
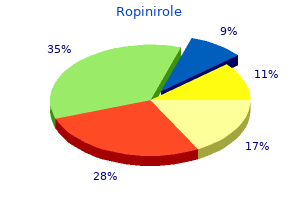
Ropinirole
Safe 0.25 mg ropinirole
Bleeding most comDorling J et al: Feeding growth restricted preterm infants with monly occurs in the subependymal germinal matrix (a abnormal antenatal Doppler results medicine 101 order 0.25 mg ropinirole with mastercard. Anemia in the Premature Infant bleeding (venous infarction in a region rendered ischemic) General Considerations and to periventricular leukomalacia (ischemic white matter injury in a watershed region of arterial supply). The lower nadir in premature infants appears to be the result of decreased erythropoiClinical Findings etin response to the low red cell mass. Symptoms of anemia include poor feeding, lethargy, increased heart rate, poor Up to 50% of hemorrhages occur before 24 hours of age, weight gain, and perhaps periodic breathing. The clinical syndrome ranges from rapid deterioration (coma, hypovenTreatment tilation, decerebrate posturing, fixed pupils, bulging anterior fontanelle, hypotension, acidosis, or acute drop in Transfusion is not indicated in an asymptomatic infant hematocrit), to a more gradual deterioration with more simply because of a low hematocrit. Most infants become subtle neurologic changes, to absence of any specific physisymptomatic if the hematocrit drops below 20%. Promild sequelae in 35% of cases, and no sequelae in 40% of gressive posthemorrhagic hydrocephalus is treated initially cases. When the infant is large enough, this mal bleeds, and progressive ventriculomegaly greatly can be converted to a ventriculoperitoneal shunt. It is important to Although the incidence and severity of intracranial bleednote that extremely low birth weight infants without major ing in premature infants have decreased, strategies to prevent ultrasound findings remain at increased risk for both cerethis complication are still needed. Group: the incidence and course of retinopathy of prematurity: Findings from the early treatment for retinopathy of prematu10. Hospital Discharge Risk of severe retinopathy is greatest in the most Criteria for discharge of the premature infant include mainpreterm infants. Infants going home on suppleExamination evaluates stage of abnormal retinal vasmental oxygen should not desaturate below 80% in room air cular development, extent of retinal detachment, and or should demonstrate the ability to arouse in response to distribution and amount of retina involved. Factors such as support for the mother at home and the stability of the family situation play a role in the timing Retinopathy of prematurity occurs only in the incompletely of discharge. Maternal fever and chorioamnionitis are associated with an Follow-up occurs at 1to 2-week intervals until the retina is increased risk of cerebral palsy. Laser therapy is used in infants with chronic lung disease and reactive airway disease, resulting in progressive disease at risk for retinal detachment. Infants with residual lung disMarlow N et al: Neurologic and developmental disability at six ease are candidates for monthly palivizumab (Synagis) injecyears of age after extremely preterm birth. Comparison with norimmunizations should be given at the appropriate chronomal birth-weight controls. Wilson-Costello D et al: Improved neurodevelopmental outcome for extremely low birth weight infants in 2000-2002. The rate of preterm births in the United States has increased Hack M et al: Behavioral outcomes and evidence of psychopathol31% since 1981. The largest contribution to this increase is ogy among very low birth weight infants at age 20 years. Feeding issues are caused by lack of coordination of suck and swallow, which can interfere with bottle feeding and delay Clinical Findings successful breast feeding, putting the infant at risk for poor Infants with these disorders present with early cyanosis. Related both to feeding issues hallmark of many of these lesions is cyanosis without associand immaturity, these infants have an eightfold increased ated respiratory distress. As a blood flow or secondary to metabolic acidemia from proconsequence, late preterm infants are overrepresented in the gressive hypoxemia. Failure of PaO2 or SaO2 to increase suggests cyanotic ure to thrive are much more common than in term infants. Note: A PaO2, if feasible, is the preferred Late preterm infants should be considered preterm rather measure. Saturation in the newborn may be misleadingly than near term and require close in-hospital monitoring high despite pathologically low PaO2 due to the left-shifted after birth for complications. After nursery discharge, close oxyhemoglobin dissociation curve seen with fetal hemoglooutpatient follow-up is indicated, especially if they are sent bin. Chest radiograph shows a generous heart size and a the National Institute of Child Health and Human Developnarrow mediastinum with normal or increased lung markment. The chest radiograph typically shows a small to normal heart size with marked pulmonary edema. General Considerations Differentially diminished pulses (coarctation) or decreased the causes of cyanotic heart disease in the newborn are pulses throughout (aortic atresia). Newborn infants who present with serious acyanotic heart disease usually have congestive heart failure secondary to left-sided outflow tract obstruction. Other clinical associations include hypothermia, meconium aspiration syndrome, hyaline memClinical Findings brane disease, polycythemia, neonatal sepsis, chronic intraInfants with left-sided outflow obstruction generally do well uterine hypoxia, and pulmonary hypoplasia. On examination, all of these infants have abnormalincrease in pulmonary vascular smooth muscle developities of the pulses. In aortic atresia (hypoplastic left heart ment, often associated with meconium aspiration syndrome; syndrome) and stenosis, pulses are all diminished, whereas and (3) decreased cross-sectional area of the pulmonary in coarctation syndromes, differential pulses (diminished or vascular bed associated with lung hypoplasia (eg, diaphragabsent in the lower extremities) are evident. Treatment of Cyanotic Clinically, the syndrome is characterized by onset on the first & Acyanotic Lesions day of life, usually from birth. Respiratory distress is prominent, and PaO2 is usually poorly responsive to high concenEarly stabilization includes supportive therapy as needed (eg, trations of inspired oxygen. Specific therapy includes infusions of prosdiography reveals right-to-left shunting at the level of the taglandin E1 (0. In some cyanotic lesions (eg, pulmonary atresia, tricusradiograph usually shows lung infiltrates related to associpid atresia, and critical pulmonary stenosis) in which lung ated pulmonary pathology (eg, meconium aspiration and blood flow is ductus-dependent, this improves pulmonary hyaline membrane disease). If the majority of right-to-left blood flow and PaO2 by allowing shunting through the shunting is at the ductal level, preand postductal differences ductus to the pulmonary artery. Neurodevelopmental outcome with problems such as seizures, renal failure, hypoglycemia, and congenital heart disease depends on the lesion, severity of infection. Specific therapy is aimed at both increasing sysneonatal presentation, and complications related to palliatemic arterial pressure and decreasing pulmonary arterial tive and corrective surgery. Other sequelae such as chronic lung disease, sensorineural hearing loss, and feeding Unable to pass an orogastric tube to the stomach. In mature ventricular contractions, are common in the first 85% of infants, the fistula is between the distal esophagus days of life in well newborns. Heart block can be seen in an otherwise structurally normal heart (associated with Clinical Findings maternal lupus) or with structural cardiac abnormalities. In Infants present in the first hours of life with copious secrethe absence of fetal hydrops, the bradyarrhythmia is often tions, choking, cyanosis, and respiratory distress. Cardiac pacing may be required if there are confirmed with chest radiograph after careful placement of a symptoms of inadequate cardiac output. If a (ventricular tachycardia) or narrow complex (supraventricutracheoesophageal fistula is present to the distal esophagus, gas lar tachycardia). In esophageal atresia without common neonatal tachyarrhythmia and may be a sign of tracheoesophageal fistula, there is no gas in the bowel. Digoxin the head of the bed should be elevated to prevent reflux of gastric should not be used in infants with Wolff-Parkinson-White contents through the distal fistula into the lungs.
Discount 0.25 mg ropinirole mastercard
Effective 2006 medications used for depression purchase discount ropinirole on-line, providers submit electronic attachments with electory of the Great Plains Regional Medical Center, a managed care system started in 1929. Icons draw attention to critical areas of confi Kaiser Permanente your knowledge at various Go to Most managed care financing is achieved through a method called capitation, and enrollees are B. He has past history of hypertension, controlled by mediManaged care is categorized according to six models: exclusive provider organizations, cation, and new complaints of dizziness and tiredness. During integrated delivery systems, health maintenance organizations, point-of-service plans, preferred provider organizations, and triple option plans. Procedures Diagnoses serves as a review aid when preparing for tests. Which means that the patient and/or insured has authorized the payer to reimburse the providernegative and the procedure was performed uneventfully. If the patient is unemployed and/or not a fullor part-time student, leave blank. A series of fixed-length records submitted to payers to bill for health care services is an electronic: 9, Leave blank. These instructions are providedDo not enter hyphens or spaces in the policy the Reviews test student understanding about chapor group number. Because in the real world there are many rules that can vary by payer, facility, and state, every effort was made to make the SimClaim program generically correct in order to provide you with a foundational understanding of the claim form. How toAccess SimClaim To access the SimClaim student practice software program online, please refer to the information on the printed access card found in the front of this textbook. Main Menu From the Main Menu, you can access the SimClaim program three different ways: Study Mode, Test Mode, and Blank Form Mode. If you need help entering information in a block of the form, you may click on Block Help for block-specific instructions while in Study Mode. You can access SimClaim support documentation from the Main Menu as well, including a video Tutorial, Block Help, a glossary, and list of abbreviations. When you open the software, enter your first and last name so the software can track your quiz results. Then choose a content area from the menu to take a quiz, complete an activity, or complete a coding case. Quizzes Quizzes include multiple choice, true/false, and fill-in-the-blank questions. Instant feedback tells you whether you are right or wrong and helps you learn quickly by explaining why an answer is correct or incorrect. In Quiz Mode, you have one try to get the answers right, but you can take each quiz as many times as you want. This software can be used to assign codes to any of the coding exercises in the Understanding Health Insurance textbook. Simply mouse over a button to view its title, and a brief description of the button will also appear in the status bar (bottom left corner of screen). Step 1 Retrieve the Encoder Pro disk from the cardboard sleeve inside the back cover of your textbook. Step 7 fi Click on the icons in the gray toolbar to view additional content and instructions about code 425. Individuals who understand claims processing and billing regulations, possess accurate coding skills, can successfully appeal underpaid or Note: Reimbursement denied insurance claims, and demonstrate workplace professionalism, specialist is another title for health insurance specialist. A review of medical office personnel help-wanted advertisements indicates the need for individuals with all of these skills. A health insurance claim is the documentation submitted to a third-party payer or government program requesting reimbursement for healthcare services provided. In the past few years, many practices have increased the number of employees assigned to some aspect of claims processing. This increase is a result of more patients having some form of health insurance, many of whom require preauthorization (prior approval) for treatment by specialists and documentation of post-treatment reports. If the insurance plan has a hold harmless clause (patient is not responsible for paying what the insurance plan denies) in the contract, the healthcare provider cannot collect the fees from the patient. Competitive insurance companies are fine-tuning procedures to reduce administrative costs and overall expenditures. This cost-reduction campaign forces closer scrutiny of the entire claims process, which in turn increases the time and effort medical practices must devote to billing and filing claims according to the insurance policy filing requirements. Poor attention to claims requirements will result in lower reimbursement rates to the practices and increased expenses. Each insurance plan has its own authorization requirements, billing deadlines, claims requirements, and list of participating providers or networks. If a healthcare provider has signed 10 participating contracts, there are 10 different sets of requirements to follow and 10 different panels of participating healthcare providers from which referrals can be made. Rules associated with health insurance processing (especially government programs) change frequently; to remain up-to-date, insurance specialists should be sure they are on mailing lists to receive newsletters from third-party payers. Employers renegotiate benefits with existing plans or change third-party payers altogether. The employees often receive retroactive notice of these contract changes and, in some cases, once notified may have to wait several weeks before new health benefit booklets and new insurance identification cards are issued. Health insurance specialists (or reimbursement specialists) review health-related claims to determine the medical necessity for procedures or services performed before payment (reimbursement) is made to the provider. A claims examiner employed Note: Health insurance speby a third-party payer reviews health-related claims to determine whether the cialists and medical assistants charges are reasonable and for medical necessity. When employed by clearinghouses, insurance to an investigator for a more thorough review. Medical billing and insurance verification specialists in healthcare organizations. Note: On December 31, fi Writers and editors of health insurance textbooks, newsletters, and other publications.
Buy 0.25mg ropinirole amex
Patient started on an empiric course of Pen Vee K 250 mg #40 to be taken qid * 10 days 3 medicine zofran 2mg ropinirole with amex. Patient to call office in 48 hours to obtain culture results and report her progress. S: this is a 50-year-old widow who comes to the office following a possible seizure. Her friend reports she was seated at her desk, and after a crash was heard, they found her lying on the floor. Patient says this was her first episode and denies ever having chest pain, palpitations, or paresthesias. She reports no hospitalizations except for normal delivery of her son 25 years ago. Patient seems to be doing fine, thinks the bleeding has just about stopped at this point. Her daughter is apparently doing fine; she is to get back chromosomal analysis in a couple of days. Entire squamocolumnar junction could not be visualized even with aid of endocervical speculum. Exam was made more difficult because of very thick cervical mucus, which could not be completely removed, and because the vagina and cervix were somewhat atrophic appearing. Whitening of epithelium around entire circumference of cervix noted, but no abnormal vasculature noted. Patient told she could have intercourse after five days, to use condoms, or to come back to office first to have size of diaphragm checked. X-rays revealed a good reduction; therefore, a plaster splint was applied, care being taken not to put any constriction in the antecubital fossa. Patient maintained good radial pulse, was awake, and was taken to Recovery in good condition. Additional procedures documented in the body of the report that are not listed in the heading of the report. The surgeon also documents the operative findings and a biopsy of a suspicious liver nodule. When the Procedures Performed heading lists procedures performed that are not described in the body of the operative report, the surgeon will have to add a written addendum to the operative report documenting the performance of any listed procedure that should be coded. Open repair, right knee, collateral and cruciate ligaments Upon review of the body of the report, the insurance specialist notes that the surgeon did not document removal of the scope. Even though the removal of a scope is not coded, the insurance specialist should instruct the surgeon to document this as an addendum to the operative report. Many coding errors are made when the coder does not understand critical medical terms in the report. Global surgery includes preoperative assessment, the surgery, and normal uncomplicated postoperative care. Preoperative diagnosis is appendicitis, and the patient undergoes appendectomy; however, the postoperative diagnosis is normal appendix. Look for additional findings in the body of the report if the postoperative diagnosis listed on the operative report does not completely justify the medical necessity for the procedure. Compare the postoperative diagnosis with the biopsy report on all excised neoplasms to determine whether the tissue is benign or malignant. When doing the exercises in this text and the Workbook, use any stated pathology report to determine whether excised tissue is benign or malignant if it is not covered in the postoperative diagnosis(es). When working in a medical practice, do not code an excision until the pathology report is received. ExErcisE 10-6 Coding Operative Reports When working with the case studies in this text, code procedures as listed in the case. Procedure: the patient was placed in the dorsal recumbent position and draped in the usual fashion. The skin and subcutaneous tissues at the junction of the skin grafts of the previous excision and the normal scalp were infiltrated with 1/2% xylocaine containing epinephrine. After hemostasis was obtained, the entire area of granulating tissue was thoroughly electrodesiccated. Resected piece of skin shows partial loss of epithelium accompanied by acute and chronic inflammation of granulation tissue from a previous excision of basal cell carcinoma. The pathology report indicated atypical melanocyte cells in the area close to the margin of the excision. The patient was informed of the situation during an office visit last week, and he agreed to be readmitted for a wider excision of the tumor area. Procedure: the patient was placed on his left side, and general anesthesia was administered. The frozen section was reported as negative for melanocytes on the excisional margin at this time. After the report was received, the wound was closed in layers and a dressing was applied. The patient tolerated the procedure well and was sent to Recovery in good condition. The ascending colon, transverse colon, and proximal descending colon appeared unremarkable. There were two polyps which were about 8 mm in size adjacent to each other in the sigmoid colon. One was removed for biopsy, and the other was fulgurated with hot wire biopsy forceps. Because of the suboptimal prep, small polyps or arteriovenous malformations could have been missed. A large amount of thick fluid was aspirated from both ears, more so from the left side. Patient tolerated the procedure well and was sent to Recovery in satisfactory condition. After application of 1% xylocaine with 1:1000 epinephrine, the lesion was completely excised. The patient tolerated the procedure well and returned to the Outpatient Surgery Unit in satisfactory condition. After sterile prepping and draping, 40 cc of 1/2% xylocaine was infiltrated into the surrounding tissue of the pilonidal cyst that had a surface opening on the median raphe over the sacrum. Next, a scalpel was used to make an approximately 8 * 8 cm elliptical incision around the pilonidal cyst. The incision was carried down through subcutaneous tissue to the fascia and the tissue was then excised. Estimated blood loss was minimal, and the patient received 550 cc of crystalloid intraoperatively. The patient tolerated the procedure well and was sent to the Recovery Room in stable condition. Initially, the patient was placed in the supine position, and the abdomen was prepped and draped with Betadine in the appropriate manner. An oblique skin incision was performed from the anterior superior iliac spine to the pubic tubercle. Dissection was carried down until the external oblique was divided in the line of its fibers with care taken to identify the ilioinguinal nerve to avoid injury.
Generic ropinirole 2mg visa
A monohybrid cross results in a 9:3:3:1 ratio whereas a dihybrid cross gives a 3:1 ratio treatment resistant schizophrenia purchase ropinirole in india. A cross between homozygous purple-flowered and homozygous white-flowered pea plants results in offspring with purple flowers. What was the most significant conclusion that Gregor Mendel drew from his experiments with pea plantsfi Two plants are crossed, resulting in offspring with a 3:1 ratio for a particular trait. Two characters that appear in a 9:3:3:1 ratio in the generation should have which of the following propertiesfi A sexually reproducing animal has two unlinked genes, one for head shape (H) and one for tail length (T). It was important that Mendel examined not just the generation in his breeding experiments, but the generation as well, because a. When crossing an organism that is homozygous recessive for a single trait with a heterozygote, what is the chance of producing an offspring with the homozygous recessive phenotypefi Plants with at least one allele D have dark green leaves, and plants with the homozygous recessive dd genotype have light green leaves. A true-breeding dark-leaved plant is crossed with a light-leaved one, and the offspring is allowed to self-pollinate. The predicted outcome of the is diagrammed in the Punnett square shown in Figure 14. Mendel accounted for the observation that traits which had disappeared in the generation reappeared in the generation by proposing that a. It states that each of two alleles for a given trait segregate into different gametes. It can be used to predict the likelihood of transmission of certain genetic diseases within families. It is a method that can be used to determine the number of chromosomes in a plant. The fact that all seven of the pea plant traits studied by Mendel obeyed the principle of independent assortment most probably indicates which of the followingfi All of the genes controlling the traits behaved as if they were on different chromosomes. Mendel was able to draw his ideas of segregation and independent assortment because of the influence of which of the followingfi The understanding of particulate inheritance he learned from renowned scientists of his time c. If a heterozygous plant is crossed with a homozygous tall plant, what is the probability that the offspring will be shortfi One parent has red, axial flowers and the other has white, terminal flowers; all individuals have red, axial flowers. If 1,000 offspring resulted from the cross, approximately how many of them would you expect to have red, terminal flowersfi What proportion of the progeny will be expected to phenotypically resemble the first parentfi In a cross of a black female with a brown male, results can be either all black puppies, 1/2 black to 1/2 brown puppies, or 3/4 black to 1/4 yellow puppies. In one type cross of black fi black, the results were as follows: 9/16 black 4/16 yellow 3/16 brown the genotype aabb must result in which of the followingfi A cross between a red-flowered plant and a whiteflowered plant yields all-purple offspring. The part of the radish we eat may be oval or long, with long being the dominant characteristic. In the generation of the above cross, which of the following phenotypic ratios would be expectedfi Drosophila (fruit flies) usually have long wings (+) but mutations in two different genes can result in bent wings (bt) or vestigial wings (vg). If a homozygous bent wing fly is mated with a homozygous vestigial wing fly, which of the following offspring would you expectfi In snapdragons, heterozygotes for one of the genes have pink flowers, whereas homozygotes have red or white flowers. When plants with red flowers are crossed with plants with white flowers, what proportion of the offspring will have pink flowersfi Tallness (T) in snapdragons is dominant to dwarfness (t), while red (R) flower color is dominant to white (r). A dwarf, red snapdragon is crossed with a plant homozygous for tallness and white flowers. Skin color in a certain species of fish is inherited via a single gene with four different alleles. Which of the following crosses would produce offspring in the ratio of 1 red: 2 roan: 1 whitefi Cactuses with the dominant allele, S, have sharp spines, whereas homozygous recessive ss cactuses have dull spines. Feather color in budgies is determined by two different genes Y and B, one for pigment on the outside and one for the inside of the feather. A woman who has blood type A positive has a daughter who is type O positive and a son who is type B negative. Rh positive is a trait that shows simple dominance over Rh negative and is designated by the alleles R and r, respectively. Which of the following terms best describes when the phenotype of the heterozygote differs from the phenotypes of both homozygotesfi Cystic fibrosis affects the lungs, the pancreas, the digestive system, and other organs, resulting in symptoms ranging from breathing difficulties to recurrent infections. In rabbits and many other mammals, one genotype (cc) prevents any fur color from developing. In Drosophila (fruit flies), white eyes can be due to an X-linked gene or to a combination of other genes. If one parent has the disease, what is the probability that his or her child will have the diseasefi An ideal procedure for fetal testing in humans would have which of the following featuresfi This and only this allele, if homozygous, produces an effect that results in death at or about the time of birth. An obstetrician knows that one of her patients is a pregnant woman whose fetus is at risk for a serious disorder that is detectable biochemically in fetal cells. The obstetrician would most reasonably offer which of the following procedures to her patientfi The frequency of heterozygosity for the sickle cell anemia allele is unusually high, presumably because this reduces the frequency of malaria. The probability of their next child being normal for this characteristic is which of the followingfi Regulate the diet of the affected persons to severely limit the uptake of the amino acid. Hutchinson-Gilford progeria is an exceedingly rare human genetic disorder in which there is very early senility, and death, usually of coronary artery disease, at an average age of approximately 13. All cases must occur in relatives; therefore, there must be only one mutant allele. Successive generations of a family will continue to have more and more cases over time. Each patient will have had at least one affected family member in a previous generation. If a young child is the first in her family to be diagnosed, which of the following is the best explanationfi Why did the improvement of microscopy techniques in the late 1800s set the stage for the emergence of modern geneticsfi It allowed the study of meiosis and mitosis, revealing parallels between behaviors of genes and chromosomes. When Thomas Hunt Morgan crossed his red-eyed generation flies to each other, the generation included both redand white-eyed flies. Sturtevant provided genetic evidence for the existence of four pairs of chromosomes in Drosophila in which of these waysfi X chromosomes in males generally have more mutations than X chromosomes in females.
Generic 2 mg ropinirole mastercard
A large fraction of the metabolites was recovered from the epithelial surface medicine nelly cheap ropinirole line, indicating that benzo[a]pyrene was first absorbed in the mucosa, metabolized, and returned to the mucus. Monkeys and dogs received nasal instillation of 14 [ C]-benzo[a]pyrene at doses of 0. Radiolabeled metabolites were detected in the nasal cavity, but little or no activity was detected in the blood and excreta of either species during the 48 hours after exposure. These results indicate that absorption of benzo[a]pyrene and/or its metabolites was poor or very slow following nasal instillation in monkeys and dogs. Following ingestion of diets containing very low levels of benzo[a]pyrene, the metabolite, 1-hydroxypyrene, was detected in the urine (Buckley and Lioy 1992). The feces of these individuals did not contain detectable levels of benzo[a]pyrene (<0. Oral absorption of benzo[a]pyrene in rats is incomplete and may be influenced by the presence of oils and fat in the gastrointestinal tract. Oral absorption of benzo[a]pyrene was estimated to be 40%, with a bioavailability of 7. Radioactivity found in the liver, lungs, kidneys, and testis following a low dose of 3 [ H]-benzo[a]pyrene to Sprague-Dawley rats provides supporting evidence of oral absorption (Yamazaki and Kakiuchi 1989; Yamazaki et al. The extent of oral absorption in rats is enhanced when benzo[a]pyrene is solubilized in a vehicle (triolein, soybean oils, high-fat diet) that is readily absorbed following lowand high-dose levels (Kawamura et al. Oral absorption of benzo[a]pyrene was estimated to be 38-58% following dietary or gavage exposure to high levels in rats (Chang 1943). Anthracene was absorbed to a slightly higher extent (53-74%) than benzo[a]pyrene in rats while phenanthracene was poorly absorbed (4-7%) (Chang 1943). However, the data were limited because an inadequate number of rats was used and study details were lacking. In general, the oral absorption of chrysene, dibenzanthracene, and pyrene was high following exposure to high doses in rats (Chang 1943; Grimmer et al. Following dietary or gavage administration of chrysene in rats, 64-87% of the dose was excreted in the feces (Chang 1943). Recovery of chrysene in excreta of Wistar rats was 74% four days after a single gavage dose of 22 mg/kg chrysene in corn oil (Grimmer et al. Administration of dibenz[a,h]anthracene in the diet (250 mg) or by stomach tube (200 mg) resulted in more than 90% of the dose being excreted in the feces of white rats (Chang 1943). Male Wistar rats administered 2-15 mg/kg of [ C]-pyrene recovered 68-92% of the dose in the excreta by 6 days postexposure (Withey et al. Bioavailability of pyrene and its metabolites was 65-84% over a period of 8 hours following administration. Fluoranthene, pyrene, or benz[a]anthracene in Tween 80/isotonic saline, was administered orally to rats at a dose of 20 mg/kg. Blood levels after administration indicated that peak concentrations of the three compounds were reached at 1-2 hours after 3 administration. The peak concentration of fluoranthene (fi30 mg/cm) was twice as high as that of pyrene, and 5 times higher than benz[a]anthracene. The mixtures contained pyrene, benz[a]anthracene, chrysene, benzo[b]fluorene, benzo[k]fluorene, benzo[a]pyrene, indeno[ 1,2,3-cd]pyrene, dibenz[a,h]anthracene, benzo[g,h,i]perylene. Urine was collected on the first, seventh, and fourteenth day of diet administration. The efficiencies of absorption without bile (as a percentage of absorption with bile) were benzo[a]pyrene, 22. This difference correlated with a difference in water solubility, with anthracene being 18 times less water-soluble than phenanthrene. Those products with low water solubility are dependent on the creation of an intermediate phase of the products of lipolysis and bile salts (Rahman et al. These reactions occur during the normal process of lipid digestion and absorption in the intestine. Phenanthrene, anthracene, pyrene, and fluoranthene were detected in the blood, but benzo[a]pyrene (which is present in coal tar) was not detected. This difference was attributed to differences in percutaneous absorption, rapid tissue deposition after absorption, or metabolic conjugation with rapid urine excretion. In another study, coal tar ointment was applied to skin of volunteers at various sites (Van Rooij et al. Twelve workers from a coke plant participated in an intensive skin monitoring program combined with personal air sampling and biological monitoring during 5 consecutive 8-hour shifts (Van Rooij et al. The mean concentration of total pyrene in the breathing zone 3 air of the 12 workers ranged from 0. Analysis indicated that dermal absorption was most important in contributing to 1-hydroxy-pyrene excretion. Of the total dose absorbed by both routes combined, 13-49% is excreted as 1-hydroxy-pyrene. Variation in excretion is influenced by smoking habits, and consumption of alcohol. Approximately 73% of the administered dose was absorbed dermally by 7 days postexposure; most of the dose was absorbed by day 3. In vitro absorption of benzo[a]pyrene through guinea pig skin demonstrated similar results; 67% absorption in a 24-hour 2 exposure (Ng et al. The site of application still retained 7% of the recovered radioactivity after 7 days. However, the area of application was not covered to prevent animals from licking the test material which may have lead to ingestion of benzo[a]pyrene. Three animals in each dose group were killed at 1,2,4, and 6 days postdosing, and the brain, lungs, heart, liver, spleen, kidneys, testes, muscle, and 14 perirenal fat were removed and analyzed for pyrene and [ C]-pyrene equivalents. Blood, urine, and feces, as well as the skin from the application site were also analyzed. Dermal absorption of benzo[a]pyrene in rats and monkeys may be affected by the vehicle of administration (Wester et al. The great variation in the absorption with the acetone vehicle limits these results. This may be related, in part, to the dependence on monitoring radioactivity recovered in urine only as opposed to monitoring radioactivity recovered in urine and feces. Disappearance of the applied dose from the application site was 40% at 24 hours following administration (Wester et al. Sprague-Dawley rats absorbed 4-5 times more of a 1 ppm dose of benzo[a]pyrene when it was applied dermally alone, compared to a soil-sorbed crude oil mixture (Yang et al. Benzo[a]pyrene (10 ppm) with acetone vehicle or in soil 2 was applied to a 12 cm area of abdominal skin of female rhesus monkeys for 24 hours (Wester et al. Over time, the permeation of anthracene significantly decreased suggesting that anthracene was dermally absorbed in a dose-dependent manner. In vitro absorption of phenanthrene and pyrene in guinea pig skin was about 79-89% and 70%, respectively (Ng et al. The disappearance of radiolabeled benzo[a]pyrene and its metabolites from the epidermis was monophasic, following first order kinetics with a half-life of approximately 2 hours (Melikian et al. Recovery of the radiolabel was 99-100% throughout the period of the experiment (8 hours), indicating that volatilization of benzo[a]pyrene from the skin was not a confounding factor (Melikan et al.
Discount ropinirole 0.25 mg with amex
The trainee will learn the up-to-date classifications of neoplastic lesions and the various non-neoplastic lesions and pitfalls symptoms 4 days after conception cheap 1mg ropinirole. At the completion of training, the resident will: fi Understand normal histology of various solid lymphoreticular organs including lymph nodes, the spleen, bone marrow, and the thymus. Communicator fi the resident should be able to communicate effectively with medical colleagues including technologists, oncologists, radiologists, and coordinators. Collaborator fi the resident should contribute effectively to interdisciplinary team activities by participating in interdisciplinary rounds or research activities. Effectively and efficiently make use of the limited diagnostic material available to make a definitive diagnosis and convey the result in a clear and timely manner. Health Advocate fi the resident promotes the technological advances that play an important role in lymphoma diagnosis and strives to introduce relevant new technologies locally. Scholar fi the resident is committed to a personal continuing educational strategy to keep up to date with new classifications, diagnostic criteria, and developments. Professional fi the resident delivers care of the highest quality with integrity, honesty, and compassion. Autopsy Rotation Postmortem pathology Postmortem pathology is a subspecialty of anatomic pathology that focuses on the diagnosis, management, and prevention of disease, trauma, and poisoning of the human body at the postmortem phase. The role of the pathologist incorporates the formulation of an opinion regarding the identification, cause, and manner of human death, taking into consideration the history and autopsy findings with a possible medicolegal scope. Evaluation fi Daily evaluation should be conducted by a host-institute consultant present at the autopsy. Clinical competencies Medical Expert fi the resident should understand the history of postmortem pathology in Saudi Arabia. Communicator fi the resident should be able to establish a professional bond with the family of the deceased and with the community. Collaborator fi the resident should reveal effective skills to participate in a professional environment as part of a multidisciplinary team with the shared goal of postmortem human care management. Manager fi the resident should demonstrate understanding of and familiarity with the management structure of both the authorizing body and the laboratory as well as the relationship between them. Health Advocate fi the resident should understand and demonstrate the role of the pathologist in providing accurate information pertaining to public health issues, particularly related to injury, poisons, and disease (infectious disease, hereditary disease, environmentand occupation-related injury and disease, death patterns, mass fatalities, custody deaths, judicial deaths, perinatal and infancy deaths, maternal deaths, deaths due to a specific disease, etc. However, forensic rotation for one month within the Kingdom is mandatory and is to be organized by the chair of the local committee. Note: Each supervisor should ensure that all R5 residents have done this rotation during their senior years (Years 3, 4, and 5) before the exit exam. Objectives fi To gain an understanding of basic molecular biology techniques in molecular pathology fi To grasp comprehensive knowledge of principles and concepts of the molecular basis of disease by this stage; the rotation will aim to reinforce the clinical use of this knowledge. Communicator fi the resident should take the opportunity to educate colleagues and members of the multidisciplinary team during clinicopathological conferences and presentations on issues related to genetics, molecular biology, and genomics. Collaborator fi the resident should communicate with requesting physicians to advise them on the appropriate use of molecular diagnostic and cytogenetic methods. Health Advocate fi the resident should engage health professionals and the medical community in determining appropriate laboratory use of molecular testing to advance health care. Scholar fi the resident should be committed to a personal strategy of continuing education. Professional fi the resident should deliver the highest standard of care with integrity, honesty, and compassion and should execute duties in an ethical manner and with sensitivity to a diverse patient population. During this rotation, the resident should be able to create and initiate a minimum of two research ideas and to conduct research projects during his/her training years. Communicator fi Upon conclusion of the project, the resident should present it as grand rounds or during an academic or research day. Collaborator the resident should be able to work with other team members from different specialties on a combined project. Manager the resident should understand the cost of research and be able to set a budget plan. Scholar fi the resident should compare his/her data to those previously collected and determine differences. Other Subspecialty Rotations these rotations might be incorporated into the surgical pathology rotations or be taken as separate rotations, depending on the hospital in which the resident is rotating. During each rotation, the resident will gain unique experience in patient diagnosis and care in regard to diagnostic pathology. Please refer to the section on teaching and academic activity for further details and guidelines for conducting a journal club presentation. Internal Educational Material Mandatory Activities Each institution is requested to provide or allow the resident to attend the following educational activities that are arranged by the local committees: For R1 Residents: Basic Pathology and Histotechnology (eight weeks) For All Residents (venue to be announced for each session): fi Academic Half Day (twice a month) Presently bi-monthly and in some regions once weekly, at least four to six hours of formal training time should be reserved for resident academic half day. Formal teaching time is planned in advance with an assigned tutor, time slots, and a venue. A master-list for suggested and recommended academic half-day lectures is provided in Appendix B. The lectures will be scheduled throughout two years and will be repeated every two years. A schedule for the current academic year with the venue and speaker should be provided at the beginning of every academic year. Journal clubs Guidelines for Anatomic Pathology Journal Club Goals of Journal Club: fi Teach critical appraisal fi Keep current with the medical literature fi Provide a foundation for evidencefibased practice fi Review landmark or controversial papers Characteristics of successful journal clubs fi Presented by residents or fellows and actively supervised by staff fi Attendance is mandatory o Residents and fellows fi Meetings last for less than 60 minutes o Protected time (preferably pager off! Purpose fi Research question, study objective, and specific hypothesis: fi Do the authors provide a clear and specific question and hypothesisfi Optional Activities fi Each institution must encourage the following educational activities: fi the resident is encouraged to present at least once a year at the local, national, or international pathology meeting. Continuous Appraisal this assessment is conducted toward the end of each training rotation throughout the academic year and at the end of each academic year as continuous assessment in the form of formative and summative evaluation. The assessment tools, in the form of a logbook, are assessed at the end of each year by the chairs of the local committees (Appendix E). Academic and clinical assignments should be documented on an annual basis using the electronic logbook (when applicable). Evaluations will be based on accomplishment of the minimum requirements for the procedures and clinical skills, as determined by the program. End-of-year Examination the end-of-year examination will be limited to R1, R2, R3, and R4. Examination details such as dates of the exam and the blueprint are published on the commission Website, The reason for taking this exam is for the resident to judge his/her progress among peers on an internationally standardized exam. It will provide a benchmark for the trainers and guide the program directors on how to improve the program. In addition, there will be a practical exam with slides for long and short cases and a computerbased exam. Examination details such as dates of the exam and a blueprint are published on the commission Website: This report may also involve clinical examinations, oral examinations, or other academic assignments. Examination details such as dates of the exam and a blueprint are published on the Commission Web site: Practical and Oral Examination this examination assesses a broad range of high-level clinical and diagnostic skills.
Buy ropinirole pills in toronto
Therefore symptoms zoning out buy cheap ropinirole 2 mg online, special caution and parental chromosome, allowing the chromosomes to be identified. Using different staining techniques, different banding patterns result: G, Q, and R banding. There are many different kinds of probes, arm, and q, the letter following p, refers to the long arm. Chromosomal Abnormalities There are two types of chromosomal anomalies: numerical Array-Based Comparative and structural. Abnormalities of Chromosomal Number Advances in computer chip technology have led to the development of new genetic testing using comparative When a human cell has 23 chromosomes, such as human ova genomic hybridization with microarray technique. After conception, in cells technique allows detection of very small genetic imbalances other than the reproductive cells, 46 chromosomes are present anywhere in the genome. Polyploid cells are those that been used to detect interstitial and subtelomeric submicrocontain any number other than the usual diploid number of scopic imbalances, to characterize their size at the molecular chromosomes. Polyploid conceptions are usually not viable level, and to define the breakpoints of translocations. It results from unequal division, called nondisjunction, of which are used more widely in research settings. Detailed nomenclature, such as 8q11, is required to further demonstrate a specific missing region so B. Examples of structural chromosomal abnormalities: deletion, duplication, inversion, ring chromosome, translocation, and insertion. Mosaicism should be suspected if clinical symptoms are short arm of chromosome 1, which results in 1p36. The prognosis is frequently better for handicaps and characteristic facial features. A well-described patient with chromosomal mosaicism can seldom be assessed duplication of chromosome 22q11 causes cat eye syndrome, reliably based on the karyotype in peripheral blood alone. It can be paracentric (not involving the centromere) or pericentric Under normal circumstances, one member of each homolo(involving the centromere). Ring chromosomal anomalies often both homologous chromosomes of that parent will be cause growth retardation and mental handicap. This requires homozygosity for deleterious recessive genes and the consethree breakpoints and may occur between two chromosomes quences of imprinting (see later discussion in the Imprinting or within the same chromosome. Sex Chromosomal Anomalies somes, including chromosomes 7, 11, 15, and X, and has been found in patients with Prader-Willi, Angelman, and Abnormalities involving sex chromosomes, including aneuBeckwith-Wiedemann syndromes. In addition, cystic fibroploidy and mosaicism, are relatively common in the general sis with only one carrier parent (caused by maternal isodipopulation. Mosaicism Contiguous gene syndromes result when a deletion causes Mosaicism is the presence of two or more different chromothe loss of genes adjacent to each other on a chromosome. The assortment of homologous chromosomes during normal gametogenesis and uniparental disomy. Examples of common presence is necessary for initiation of the cancer; an example contiguous gene syndromes. Secondary abnormalities appear de novo in somatic cells only after the cancer has developed, Abnormal Chromosome for example, Philadelphia chromosome, t(9;22)(q34;q11), in Syndrome Segment acute and chronic myeloid leukemia. Primary and secondary Prader-Willi/Angelman syndrome del 15q11 chromosomal abnormalities are specific for particular neoShprintzen/DiGeorge spectrum del 22q11 plasms and can be used for diagnosis or prognosis. For example, the presence of the Philadelphia chromosome is a Miller-Dieker syndrome del 17p13 good prognostic sign in chronic myelogenous leukemia and Wilms tumor with aniridia, genitourinary del 11p13 indicates a poor prognosis in acute lymphoblastic leukemia. Chromosome Fragility genetics, as they allow for the localization, isolation, and It is well known that environmental factors such as exposure characterization of genes that encode protein sequences. As to radiation, certain chemicals, and viruses contribute to the Human Genome Project has moved into the postchromosome breaks and rearrangements. These are called chromocomplex underlying biology involved in many human some instability or breakage syndromes. Western blot analysis is used to pigmentary changes, mild mental retardation, and devellook for protein changes. Assessment of chromosome breaks and sister chromatid exchanges Molecular Biology in Clinical requires special techniques that lead to enhancement of the Genetics & Genetic Diagnosis breaks, or special staining that allows visualization of the Genetic diagnosis can be performed by direct detection of a exchanged chromatids. A normal gene introduced into an individual affected Indirect detection of abnormal genes is used when the with a serious inherited disorder during embryonic life gene is known but there is extensive heterogeneity of the (germline therapy) in principle has the potential to be transmolecular defect between families, or when the gene responmitted to future generations, whereas its introduction into sible for a disease is unknown but its chromosome location somatic cells (somatic therapy) affects only the recipient. Experimental gene therapy by bone marrow transplantation One form of indirect analysis is the linkage method. RecombiLinkage traces the inheritance of the abnormal gene between nant enzyme replacement has been successfully applied in members in a kindred. This method requires that the aftreating the non-neurologic form of Gaucher disease, Fabry fected individual be studied, as well as parents and other disease, Pompe disease, mucopolysaccharidosis types I and relatives, both affected and unaffected. They are also used rize, the inheritance of genetic traits through generations increasingly to identify gene changes in tumors. SegregaNeurofibromatosis is an example of a disorder in which tion is the process through which gene pairs are separated both the direct and indirect assay may be used. Man, lists more than 10,000 entries in which the mode of inheritance is presumed to be autosomal dominant, autosoMolecular Biology in Prevention mal recessive, X-linked dominant, X-linked recessive, and Y& Treatment of Human Diseases linked. Single genes at specific loci on one or a pair of chromosomes cause these disorders. Analysis of the pedigree and the pattern of transdefective genes and permitting prenatal diagnosis. For example, differentiation of gonadal mosaicism from decreased penetrance of a dominant gene Terminology has important implications for genetic counseling. In the past, the diagnosis of a genetic disease characterized by late the following terms are important in understanding heredonset of symptoms (eg, Huntington disease) could not be ity patterns. It may be one phenotype is caused by different allelic mutations at a modified by environment.
Order 0.5mg ropinirole with mastercard
Alternatively medications 101 purchase ropinirole master card, use should be encouraged to consider or choose a second method of a pill with lower or no estrogen. These strains have a variety of virulence factors, including adhesive fimbriae, which allow these bacteria to adhere to the uroepithelium and resist the flushing action of urine flow. Infections usually Dysuria is pain or discomfort associated with urination that is remain within the bladder but bacteria sometimes ascend localized to the bladder or urethra. Approximately the renal parenchyma becomes infected, the infection is called 3% of all office visits are in response to this symptom (2,3). Infections within the urinary tract are only patients with dysuria are otherwise healthy women who have rarely caused by a bloodborne source. Other causes of divided into four very broad categories: (i) acute uncomplidysuria are listed in Table 27. The diagnosis of urethral syndrome is made only after the symptomatic patient has had normal findings on physical Pathophysiology examination, and normal urinalysis and culture. During the third and fourth empiric therapy to have a high probability of success. For example, 10% to 20% of women have an and depends largely on the clinical setting. Another high-risk group is women with colonization of the vagina by uropathogens. Fecal incontiWhen a healthy adult woman complains of moderately severe nence and stasis of urine in the bladder are risk factors in both dysuria and nocturia, there is about a 65% probability that men and women. A simple scoring system for evaluating symptoms, history and urine dipstick testing in the diagnosis of urinary tract infection. Prevalence and diagnosis of chlamydial infection and evaluation of rapid screening of bacteriuria. Developing clinical rules to predict urinary tract infection in primary care settings: sensitivity and specificity of near patient tests (dipsticks) and clinical scores. Tenderness over a flank or in the midabdomen sugFever and dysuria can be from conditions other than gests upper tract disease; however, suprapubic tenderness with pyelonephritis. For example acute prostatitis or genital herpes an uncomplicated lower tract infection is common. Similarly, the lack of upper the penis should be gently milked to elicit a urethral discharge, tract symptoms such as fever and flank pain does not eliminate and a rectal exam performed to feel for a tender or boggy the possibility of infection of the upper urinary tract. You should perform a vaginal these infections include dysuria for more than 7 days, an examination on women who report vaginal discharge or irriimmunosuppressing condition, prior episode of acute tation (see Chapter 33). Giving the patient thorough instructions about cleansing the urethra and genitalia has been stressed, but controlled studies have not demonstrated any advantage to this practice (12). The dipstick, trifuging a 10-mL tube of freshly voided urine, decanting the which detects blood, nitrite, and leukocyte esterase in the urine, and then resuspending the sediment with the residual urine, is simple to perform and takes 5 minutes from sample urine adhering to the inside of the tube. The sensitivity, specificity, and likeliare influenced by how long the urine is allowed to sit after colhood ratios for these tests are summarized in Table 27. This Bayesian approach will reduce the because these bacteria do not convert urinary nitrates to number of incorrect diagnoses. Using the leukocyte esterase and nitrate in White cell casts can also be found in the urine sediment and combination (the dipstick is considered positive if either test is are identified by their tubelike granular appearance. False-positive reactions can occur from the peroxidase-like activity of myoglobin or the presence of bacteria that produce peroxidase. This tures are useful to confirm the infection and identify the approach is supported by research (22) and by a retrospective organism and its antibiotic susceptibilities when evaluating study of more than 4,000 women managed through telephone dysuria in children, men, and older women, and in younger contact, in which only 0. A concern about telephone-based tract infection or infection with bacteria not likely to respond treatment of dysuria is that this results in needless use of to first-line antibiotics. An algorithm for management appears in Figure of recommendations for different therapies. Women Recommended Therapies with risk factors for occult pyelonephritis (see Table 27. Singledose therapy has a high failure rate in these patients and Intervention Recommendation* should not be used (29). Recurrent infections typically occur in women with women) genetic or behavioral factors, discussed earlier, that place them No need for imaging (in B at an increased risk for infection. Increased fluid intake C A urine culture should be obtained for women with recurrent infections to both clearly document the infection and Behavioral interventions C identify the organism and its antibiotic susceptibility. Additionally, physicians often prescribe a short course of antibiotics to be kept on hand for use when a woman develops her typical symptoms. A urinary analgesic, with pyelonephritis should be placed into one of three groups: phenazopyridine, is useful for patients with significant dysuria 1. Women who are medically stable and maintaining hydrato quickly provide symptomatic relief. Three-day therapy results ing disability, are not medically stable or are unable to take in a cure rate similar to that achieved with 7 to 10 days of treatoral fluids or medications. Women who have infection complicated by abscess or tion is that 7 days of treatment are needed when nitrofuranobstruction, regardless of ability to take fluids by mouth. Generally, a follow-up visit is not Medically stable women who maintain hydration on oral required if the urinary symptoms resolve. More subgroup of women with symptoms typical of uncomplicated than 90% of healthy women who develop pyelonephritis fall lower tract infections. Amoxicillin-clavulanate vs ciprofloxacin for the treatment of uncomplicated cystitis in women: a randomized trial. Upper tract infection outpatient (oral antibiotics): female adult 14 days, male adult 14 days; geriatric patient 14 days or child 14 days. After a second lower tract infecfollow-up are all important for successful outpatient managetion or a single episode of pyelonephritis, the adult male ment of pyelonephritis. Fourteen days of antibiotics are generpatient should undergo imaging to identify an anatomic ally effective for outpatient treatment of otherwise healthy abnormality or nephrolithiasis. These symptoms are not specific and Women with pyelonephritis need hospitalization if they can be caused by many other conditions, including other infechave evidence of severe sepsis, are unable to take oral medications, hypoxia, an adverse reaction to medications, or metation, or have an infection complicated by obstruction or renal bolic abnormalities. For women with severe illness or urosepsis, the initial challenging because the symptoms are nonspecific and asympchoice of parenteral antibiotic should be a fluoroquinolone, tomatic bacteriuria is common, affecting 10% of elderly men piperacillin/tazobactam, or a third-generation cephalosporin. Intravenous antibiotics should be continued until traditionally recommended for older women (40). Urine culthe patient has been afebrile for 24 hours; the patient can then ture should be obtained before treatment because the organbe switched to an oral agent to complete the 14 days of therism or its antibiotic sensitivity is not as predictable as in apy. Pending culture results, these patients can be hours after switching to oral antibiotics (37). Older patients When patients do not improve after 72 hours of parwith upper tract infections should be treated using the same enteral therapy, imaging is indicated to identify a perguidelines given for men in the preceding section. If these are from abnormality, or ureteral obstruction; either sonography or documented relapses occurring after short course therapy, computed tomography can be used to identify these complisubsequent infections should be treated for 14 days with an cations.