement and electrical interference, is a sensitive indicator of perfusion. In children with patent ductus arteriosus and with structural congenital heart disease, arterial oxygen saturation may vary by location. Post-ductal saturation (lower extremities) reflects a mixture of blood ejected from the left ventricle and systemic venous blood from the pulmonary artery. Thus, pre-ductal saturation is a better tool to assess pulmonary function though the absolute value may be affected by changes in intracardiac shunt. In contrast, post-ductal saturations are indicative of the significance of pulmonary hypertension and the oxygen content delivered to abdominal viscera. Apnea and bradycardia monitoring Premature infants (<36 weeks gestation and total gestational age <60wks) frequently experience apnea and may become bradycardic as a result. This may occur spontaneously, but is also a well-recognized consequence of illness, operation/anesthesia, and physiologic stress. When combined with continuous pulse oximetry, these tools are effective at notifying clinicians of impending compromise. Simple stimulation of the infant is often sufficient to address an apnea episode, though more definitive airway control may be required. In practice, ventilation/perfusion mismatch, timing of emptying of regions of lung, and lung disorders lower the detected values and limit the utility of the absolute value obtained in capnometry. However, trends in the capnometric measurement may be interpreted to reflect changes in endogenous C02 production, minute ventilation, expiratory restriction, and effective pulmonary perfusion as described in the examples below: 1. A normal waveform begins from a baseline value of zero (inspired gas washout), increasing towards an upper baseline, slowly rising towards the end-expiration value (gradual increase expiration of lung units), a rapid down-sloping line (initiation of inspiration), and rapid return to zero during the remainder of inspiration. Asthma and other expiratory restrictive changes will manifest a slower upslope and either truncated or, more commonly, absent upper baseline. Each may report values for gas partial pressure validated to track the trend of capillary gas concentrations, but do not report hemoglobin oxygen saturation. The devices are generally applied on the trunk and generally must be moved every two days or more frequently. Cardiac Monitoring 94 Cardiac monitoring begins with rhythm and rate evaluation and surrogate measures of function such as blood pressure. In recent years, many of the more invasive measures have been deemed unnecessary and surrogates have been increasingly used as indicators of cardiac function.
| Comparative prices of Diflucan | ||
| # | Retailer | Average price |
| 1 | Ruddick Corp. | 789 |
| 2 | Menard | 468 |
| 3 | SonyStyle | 749 |
| 4 | PetSmart | 161 |
| 5 | Wendy's / Arby's Restaurants | 575 |
Buy 200mg diflucan free shipping
Incise the skin on the medial aspect of each leg and reflect it to expose the muscles and stifle joint fungal watch buy diflucan now. Connect the lateral skin incisions with a transverse skin incision across the middle of the abdomen. Reflect the skin of the breast anteriorly and, the skin of the abdomen posteriorly. Make a longitudinal incision through the pectoral muscles on each side of the keel and over the costochondral junctions. The anterior end of each incision should intersect the thoracic inlet at the dorso-ventral midpoint. With sterile scissors make a transverse incision through the posterior part of the abdominal muscles. On each side continue the incision anteriorly through the costochondral junctions. Remove the ventral abdominal wall and breast as one piece, observing the air sacs as they are torn during removal. If air sacs are cloudy they can be cultured for bacteria including mycoplasma and fungus if necessary. Using sterile instruments remove any organs and take any swabs desired for culturing. All unnecessary manipulations and delays prior to culture increase the probability of contamination. Reflect the entire gastrointestinal tract posteriorly by cutting the mesenteric attachments and then remove it after transecting the rectum. With shears or scissors, cut through one lateral commissure of the mouth and examine the oral cavity. Continue at the cut commissure and make a longitudinal incision through the skin of the neck to the thoracic inlet. Reflect the skin laterally and examine the paired vagus nerves and the thymus if present. Examine syrinx also, some times aspergillus lesions are present only in the syrinx. With heavy scissors, remove the upper beak by a transverse cut as near the eyes as possible. This will allow inspection of the nasal cavity and will expose the open anterior end of the infraorbital sinuses. Make a longitudinal lateral incision through the wall of each sinus and examined them. If you suspect aortic rupture in turkeys (blood in the abdominal cavity), dissect the aorta starting at the origin near the heart and continuing distally till you can find the rupture. Examine the lungs by reflecting them medially from their attachment to the rib cage. For histopathology collect lungs at the entrance of the primary bronchus for best results. With knife or scissors make a longitudinal incision through the proventriculus, ventriculus, small intestine, ceca, colon, and cloaca. Examine brachial plexuses, sciatic nerves and vagus for any enlargements or loss of cross striation. The sciatic nerves are exposed by careful separation of the adductor and semimembranous and semitendinoses muscles. The intrapelvic portion of the sciatic nerves can be exposed by removal of the overlying portion of the kidneys by blunt dissection. Vagus can be examined on the lateral sides of the neck (it is easier to examine the left vagus) 25. Using a sharp knife open each tibiotarsal joint (coxofemoral joint, stifle and foot pad if necessary) and examine the joint fluid for signs of exudate. Remove the calvarium with strong scissors cutting the skull starting at the atlantooccipital joint and continuing on and around till the cut is complete at the opposite side of the atlantooccipital joint. Other organs such as thyroids (at the thoracic inlet), parathyroids, adrenals, eyes, gland of Harder, ears, spinal cord with vertebrae intact should be collected for histopathology depending on the clinical signs and pathology. Therefore, consider obtaining blood samples for serology, culturing organs for bacteria and collect tissues for histopathology any organ that has lesion/s and save tissues for further tests. Bacteriology: Aerobic, anaerobic, campylobacter, mycology, coliforms, botulism toxin, etc. Toxicology: Heavy metals, selenium, vitamins (A and E), ionophore screen, mycotoxins, salt screen, trace element screen, anticoagulant screen, herbicide screen, cholinesterase, insecticides/pesticides, domoic acid, metaldehyde, avitrol, plant identification, zinc/aluminum phosphide, etc. Intestine: make smears on glass slides for coccidia and other parasites Transmission electron microscopy (negative stain): pool of small intestine (and ceca) in viral transport media. Liver also for vitamins (A, E), selenium, insecticides/pesticides, rodenticides and certain aflatoxins. If the bird/s is live observe the bird/s for clinical signs such as respiratory, diarrhea, neurological, weakness, etc. If blood is available make a blood smear especially from pigeons, wild birds, etc. Observe the exterior: conjunctiva/eyes, feathers, skin, nostrils, vent, uropygial gland, toes, keel, etc. If information is not available, talk to the owner regarding the breed and age (age is difficult to determine if wild caught). Record the nature and amount of contents if any in crop, proventriculus, gizzard, intestine. Record all lesions accurately, if necessary weigh organs like liver, heart, spleen, etc. Photograph the whole bird with accession # clearly visible if it is a legal or insurance case. Disposal of carcasses and remains: should be done according to the protocols; in a biohazard bag for autoclave or incineration especially psittacines. Save: i) Liver, spleen, kidney, lung, heart, brain, intestine in viral transport media for virology. Take the tissues for histopathology (see the list below) List of tissues to be collected for histopathology (Note: Take any tissue that looks abnormal/has a lesion. There are anatomical differences between various species (>22, 000 subspecies) of birds and ages. He has been involved in avian diagnostics, teaching and research for more than 35 years. His primary research interests are to identify novel etiologies and diseases of both infectious and noninfectious nature and study their pathogenesis in avian species. He has published extensively in journals, books and proceedings and has presented numerous papers in national and international conferences. He is a member of many professional organizations, serves on the editorial board of one journal, associate editor of Avian Pathology J and is an ad-hoc reviewer of a number of other journals. He was the senior author of the best paper published in the J of Veterinary Pathology in the year 2011. He was also the recipient of Lasher Botorff award in 2015 awarded by the American Association of Avian Pathologists in his recognition as an eminent avian pathologist and for his contribution to the poultry health programs in North America He has traveled to more than 30 countries on invitation primarily for teaching. The ability of the authors to condense their lecture material to the limited number of pages before you is a testimony to them and is very much appreciated. These pages have been reproduced directly from their submitted manuscripts and any questions concerning their content should be directed to the authors. Diastolic dysfunction (inability for ventricles to relax) is also a common finding. Typically the disease targets the left ventricle, but in some cases both ventricles may be affected.
Cheap 200mg diflucan otc
Percentage of necrosis after neoadjuvant systemic therapy fungus gnats thc buy discount diflucan 400 mg on line, from pathology report: 4. Number of resected pulmonary metastases, from pathology report: this form continues on the next page. Soft Tissue Sarcoma of the Head and Neck 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. Soft Tissue Sarcoma of the Head and Neck 6 Registry Data Collection Variables See chapter for more details on these variables. Soft Tissue Sarcoma of the Trunk and Extremities 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. Soft Tissue Sarcoma of the Trunk and Extremities 5 Prognostic Factors Required for Stage Grouping 5. Soft Tissue Sarcoma of the Trunk and Extremities 7 Registry Data Collection Variables See chapter for more details on these variables. Soft Tissue Sarcoma of the Abdomen and Thoracic Visceral Organs 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. Soft Tissue Sarcoma of the Abdomen and Thoracic Visceral Organs 6 Registry Data Collection Variables See chapter for more details on these variables. Necrosis Definition Score 0 No necrosis 1 <50% tumor necrosis 2 50% tumor necrosis this form continues on the next page. Tumor site: esophagus stomach duodenum jejunum/ileum rectum extraintestinal 3. Soft Tissue Sarcoma of the Retroperitoneum 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. Soft Tissue Sarcoma of the Retroperitoneum 5 Prognostic Factors Required for Stage Grouping 5. Soft Tissue Sarcoma of the Retroperitoneum 7 Registry Data Collection Variables See chapter for more details on these variables. Merkel Cell Carcinoma 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. Merkel Cell Carcinoma 6 Registry Data Collection Variables See chapter for more details on these variables. Largest tumor diameter (in millimeters): measured clinically measured histologically 2. Tumor nest size in regional lymph node(s) (greatest dimension of largest aggregate in millimeters): 14. Eyelid tumor involving the upper or lower eyelid, or both: upper eyelid lower eyelid both 16. Eyelid tumor involving the eyelid margin, defined as the juncture of eyelid skin and tarsal plate at the lash line: yes no If present, is the eyelid margin involvement full thickness Melanoma of the Skin 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. N0 No regional metastases detected No N1 One tumor-involved node or in-transit, satellite, and/or microsatellite One tumor-involved node or in-transit, metastases with no tumor-involved nodes satellite, and/or microsatellite metastases with no tumor-involved nodes N1a One clinically occult. By convention, clinical staging should be used after biopsy of the primary melanoma, with clinical assessment for regional and distant metastases. Note that pathological assessment of the primary melanoma is used for both clinical and pathological classification. Diagnostic biopsies to evaluate possible regional and/or distant metastasis also are included. Melanoma of the Skin 6 Registry Data Collection Variables See chapter for more details on these variables. Microsatellites (pathologically detected satellites, not clinically apparent) (yes/no) 5. Microscopic confirmation of tumor metastasis in any regional lymph node that was clinically or radiologically detected (yes/no) 13. Number of lymph nodes examined from completion or therapeutic lymph node dissection (whole number) 20. Number of lymph nodes involved with tumor from completion or therapeutic lymph node dissection (whole number) 21. Tumor thickness is measured from the top of the granular layer of the epidermis to the deepest invasive cell across the broad base of the tumor. Tumor thickness is measured from the top of the granular layer of the epidermis (or, if the surface overlying the entire dermal component is ulcerated, from the base of the ulcer) to the deepest invasive cell across the broad base of the tumor. Tumor thickness is measured from the base of the ulcer to the deepest invasive cell across the broad base of the tumor. Breast It is important to note that there are Definitions of Histologic Grade (G) for in situ breast tumors and invasive breast tumors. We have not divided the staging forms due to the complexity of breast cancer staging and the length of the single form, but it is important to note this distinction when documenting grade. Breast 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. Carcinomas in the breast parenchyma associated with Paget disease are categorized based on the size and characteristics of the parenchymal disease, although the presence of Paget disease should still be noted. T1 Tumor 20 mm in greatest dimension T1mi Tumor 1 mm in greatest dimension T1a Tumor > 1 mm but 5 mm in greatest dimension (round any measurement >1. OncotypeDx is the only multigene panel included to classify Prognostic Stage because prospective Level I data supports this use for patients with a score <11. Future updates may include results from other multigene panels to assign cohorts of patients to prognostic stage groups when there are high level data to support these assignments. It uses clinical tumor (T), node (N) and metastases (M) information based on history, physical examination, any imaging performed (not necessary for clinical staging) and relevant biopsies. Genomic profile information is not included in Clinical Prognostic Stage as pathologic information from surgery is necessary to ascertain the prognosis using these tools. It includes all information used for clinical staging plus findings at surgery and pathological findings from surgical resection. Pathological Prognostic Stage does not apply to patients treated with systemic or radiation prior to surgical resection (neoadjuvant therapy). T1 N1mi M0 and T0 N1mi M0 cancers are included for prognostic staging with T1 N0 M0 cancers of the same prognostic factor status. T2, T3, and T4 cancers and N1mi are included for prognostic staging with T2 N1, T3 N1 and T4 N1, respectively. However genomic profiles may be performed for use in determining appropriate treatment. OncotypeDx is the only multigene panel included to classify Pathologic Prognostic Stage because prospective Level I data supports this use for patients with a score <11. Future updates to the staging system may include results from other multigene panels to assign cohorts of patients to Prognostic Stage Groups based on the then available evidence. Inclusion or exclusion in this staging table of a genomic profile assay is not an endorsement of any specific assay and should not limit appropriate clinical use of any genomic profile assay based on evidence available at the time of treatment. Breast 8 Registry Data Collection Variables See chapter for more details on these variables. Survival in breast cancer cases in relation to the structure of the primary tumor and regional lymphnodes. The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. Vulva 1 Terms of Use the cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting treatment plans or follow-up. The largest lesion or the lesion with the greatest depth of invasion will be the target lesion identified to address the highest pT stage.
Buy diflucan overnight
Directed altruistic donation A form of living donation whereby an organ or part of an organ is donated by a healthy person and contact between the donor and recipient has been made because the recipient requires a transplant fungus gnats do they bite buy diflucan 200mg line. It is an offence to remove or use an organ from the body of a living person for transplantation unless the requirements of the Human Tissue Act 2004 and the Regulations are met. Consent to removal for the purpose of transplantation has been given (or removal for that purpose is otherwise lawful); 3. The donor is asked to explicitly consent to one of the following options: implantation into another recipient, re-implantation back into the donor, research, or disposal of the organ. Give, offer or receive any type of reward for the supply or offer of supply of an organ or part of an organ; 2. Initiate or negotiate any arrangement involving the giving of a reward for the supply of, or for an offer to supply, an organ or part of an organ for transplantation; 5. Take part in the management or control of any type of group whose activities consist of or include the initiation or negotiation of such arrangements; 6. Cause to be published or distributed, or knowingly publish or distribute, any type of advertisement inviting people to supply, or offer to supply, an organ or part of an organ for reward, or indicate that the advertiser is willing to initiate or negotiate any such arrangements. This provides the first internationally agreed legal definition of trafficking in human organs, identifying the activities that ratifying States must criminalise in their national laws. It could be argued that organ donation is not, prima facie, in the best interests of the minor as a potential donor, nor is it therapeutic treatment. However, children should only be considered as living organ donors in exceptionally rare circumstances. As a minimum, good practice demands that parental consent is always obtained and, even if there is parental consent to donation, that an advanced ruling be sought from the Court before proceeding. In Scotland, living donation of solid organs from children is not permitted under the Human Tissue (Scotland) Act 2006 (see 3. In Scotland, living donation from adults without mental capacity is not permitted under the Human Tissue (Scotland) Act 2006 (see 3. The 2006 Act stipulates that the removal and use of organs, parts of organs or tissue from the body of a living person for use in transplantation constitutes an offence unless certain conditions are satisfied, including that the donor must give consent, without coercion or reward, for the removal of organs to take place. Restrictions on transplants involving living donors are set out in section 17 of the 2006 Act (25). These provisions are supplemented by the Human Organ and Tissue Live Transplants (Scotland) Regulations 2006 (the Scottish Live Transplants Regulations) (26) Prohibitions of commercial dealings in parts of a human body for transplantation are set out in section 20 of the 2006 Act (27). The 2006 Act also permits kidney paired exchange programmes and altruistic donation. The Adults with Incapacity (Scotland) Act 2000 governs adults without capacity to make their own decisions in Scotland (29). The Human Tissue (Scotland) Act 2006 prohibits the donation of non-regenerative tissue such as kidneys and liver lobes by minors (under 16 years of age) and adults lacking capacity (30). Human Tissue Authority Codes of Practice on Donation of Solid Organs and Tissue Human Tissue Act 2004 (Persons who Lack Capacity to Consent and Transplants) Regulations 2006. Gillick v West Norfolk & Wisbech Area Health Authority and Department of Health & Social Security (1985). Human Organ and Tissue Live Transplants (Scotland) Regulations 2006 (the Scottish Live Transplants Regulations). By its nature, living donor organ transplantation raises a wide range of complex ethical issues. As transplant programmes continue to expand, all health professionals involved in living donor transplantation must be familiar with the general principles that underpin and are applicable to good ethical practice (2-7). Altruistic giving may be to strangers or take place within the context of family or other relationships. There are some concerns that altruism may be compromised by hidden coercive pressures: for example, the expectation that a family member will donate an organ to help another family member in need of a transplant (9). These pressures may be exacerbated if there is a sense of urgency to transplant a recipient who, for example, is deteriorating rapidly. Dignity is often associated with the Kantian concept of the inherent dignity or special status of the human body where dignity and price are mutually incompatible: the maintenance of human dignity requires human beings to be beyond negotiable price (10). Reciprocity refers to providing benefits or services to another as part of a mutual exchange. In terms of outcome, a living donor kidney transplant would almost always be the preferred option, with better transplant and patient survival than for deceased donation. For children, living donation offers a unique opportunity for early transplantation and to minimise disruption to growth, development and school. Regardless of recipient benefit, living donation can only be justified if the interests of the donor are given primacy. The safety and welfare of the potential living donor must always take precedence over the needs of the potential transplant recipient. Whilst there are documented overall benefits for the individual donor and wider society, living donor surgery entails risk, which includes a small risk of death (see Chapter 6). In addition, removal of a kidney will inevitably cause physical harm to the donor and the potential life-long impact on health and well-being must be fully considered for every individual. It could be argued that a potential living donor may be psychologically harmed if his/her donation, for whatever reason, does not take place. The principle of autonomy provides a legitimate basis for supporting living donation. While all living donor programmes expect potential donors to be given an appropriate, detailed description of the risks of donation, it is much less clear that all such donors will listen. There is a well-described tendency for some people to decide that they wish to donate at an early stage and then to be impervious to or oblivious of any suggestion that they should make a more informed decision following counselling (13). The consent may be real, but whether it is truly informed may be questionable (see Chapter 4: Informing the Donor). While it may be possible to identify the donor who has come under overt pressure or coercion, from either the recipient or from other family members, more subtle pressures may not be revealed and/or remain undetected by health care professionals. These may make it difficult or impossible for a potential donor not to proceed through the assessment process. In most situations, the motives and autonomy of the donor will be beyond question but, in others, it can be more difficult to establish that consent is both informed and voluntary. Once the clinical assessment is complete, the Independent Assessor for the Human Tissue Authority (see Chapter 2) provides an additional safeguard for the potential donor. Members of the transplant team have individual rights as well as professional responsibilities. If a fully informed potential living donor wishes to proceed with a course of action that involves risks that go beyond that which individuals or the team find acceptable or appropriate, they are under no obligation to proceed.
Syndromes
- Injury to blood vessels
- Infection in the bone
- Death caused by bleeding, infections or other complications of a bone marrow transplant, rejection of a bone marrow graft, or severe reactions to ATG
- Nicardipine (Cardene)
- Draining
- Kidney disease or dialysis (you may not be able to receive contrast)
- T4: The cancer has spread to nearby structures such as the prostate gland, uterus, vagina, rectum, abdominal wall, or pelvic wall
- Long-term back pain or leg pain
- Excessive sunlight exposure
Purchase diflucan 400 mg without prescription
Other symptoms fungus woods rct2 diflucan 150mg for sale, such as chills, pruritic, alcohol-induced pain and fatigue, are not included in the A or B designation but are recorded in the medical record, as the reappearance of these symptoms may be a harbinger of recurrence. Coding Instructions and Codes Note 1: Physician statement of B symptoms can be used to code this data item when no other information is available. They have a preponderance for extranodal involvement, with central nervous system being the most common site. Note 2: Physician statement of presence or absence of adenopathy should be used to code this data item. Traditionally the lymphoma diagnosis was staged with the Ann Arbor staging system and it is now staged with the Lugano classification. Note 2: Physician statement of presence or absence of organomegaly should be used to code this data item. Note 3: Organomegaly is defined as presence of enlarged liver and/or spleen on physical examination and is part of the staging criteria. Note 5: If there is no mention of thrombocytopenia, or the relevant lab tests, code 9. Definition Mycosis fungoides is the most common type of primary cutaneous T-cell lymphoma. Sezary syndrome is a more aggressive type of primary cutaneous T-cell lymphoma in which a specific type of malignant T lymphocytes (Sezary cells) are present in the circulating blood. Staging of mycosis fungoides includes analysis of the circulating blood for Sezary cells. Results of microscopy are reported as counts of Sezary cells per cubic millimeter or the percentage of Sezary cells as a proportion of total lymphocytes. The basic categories are B0 (no significant blood involvement); B1 (low blood tumor burden); and B2 (high blood tumor burden). Code a statement of peripheral blood involvement and clonality (if given) as reported by the clinician from tissue and/or blood samples. Note 3: If counts or percentages of neoplastic cells and clonality test results are available, but a B rating is not stated by the physician, the registrar can use the information and assign a B rating and code this data item accordingly. This schema discriminators collects the specific terminology used to describe the plasma cell myeloma at the time of diagnosis. Code the terminology used by the physician to describe the plasma cell myeloma from any documentation in the medical record. If other terminology is used later in the course of the disease to describe more aggressive plasma cell myeloma, do not change the code in the schema discriminator. Coding Instructions and Codes Note 1: Several terms are used to characterize plasma cell myeloma at the time of diagnosis. All these terms are reportable according to the new Hematopoietic and Lymphoid Neoplasms rules effective for cases diagnosed January 1, 2010 and later. Note 2: Select the code based on the terminology specified by the physician in the record. Note 3: Do not change the discriminator code if a term used later indicates progression to a more aggressive disease course. Note 4: If diagnosis is plasma cell leukemia variant and is diagnosed concomitant with plasma cell myeloma, code 0. Coding Instructions and Codes Note 1: Physician statement of presence or absence of high-risk cytogenetics can be used to code this data item. Increased production or destruction of these cells causes Serum 2 (beta-2) Microglobulin level to increase. Elevated Serum 2 (beta-2) Microglobulin level is a prognostic factor for plasma cell myeloma. Nearly all people with polycythemia vera, and about half of those with primary myelofibrosis and essential thrombocythemia, have the mutation. In 2001, clinical researchers linked several benign aspects of the disorder to the possibility of developing kidney cancer. Communicating to the outside world about this condition has been slow and arduous, although we are making progress. So far, up to 1000 individuals have been involved in studies regarding this condition, but most likely thousands more individuals are going undiagnosed. These facts, along with the knowledge that most doctors do not even know that this condition exists, prompted us to create this handbook. Medical information on this site is reviewed by our Medical, Research and Support Page 5 Council. Information provided in this Handbook and on the website is designed to support, not replace, the relationship that exists between a patient or site visitor and his or her physician. These details are shared within this organization among staff and volunteers for the purpose of providing service to you, but are never shared with, rented or sold to other organizations. All staff and volunteers have made confidentiality agreements to protect your information. Computer Tracking and Cookies the website is not set up to track, collect or distribute personal information not entered by visitors. Our site logs do generate certain kinds of non-identifying site usage data, such as the number of hits and visits to our sites. This information is used for internal purposes by technical support staff to provide better services to the public and may also be provided to others, but again, the statistics contain no personal information and cannot be used to gather such information. Site information is used to help us serve these search sites with the correct information about our material, No personal information is collected. We do not generate personal data, do not read personal data from your machine and do not store any information other than what you voluntarily submit to us. Links to Third Party Sites the links included within the service may let you leave this site. Rather, by providing context and understanding, we hope that the information provided in this Handbook and on the website will empower the patient to be a better partner in his or her own care and will facilitate constructive conversations between patient and physician. Medical, Research and Support Council Links to each member can be found at hlrccinfo. Please contact your local group and your tax advisor for specific information on guidelines for tax deductibility of donations. There is a 50% risk of passing this on and the severity of the disease can vary a lot from person to person.
Buy diflucan 100mg overnight delivery
In the third stage fungus yeast infection treatment discount 400mg diflucan overnight delivery, severe haemorrhagic diathesis, and cyanogenic glycoside linamarin. This is normally converted necrotic pharyngitis and laryngitis can occur, resulting to the less toxic thiocyanate by the enzyme rhodanese. The in death in some instances, by total oclusion of the substrate for this reaction is sulfur originating from proteins in larynx. Optic atrophy and perceptive deafness have also been Visual disturbances and salivation have been reported in reported. Optic neuropathy results in decreased visual acute poisoning, as have conjunctivitis, rhinitis, pharyngitis, acuity, abnormal pupil size or an afferent pupillary defect, and epistaxis. Main feature is spastic paralysis of toxins were used both in Southeast Asia and Afghanistan. They include cyanogenic paraparesis have been described in many areas of the world plants, fava beans, cycads, sweet pea and prickly poppy. Pancreatitis Cyanogenic Plants and endemic goitre have also been reported in patients from Examples cassava-consuming areas. Administration of cassava or Laetrile in animal studies Cyanogenic plants may contain amygdalin or other glyco have resulted in limb defects, open eye defects, microcephaly, sides, which on hydrolysis can release traces of cyanide. Sodium thiosulfate administra following contain mostly glycosides other than amygdalin: tion protected the foetus from such teratogenic effects. However, there is one report of deaths well in Madhya Pradesh, Bihar, Uttar Pradesh, West Bengal, 532 of three patients after a single meal of cassava. Amygdalin is the cyanogenic diglucoside Clinical Features D-mandelonitrile-beta-D-gentiobioside, and is not toxic until it is metabolised by the enzyme emulsin which is present in the Chronic intake of kesari dal leads to the development of seeds of these plants. Synthetic amygdalin (laetrile) has been lathyrism, characterised by gradually progressing bilateral tried without signifcant success, in the treatment of cancer. There may be prodromal manifestations Overdose of amygdalin can produce manifestations of cyanide such as cramps, prickling sensation, and nocturnal calf pain. Peach (Prunus persica) Exclusion of kesari dal from diet and symptomatic measures. One of the richest sources of amygdalin is the bitter almond and it has been established that 40 to 60 seeds, yielding 70 mg of hydrocyanic acid would result in severe toxicity or death. Acute toxicity results in dyspnoea, weakness, dizziness, sweating, vomiting, disorientation, convulsions, paralysis, cyanosis, coma, and cardiovascular collapse. Severe poisoning must be treated on the same lines as for cyanide poisoning (page no 367). The usual antidotes (nitrites and thiosulfate) should be administered in patients who are clinically symptomatic (unstable vital signs, 33. Administer 100% humidifed supplemental oxygen with assisted ventilation as required. Botanical Name Argemone mexicana Physical appearance this is a robust, prickly, annual or perennial herb belonging to family Papaveraceae, which grows up to 4 feet in height, bearing thistle-like leaves and yellowish fowers 33. The leaves are pinnately cut, while the fowers are solitary, showy, and yellowish. The fruit is a prickly capsule, and bears many small seeds which are tiny and brownish black. In India, mustard oil and other vegetable oils are often adulterated deliberately with argemone oil. Mode of action Berberine and protopine are found throughout the entire plant, while sanguinarine and dihydrosanguinarine are found Liver, heart, kidneys, and lungs are the target organs of in the seeds. Decrease in renal blood fow sets into motion a compensatory mechanism through the activation of renin-angiotensin-aldosterone system, and retention of sodium and water. Conservation of fuid and salt compensates for the expanded vascular capacity and increased permeability in mild cases. Hypoalbuminaemia, raised alpha-2 globulin, reversal Exudation of protein-rich fuid from pulmonary capillaries of albumin-globulin ratio. Adulteration of light yellow mustard seeds with in the pleural, pericardial, and peritoneal cavities. Adulteration of dark mustard seeds can be detected by placing the seeds in normal saline. Identifcation of adulterated mustard oil: mustard or vegetable oils results in a condition called epidemic a. Diarrhoea, abdominal yellow, orange, or crimson, depending on the amount pain, and fever are often present in the early stages. Thin Layer Chromatography: Researchers at the Differential Diagnosis National Institute of Nutrition, Hyderabad, have devel Hypoproteinaemic states oped a highly sensitive quantitative assay of sangui Nephrotic syndrome narine by thin layer chromatography. Management of cardiac failure: bed rest, salt restriction, digitalis, and diuretics. The outbreaks have mostly been confned to West Bengal, Bihar, Scombroid poisoning is a form of ichthyosarcotoxicosis (the Madhya Pradesh, Orissa, Uttar Pradesh, Gujarat, Delhi, and toxin is contained within the fesh of the fsh). The most recent epidemic occurred in 1998 from consumption of improperly preserved fsh in which the in Delhi, claiming 65 lives out of a total number of 2552 endogenous histidine has been broken down by bacteria into cases reported from all across the state. Unfortunately, tainted Almost all the outbreaks have been due to consumption fsh may look and smell normal. To add insult to injury, even if such contami argemone oil (except the South African epidemic which nated fsh is subsequently cooked well or smoked, the toxins occurred due to adulteration of wheat four with argemone are not destroyed. Scombrotoxin formation can also occur if the fsh Poisoning resulting from fish and other marine creatures is improperly refrigerated. Few minutes to few hours: Symptoms may develop as early Poisonous fsh are subdivided into: as 5 to 10 minutes after eating the fsh, or be delayed up to 1 Ichthyosarcotoxic fsh, which contain a toxin within their to 2 hours. Although most cases are mild and self-limiting, fesh, resolving in 3 to 36 hours, potentially life-threatening effects Ichthyohaemotoxic fsh, which have poisonous blood, and have occurred. Diarrhoea and vomiting are also common fndings after Tuna, bonito, escolar, skipjack, mackerel, needlefsh, saurie, scombroid poisoning. Tachycardia/bradycardia and hypotension have been mahi, marlin, anchovy, herring, swordfsh, Australian ocean described. Illness is usually associated with more than 100 mg of histamine per 100 gm of fesh (though illness can result from much less 33. Diagnosis can be confrmed by measuring the histamine level in the fsh which may exceed 100 mg%. Cimetidine has been successful in patients refractory to conventional antihistamines. Ciguatera Poisoning Source Ciguatera poisoning is the commonest form of seafood poisoning, accounting for more than 50% of the cases. Barracuda, sea bass, parrot fsh, red snapper, grouper, amber jack, kingfsh, sturgeon, and many other large-sized fsh are the main culprits. The following are associated most commonly with outbreaks of poisoning: grouper 33. The latter are in turn consumed by larger carnivorous fsh, and the ciguatoxin 33. Bradycardia and orthostatic hypotension have also been 537 and viscera) of larger and larger fsh. Respiratory depression, dyspnoea, and bronchospasm poisoning have been reported from some areas of the Indian may also occur.
Order diflucan once a day
Isolated ablation congenital complete heart block has a favourable outcome Catheter ablation may be necessary in the case of drug-refractory during pregnancy fungus gnats in worm bin buy diflucan visa, especially when the escape rhythm has a and poorly tolerated tachycardias. Supportive pacing during pregnancy is exposure, ablation should be postponed to the second trimester usually not necessary. Vaginal delivery carries no extra risks in a if possible, and it should be performed at an experienced ablation mother with congenital complete heart block, unless contraindi centre with suitable lead shielding and maximal use of echo and cated for obstetric reasons. Fetal radiation dose and risk from catheter ablation procedures during pregnancy have been cal culated25 (see Section 2. I C Immediate electrical cardioversion is recommended for acute treatment of any tachycardia with haemodynamic instability. Hypertensive disorders accident, organ failure, and disseminated intravascular coagulation. Hypertensive disorders in pregnancy remain a major cause of the fetus is at risk for intrauterine growth retardation, prematurity, maternal, fetal, and neonatal morbidity and mortality in developing and intrauterine death. These women are at higher risk for problem in pregnancy, complicating up to 15% of pregnancies and 203 severe complications such as abruptio placentae, cerebrovascular accounting for about a quarter of all antenatal admissions. Pre-eclampsia pregnant patients with hypertension include urinalysis, blood occurs more frequently during the rst pregnancy, in multiple count, haematocrit, liver enzymes, serum creatinine, and serum fetuses, hydatidiform mole, or diabetes. Proteinuria should be standardized in 24 h urine collec tal insufficiency, often resulting in fetal growth restriction. Ultrasound investigation of the adrenals of prematurity, accounting for 25% of all infants with very low and urine metanephrine and normetanephrine assays may be con 214 birth weight (, 1500 g). Although it might be benecial for the mother within the short time frame of pregnancy. However, close monitoring and, if necessary, trimester, switching to another medication and close monitoring resumption of treatment is necessary. The only trial of treatment of hypertension in pregnancy with a-Methyldopa is the drug of choice for long-term treatment of 216 adequate infant follow-up (7. Diuretics should be hypertension (pre-eclampsia), in which the only effective treat avoided for treatment of hypertension because they may decrease ment is delivery. They are not recommended in and the presence of associated maternal and fetal risk factors, pre-eclampsia. This Task Force recommends women, because it can lead to reduced neonatal weight and following these guidelines. The drug of choice in hypertensive crises is hypertension in pregnancy sodium nitroprusside given as an i. Table 16 Recommendations for the management of hypertension Delivery a b Recommendations Class Level Induction of delivery is indicated in gestational hypertension with proteinuria with adverse conditions such as visual disturbances, Non-pharmacological management for pregnant coagulation abnormalities, or fetal distress. Bromo gestational hypertension or with hypertension criptine, which is used to suppress lactation, may induce hyperten and subclinical organ damage or symptoms at sion. Methyldopa should be avoided oedema, nitroglycerine given as an intravenous I C post-partum because of the risk of post-natal depression. Women experiencing hypertension in their rst pregnancy are at Women with pre-existing hypertension increased risk in a subsequent pregnancy. The relative risk of developing ischaemic heart disease after pre-eclampsia is more than twice as high compared with women with normal preg 10. Venous thrombo-embolism nancies, and the risk of developing hypertension is almost four 229 during pregnancy and the fold. Women with early-onset pre-eclampsia (delivery before 32 weeks of gestation), with stillbirth, or fetal growth retardation puerperium 229 are considered to be at highest risk. Risk factors before preg nancy for the development of hypertensive disorders are high 10. Therefore, identication of risk factors in the individual Mid-cavity or rotational forceps patient is important for risk assessment and choice of preventive Prolonged labour (>24 hours) strategies. Peripartum haemorrhage (>1 L or transfusion) Table 17 provides a suggested checklist for documentation of Transient risk factors 238 this risk assessment. On the basis of the type and the total Current systemic infection number of risk factors present in the individual patient, three risk groups can be identied (high, intermediate, and low risk Immobility groups) and preventive measures applied accordingly (see Table 19). This complicates recommendations and but there are no studies available on the optimal dose and weight calls urgently for multicentre, prospective studies. Subjective clini centration for each trimester compared with the previous cal assessment of pulmonary embolism is, however, more difficult, one. Patients with: Low In low risk patients early mobilization and avoidance of risk dehydration is recommended. Several risk scores for identication of patients at different risk levels have been developed, 240 yet all risk scores, including the above, still need validation in prospective studies. It is favoured measured in patients with suspected pulmonary embolism, in patients with renal failure and when urgent reversal of anticoa followed by bilateral compression ultrasonography. If this is gulation by protamine is needed, as well as in the acute treatment normal in the presence of negative D-dimer levels, then pulmon of massive pulmonary emboli. In patients with acute pulmonary embolism with haemo In patients with suspected pulmonary embolism, positive dynamic compromise, i. Fetal loss of 6% and 6% pre-term delivery Heparin-induced thrombocytopenia is markedly lower with 250 were reported. Whereas it is therefore not been evaluated, and is not recommended in preg considered necessary in patients with mechanical valves in nant patients. Indications for vena cava lters are the same as in nancy progresses to maintain a certain therapeutic anti-Xa non-pregnant patients. Vitamin K antagonists may be started on the second day pregnancy and puerperium after delivery and continued for at least 3 months or for 6 months if pulmonary embolism occurred late in pregnancy. Isolated iliac vein thrombosis may manifest with isolated pain in In intermediate risk patientsd post-partum the buttock, groin, ank, or abdomen. In women with a high pre-test probability, a positive D-dimer and a normal initial compression ultrasound magnetic aClass of recommendation. Drugs during pregnancy and be applied, weight adjusted, twice daily (see treatment of pulmon ary embolism). There are no uniform rec thrombo-embolism in pregnancy and ommendations for the treatment of pregnant women yet. As drug treatment in pregnancy concerns the mother Category D: there is evidence of human fetal risk, but the benets and the fetus, optimum treatment of both must be targeted. Category X: studies in animals or human beings have demonstrated In case of emergency, drugs that are not recommended by the fetal abnormalities, or there is evidence of fetal risk based on pharmaceutical industry during pregnancy and breastfeeding human experience, or both, and the risk of the use of the should not be withheld from the mother. The potential risk of a drug in pregnant women clearly outweighs any possible drug and the possible benet of the therapy must be weighed benet. Different sources of evidence can be used for risk classication of drugs applied during pregnancy. Category B: either animal reproduction studies have not demon strated a fetal risk but there are no controlled studies in preg 11. For this and for legal reasons, drugs are frequently considered Category C: either studies in animals have revealed adverse effects prohibited during pregnancy and breastfeeding. Drugs should be given only if potential benets justify the potential risk to the 11. Acenocoumarola Vitamin K antagonist D Yes Yes (no adverse effects Embryopathy (mainly first trimester), reported) bleeding (see further discussion in Section 5 for use during pregnancy). Acetylsalicylic acid Antiplatelet drug B Yes Well-tolerated No teratogenic effects known (low dose) (large datasets). Adenosineb Antiarrhythmic C No No No fetal adverse effects reported (limited human data).
Purchase discount diflucan
The primary sources of this contamination were on-base leaking storage tanks and industrial activities antifungal groin best order for diflucan, and an of-base dry cleaner. It is estimated that the contaminants were in the water supply from the mid-1950s until February 1985, when the wells were shut down. In addition, Eligibility timeframe Veterans can receive disability and health care benefts Veterans, National Guard and reserve members, and for eight presumptive disease conditions associated with family members who lived on the base for at least 30 days contaminants in the water at Camp Lejeune. Camp Lejeune Historic Health Care Benefts Veterans who served at Camp Lejeune for 30 days or What areas are included To be added to the Camp Lejeune Historic the Marine Corps continues to work diligently to Drinking Water Notifcation Database, or for more both identify and communicate with registrants by information, please visit. Please share information about the registry Historic Drinking Water Call Center at (877) 261-9782 with anyone who may have been at Camp Lejeune or e-mail clwater@ usmc. These at Camp Lejeune during the qualifying period are eligible members who lived on Camp Lejeune, conditions were determined after a review for reimbursement of out-of-pocket medical expenses meet the time-on-station and service related to any of the 15 covered health conditions. Reim of scientifc and medical literature on date requirements, and have one of the bursement for medical claims can be paid for care up to health efects related to the contaminants two years prior to the date of application for benefts. The presumption applies to active duty, reserve, and Qualifying health conditions: Apply online for reimbursement at We recommend that patients ask their doctors about what tests or types of treatments are needed for their type and stage of disease. Most stomach cancers start from cells in the inner layer of the stomach (the mucosa) which normally make and release mucus* and other fluids. These cancers are called adenocarcinomas and represent about 90% of stomach cancers. The mucosa* or inner layer of the stomach is made up of the epithelium* and the lamina propria*. Going deeper in the stomach wall we find the submucosa*, followed by the muscle layers, subserosa* (not shown in the picture) and the serosa*. Important note regarding other types of stomach cancer the information provided in this Guide for Patients does not apply to other types of stomach cancers. The main other types of stomach cancer include: Gastric lymphomas, which are cancers originating from cells of the immune system found in the wall of the stomach. Diagnosis and treatment of these types of cancer are different from those for gastric adenocarcinoma. Worldwide, stomach cancer is most common in East Asia, South America and Eastern Europe. It is less common in Western Europe even though stomach cancer is the fifth most frequent cancer in Europe. The marked variation in the frequency of stomach cancer between continents and countries is mainly due to differences in diet and to genetic factors. There are marked geographic variations between countries worldwide but also within Europe. Stomach cancer is more frequent in countries of Eastern Europe and in Portugal where up to 4 in every 100 men and 2 in every 100 women will develop the disease at some point in their lifetime. A risk factor* increases the risk of cancer occurring, but is neither sufficient nor necessary to cause cancer. Most people with these risk factors* will never develop stomach cancer and some people without any of these risk factors will nonetheless develop stomach cancer. The main risk factors* of stomach cancer are: Environmental factors: Helicobacter pylori or H. However, the infection will first go through a number of pre-cancerous stages (like atrophic gastritis, metaplasia and dysplasia) that could, but do not systematically turn into cancer. These stages can already be detected and treated before they could evolve to cancer. Transmission occurs through stools and saliva and is strongly related to poor socio-economic status and poor living conditions. Besides that, it damages the mucosa* of the stomach and can in this way directly contribute to the development of stomach cancer. The type of stomach cancer due to this mutation* is called hereditary diffuse stomach cancer and has a bad prognosis*. Individuals with this mutation* might therefore consider close surveillance, or discuss a preventative removal of the stomach. Reasons for this difference are unclear, but the female sex hormone estrogen may have a protective effect. The reduced acid level may allow more bacteria to grow and the bacteria may help to produce more chemicals that may increase stomach cancer risk. Along with anemia (low red blood cell counts), the risk of stomach cancer is also increased for these patients. Unfortunately, these signals are often vague and quite common, and they can also point to many other medical conditions. In case of a combination of the following complaints, and especially if persistent, further examinations should be considered: abdominal discomfort or pain a sense of fullness, even after eating a small meal heartburn, indigestion, acidity and burping nausea and/or vomiting, especially including blood. In Japan and Korea, where there is a high number of new cases of stomach cancer, a screening is proposed to every individual at the age of 50 and with a follow-up according to the result of the screening exam. In Europe, no such screening is proposed because the number of new cases of stomach cancer is not 1 considered to be sufficient for screening to be efficient. He will also check for any abnormal swelling above the left collar bone, which may be caused by a spread of the cancer to the lymph nodes* that are situated there. This allows the doctor to see the lining of the esophagus, stomach, and the first part of the small intestine. If abnormal areas are noted, biopsies* (tissue samples) can be taken using instruments passed through the endoscope. These tissue samples are examined by a specialist in the laboratory (see histopathological* examination). A screening is proposed if a safe and acceptable exam can be performed and if this exam is able to detect cancer in the majority of cases. It should also be proved that treating screened cancers is more effective than treating cancers diagnosed because signs of cancer were present. During the gastroscopy, an endoscopic ultrasound can be performed at the same time. It provides images of the different layers of the stomach wall, as well as the nearby lymph nodes* and other structures. This technique is used to see how far a cancer has spread in the stomach wall, into nearby tissues or to nearby lymph nodes*. It can also guide the doctor in removing a small sample (biopsy*) of a suspicious lesion during the gastroscopy. The biopsy* specimen (the tissue sample that has been taken during the gastroscopy) will be examined in the laboratory by a pathologist*. Using the microscope and several other tests, the pathologist* will confirm the diagnosis of cancer and will give more information on the characteristics of the cancer. The histopathological* examination can also be performed on samples obtained during either a laparoscopy*, or on the liquid used for peritoneal washing*, or on the tumor removed during surgery. A laparoscopy* is usually performed when the stomach cancer has already been found and when an operation is foreseen. It helps to confirm that the cancer is still only in the stomach and thus can be completely removed by surgery. It has a small camera on its end, through which doctors can look closely at the surfaces of the organs and nearby lymph nodes*, and take small samples of tissue, to check for possible metastases*. Sometimes surgeons also pour liquid in the abdominal cavity, remove it by suction and send it to the laboratory to check for cancer cells. When surgery is performed to remove a tumor, the tumor and the lymph nodes* will also be examined in the lab. Doctors will need to consider many aspects of both the patient and the cancer in order to decide on the best treatment.
Purchase diflucan mastercard
Forty three cases were diagnosed as having the Symptoms do not always correlate with blood mercury Minimata disease out of whom six died fungus plague inc mega brutal generic diflucan 100mg on-line. Urine mercury level: Urinary mercury is the best biolog died out of a total of 6530 victims due to consumption ical marker for chronic elemental or inorganic mercury of imported wheat and barley meant for sowing, treated exposure. Signs and symp Unlike inorganic mercury compounds, methyl toms of toxicity may begin to occur at urinary mercury mercury is a subtle, diffcult to detect, long lasting concentrations of 20 to 100 mcg/100 ml. When large quantities of industrial waste and levels, however, often do not correlate with clinical agricultural fungicides containing mercury are released signs and symptoms of toxicity. External contamination can however vitiate 250 mg qid, for adults, (20 mg/kg/day) for 5 the results. If there had been survival for a few days, the large intestine In elemental mercury ingestion, take x-ray and may reveal ulceration. Kidneys are often pale and swollen due to oedema of renal gets lodged in the appendix, perform appen cortex. In the past when white or 5% albumin or just plain milk to the mercury was used in its various forms for the therapy of a wide lavage fuid to bind the mercury. Prolonged use can If there is abscess formation, perform repeated cause colitis dementia, tremor, and renal failure. If the globules resulting from teething powders containing calomel has fortu are very minute and widely distributed in the nately become a rarity. Many resulting from any type of exposure, the following dentists still knead the amalgam mass in the palms of their may be tried: haemodialysis, haemofltration, or hands. Haemoperfusion is said to be droplets of the metal sometimes fall to the foor where they ineffective. Take the total Environmental Sources: molecular weight of iron in the compound, and divide it by Y Iron is found in 5. This means the amount of ferrous Fumarate divided by 3; Sulfate divided by 5 and Gluconate divided by 9 is the amount of elemental iron in the prepara tion. The usual fatal dose corresponds to about 200 to 250 mg of elemental iron per kg of body weight. This can be calculated from the percentage of elemental iron in a particular prepara tion. But such calculations can be misleading since serious hepatotoxicity can result at much lower concentra tions of iron in the body which can lead to death. With 97 less serious overdoses, the initial gastrointestinal symptoms Iron poisoning occurs when serum iron level exceeds the total may be the only fndings to develop even without treatment. However, chewable iron tablets and liquid Free iron causes: iron formulations are usually not visualised on x-ray. Massive postarteriolar dilatation which results in venous Completely dissolved iron tablets/capsules may also not be pooling. Peak levels are seen Subsequent hydration of ferric iron results in metabolic around 4 hours after ingestion. Inhibits mitochondrial function leading to hepatic damage, often misleading and unreliable. Inhibits thrombin-induced conversion of fbrinogen into gas, clotting studies, liver function and renal function tests fbrin. If the serum iron has Clinical Features exceeded iron binding capacity, the excess iron is chelated Most cases occur in children. There are 5 stages: to desferrioxamine and the complex is excreted as a pinkish Stage I (0. But a negative abdominal pain, diarrhoea, haematochezia, lethargy, shock, result does not rule out iron poisoning. Severe gastro gastric fuid and 2 drops of 30% hydrogen peroxide are intestinal haemorrhagic necrosis with large losses of fuid placed in 2 plastic tubes. Free iron and ferritin produce amine (500 mg in 4 ml distilled water) is added into one vasodilatation that may also contribute to shock. If the test is positive, an orange to red contribute to a false sense of security. The test must be done within 2 hours of inges shock, severe acidosis, cyanosis and fever. Magnesium hydroxide solution (1%) administered orally Y the primary site of hepatic injury is the periportal may help reduce absorption of iron by precipitating the areas of the hepatic lobule (the principal site for hepatic regeneration), which may explain the increase in mortality and poorer prognosis. Iron induced hepato toxicity is a presumed result of free radical generation and lipid peroxidation. Iron catalyses hydroxyl radical formation (the most potent-free radical), which initiates lipid peroxidation. Based on limited data, antioxidants may have a hepatoprotective role in iron poisoning. Sustained-release preparations have resulted in small intestinal necrosis with resultant 9. Magnesium hydroxide and have provided the iron siderophore complex 98 growth factor needed by the bacteria to induce calcium carbonate containing antacids may safely be used in therapeutic doses to help reduce iron absorption. Obtain serum iron levels, creatinine, electrolytes, blood Visual Toxicity: Continuous intravenous haemoglobin concentration, blood prothrombin time, base administration of desferrioxamine, often in line liver function tests, and arterial blood gases in seriously the presence of low iron stores, has produced poisoned patients. Chelation can be done either with desferrioxamine factors include desferrioxamine dose, duration (parenteral) or deferiprone (oral). Infusion rates up to 35 mg/ several days for acute and chronic iron overload kg/hr have been used in children with severe patients. Pain and induration at the injection site study has suggested that intravenous desferriox are often experienced. At present, a safe administration venous or intramuscular daily dose should not rate has not been established and is based on generally exceed 6 grams. Liver transplantation is the only therapeutic avenue for evidence of recurrent toxicity (hypotension, open in the presence of fulminant hepatic failure. Infusion duration of Autopsy Features greater than 24 hours has been associated with 1. In patients Acute iron poisoning has assumed grave signifcance in recent who demonstrate a colour change, desferriox years and cases of accidental poisoning are being reported amine therapy may be discontinued when the with alarming frequency in young children. It is imperative that public awareness be enterocolitica septicaemia and mucormycosis. In such circumstances desferrioxamine may Introduction of childproof containers would be very effective in minimising inadvertent ingestions by children as demonstrated Y Copper is useful in electroplated coatings and under 99 by the Western experience. Copper is also Copper made into corrosion-resistant plumbing pipes, used in Physical Appearance heating and roofng materials for building construc tion, and has applications in industrial machinery and Copper is a lustrous, ductile, malleable, odourless solid in automobiles.