
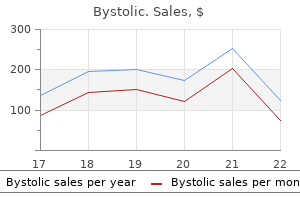
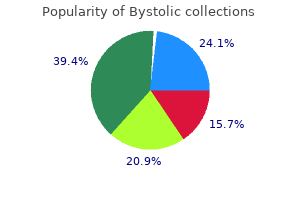
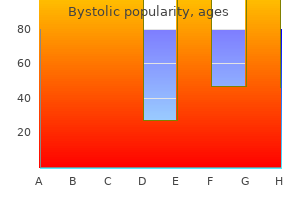
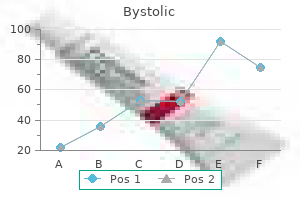
Bystolic
Discount bystolic
Even though the patient in the case pre sented has a family history of calcium oxalate calculi blood pressure what do the numbers mean buy bystolic overnight delivery, dehydration is the most likely cause of her stone formation. For this reason, calcium oxalate stones are more common in the summer months and in the 38. Other common types of stones include magnesium ammonium phosphate and carbonate apatite stones. These stones sometimes are called infection stones, since they form secondary to urinary tract infections with urea splitting bacteria. Urea splitting bacteria raise the pH of the urine, and this facilitates the formation of infection stones by lowering the solubility of magnesium-ammonium and phosphate. Infectious stones can enlarge quickly and sometimes can fill the entire renal collecting system to form a staghorn calculus. The term staghorn calculus indicates that the stone is a large stone, but it does not imply stone composition. All urinary calculi have the potential to form staghorn calculi; however, infection stones result in staghorn formation most often. Some stones, including uric acid and cystine stones, form sec ondary to metabolic abnormalities. These stones are seen less com monly in clinical practice, but they should be suspected in patients with a history of gout or homozygous cystinuria. Hyperuricosuria may be seen in gout, myelo proliferative disorders, idiopathic hyperuricosuria, and patients with increased dietary purine. Uric acid stones are clinically unique, since they cannot be seen on a standard abdominal x-ray. Since the formation of uric acid stones is very dependent on the pH of the urine, they generally form only if the urine pH is consistently below 5. Typically, an oral urinary alkalin izing agent, such as potassium citrate, is used to raise urine pH and dissolve uric acid stones. Cystine stones are uncommon and form only in patients who are homozygous for cystinuria. Cystinuria is an inher ited defect of the renal tubule causing loss of cystine, ornithine, arginine, and lysine. The loss of cystine is the only clinical problem patients suffer, since they excrete over 250mg of cystine per liter of urine. This high urinary cystine level is problematic, since stone for mation results in urinary cystine levels of 170mg per liter of urine at pH 5. Patients who are heterozygous for cystinuria excrete less urinary cystine and generally do not suffer from cystine stone formation. Risk Factors Some of the common risk factors for developing urinary calculi include inadequate fiuid intake, excess sodium intake, metabolic abnormalities, infiammatory bowel disease, dehydration, and family history. Patients with infiammatory bowel disease form stones composed of calcium oxalate by a unique mechanism. Fat malabsorption caused by the infiammatory bowel disease results in excess fats in the gut, which bind to calcium. This creates a situation in the gut in which oxalate, which normally binds to calcium, enters the bloodstream in its ionic 674 J. Since oxalte is a stone inducer, it binds with urinary calcium and facilitates calcium oxalate stone formation. Other medical conditions increase the risk for stone formation by causing hypercalciuria, which is excess calcium in the urine. These medical problems include renal tubular acidosis, sarcoidosis, hyper parathyroidism, chronic immobility, and paralysis. In these condi tions, hypercalciuria results when excess calcium is absorbed from bone or the gut and ultimately is excreted by the kidneys. In renal tubular acidosis, the renal tubule leaks calcium directly into the urine. Chronic urinary tract infection also can lead to stone formation due to urea splitting bacteria, which lead to an elevated urine pH. These end products cause a rise in urinary pH, which facilitates infec tious stone formation. These bacteria raise the pH of the urine, and this allows the precipitation of magnesium-ammonium-phosphate or apatite stones. Patients with infected urine and fiank pain due to an obstructing calculi may require hospitalization to prevent urosepsis. Management As illustrated in the case presented, most patients who present with fiank pain secondary to acutely obstructing urinary calculi can be managed on an outpatient basis. Cornerstones of therapy include adequate hydration, pain relief, and control of any associated nausea or vomiting. If the pain is severe enough to require intravenous morphine sulfate or if there is associated fever or dehydration due to nausea or vomit ing, hospital admission may be necessary. Again, one of the most important decisions the clinician has to make is to determine if the patient can be treated as an outpatient or if the patient needs hospital admission. There are several indications for hospital admission, and fever is a common indicator for admission (Table 38. Fever in the pres ence of obstructing urinary calculi can be an ominous clinical find ing that suggests an accumulation of purulent urine proximal to an obstructing stone. This is an especially serious situation if the patient has comorbid medical conditions, such as diabetes. Emergent intra venous antibiotics, aggressive intravenous fiuid hydration, and per cutaneous or transureteral drainage of the infected urine usually are necessary in these situations. Patients with fever and obstructing urinary calculi should not be discharged from the emergency room, as urosepsis and septic shock can develop quickly. Following the acute event, it is suggested that all patients who form urinary stones undergo a metabolic evaluation consisting of a com plete blood count, urinalysis, serum chemistry profile, and a 24-hour urine collection for calcium, phosphorus, uric acid, creatinine, citrate, and oxalate levels. Evidence-based practice management guideline for the evaluation of fever in critically ill adult patients. The nosocomial spread of pathogens must be avoided when using temperature measurement devices. Laboratory testing for the evaluation of fever should be individualized for each patient. Blood cultures Level I: For skin preparation, povidone-iodine should be allowed to dry for 2min, or tincture of iodine for 30s. Alcohol skin preparation, an acceptable alternative for iodine allergic patients, need not be allowed to dry. Additional cultures should be based on high clinical suspicion of bacteremia or fungemia, and not instituted automatically for each temperature elevation. If two peripheral sites are not available, one pair of cultures may be drawn through the most recently inserted catheter, but the diagnostic accuracy is reduced. Any expressed purulence from an insertion site should be collected for culture and Gram stain. The catheter should be removed and cultured for evidence of a tunnel infection, embolic phenomena, vascular compromise, or sepsis. Two blood cultures should be drawn peripherally, or one may be drawn from the most proximal port (if a multilumen catheter). Both the introducer and the catheter itself should be cultured for suspected pulmonary artery catheter infection. Posteroanterior and lateral films or computed tomography of the chest can offer more information. Respiratory secretions should be transported to the laboratory within 2h of collection. Pleural fiuid should be obtained for culture and Gram stain if there is an adjacent infiltrate or another reason to suspect infection. A second sample should be sent if the first is negative and suspicion remains high.
Order bystolic 5mg on-line
For the case of skin ease blood pressure 8860 buy bystolic 2.5 mg without prescription, ascites, pleural or pericardial effusion, infiammatory lesions, documentation by colour photography including a ru breast disease, lymphangitic involvement of skin or lung, ler to estimate the size of the lesion is suggested. As noted abdominal masses/abdominal organomegaly identified by above, when lesions can be evaluated by both clinical exam physical exam that is not measurable by reproducible imaging and imaging, imaging evaluation should be undertaken since techniques. However, lesions on chest X-ray may be considered quate imaging techniques to measure bone lesions. How measurable if they are clearly defined and surrounded by aer ever, these techniques can be used to confirm the ated lung. Study protocols should detail the conditions under which such lesions would be Endoscopy, laparoscopy: the utilisation of these techniques for considered measurable. Specifications by methods of measurements where recurrence following complete response or surgical resection is an endpoint. Measurement of lesions All measurements should be recorded in metric notation, Tumour markers: Tumour markers alone cannot be used to as using calipers if clinically assessed. Itm aybe tumour markers are disease specific, instructions for their the case that, on occasion, the largest lesion does not lend it measurement should be incorporated into protocols on a self to reproducible measurement in which circumstance the disease specific basis. When effusions are known to be a potential adverse reported as two dimensions in the plane in which the image effect of treatment. All other pathological nodes (those with short axis P10 mm but <15 mm) should be considered 4. Nodes that have a short axis <10 mm are considered non-pathological and should not be recorded 4. The baseline sum diameters Only patients with measurable disease at baseline should will be used as reference to further characterise any objective be included in protocols where objective tumour response tumour regression in the measurable dimension of the is the primary endpoint. Response criteria When more than one measurable lesion is present at baseline all lesions up to a maximum of five lesions total (and a max this section provides the definitions of the criteria used to imum of two lesions per organ) representative of all involved determine objective tumour response for target lesions. For evidence to support the selection of only five tar non-target) must have reduction in short axis to get lesions, see analyses on a large prospective database in <10 mm. If the lesions have truly coalesced such that they the smallest sum on study (this includes the baseline are no longer separable, the vector of the longest diameter sum if that is the smallest on study). All sured in the same anatomical plane as the baseline examina lymph nodes must be non-pathological in size tion), even if the nodes regress to below 10 mm on study. While on the concept of progression of non-target disease requires study, all lesions (nodal and non-nodal) recorded at baseline additional explanation as follows: should have their actual measurements recorded at each sub sequent evaluation, even when very small. To reiterate, however, if the radiologist is able to able) a useful test that can be applied when assessing patients provide an actual measure, that should be recorded, even if for unequivocal progression is to consider if the increase in it is below 5 mm. New lesions introduced before progression will affect best response desig the appearance of new malignant lesions denotes disease nation. There are no specific criteria for the and will also take into consideration the appearance of new identification of new radiographic lesions; however, the find lesions. Furthermore, depending on the nature of the study ing of a new lesion should be unequivocal: i. Table 1 on the next page provides A lesion identified on a follow-up study in an anatomical a summary of the overall response status calculation at each location that was not scanned at baseline is considered a new time point for patients who have measurable disease at lesionandwillindicatediseaseprogression. Smaller or greater time intervals than these could randomised trials, from date of randomisation) until the crite be justified in specific regimens or circumstances. In selected circum tients achieving stable disease for a minimum period of time stances certain non-target organs may be evaluated less fre is an endpoint of importance in a particular trial, the protocol quently. For example, bone scans may need to be repeated should specify the minimal time interval required between only when complete response is identified in target disease two measurements for determination of stable disease. However, these limitations of the precision of the specified sites of disease is warranted. Progression-free survival/proportion progression-free months after treatment) and should not be affected by delays in therapy, drug holidays or any other events that might lead 4. Reporting best response results tent (and usually consistently poor), that a non-randomised trial is justifiable (see for example van Glabbeke et al. Stable disease to this subset of patients is subject to criticism: it may result 4. If objective response is selected as a primary end proval decisions are to be based on the study outcome. An overview of these factors and other way that it is clear how these criteria should be applied for lessons learned from independent review is provided in an all trials in which anatomical assessment of tumour response article by Ford et al. Anatomic coverage: Optimal anatomic coverage for most solid tumours is the chest, abdomen and pelvis. This will involved based on signs and symptoms of individual greatly enhance the reproducibility of the tumour mea patients. Each case should be discussed with the radiologist to Most solid tumours may be scanned with a single determine if substitution of these other approaches is phase after administration of contrast. Therefore, the method of administration of and indeed this guideline presumes a minimum 5 mm intravenous contrast agents is variable. Rather than thickness in recommendations for measurable lesion try to institute rigid rules regarding methods for definition. With these metastases are demonstrated to best effect and a con parameters, a minimum 10 mm lesion is considered sistent method is used on subsequent examinations for measurable at baseline. Note that the number of lesions visible differs greatly between the two phases of contrast administration as does any potential lesion measurement. In general, it is preferred if patients on clinical trials the possibility of interval progression of disease. Other skin the base of the skull to the level of the mid-thigh should be ob or palpable lesions may be measured on physical examina tained 60 min post injection. Ideally, the same type of should always be measured at subsequent follow-up time scanner should be used and the image acquisition protocol points even if this results in measuring the lesion at a differ should be followed as closely as possible to prior scans. Body ent slice level or in a different orientation or vector compared scans should be performed with breath-hold scanning tech with the baseline study. Because malignant nodes are identified However, in some cases, the largest lesions may not be easily by the length of their short axis, this is the guide used to measured and are not suitable for follow-up because of their determine not only whether they are pathological but is also configuration. In these cases, identification of the largest most the dimension measured for adding into the sum of target le reproducible lesions is advised. There then reappears, its maximal diameter should be added to the are some tumours, for instance paraspinal lesions, which sum of the remaining lesions for a calculated response: in are better measured in the coronal or sagittal plane. However, this is potentially challenging to reproduce in a multicentre trial and if attempted should be done with careful imaging input and analysis. The most reproducible lesion is a lymph node (circled at baseline and at follow-up in the bottom two images).
Purchase 2.5mg bystolic visa
Pacara and Quebracho Rooms were reserved for the Poster Session area and were divided (see Poster Session layout) There were also other additional rooms reserved that were available for Committee Meetings and hospitality suites 5 fu arrhythmia order bystolic toronto. Registration Area the Registration Area was located at the Lobby Level in the access to the Convention Center. It was a convenient and strategic point for delegates to register before entering the congress and exhibit area. An industry-sponsored Post Graduate Course and a total of 14 industry-sponsored satellite symposium sessions took place during the congress. These slots are available as an integral part of the Platinum sponsorship package and will be allocated on a first come, first served basis. Approval of Scientific Committee with regard to program and invited faculty of a self-organized symposium is mandatory. The sponsoring company will have signs with their logo within the cyber cafe, their company home page as the default home page, and their logo as the screen saver on each workstation. Sponsors will have their logo displayed at the catering points for one day (two coffee breaks). For a better organization and administration, a sample of the promotional material will be required in advance. Cases will be sent to Moderators for a better coordination of the session, Speakers will have 10 minutes for the case presentation and 10 minutes for discussion. Case conclusions may include 1 or 2 slides with bibliographic reference on the topic. Discussion will take place after each video presentation Summary Session Presentation of a summary of the most relevant information on Pancreas, Liver, Biliary, Transplantation, presented at the congress Symposium Speakers will have 15 minutes for presentation. Discussion/Questions may take place after the last presentation or after each presentation. Update Lecture Speaker presentation: 20 minutes Questions/discussion: 10 minutes Video Debate Video Debaters will have 10 minutes (2 minutes for the introduction and 8 minutes for the video presentation) followed by a ten-minute discussion. They were asked to complete a form with their contact information and automatically an access code to their e-mail address was sent; this allowed the system to check if the e-mail address was operational. With the access code authors logged in to the system at any time before the deadline to submit a new abstract, amend submitted abstracts, withdraw an abstract or to see a list of all their submitted abstracts. Confirmation of receipt of abstracts:When authors had successfully submitted their abstract you would see a confirmation screen and an e-mail would be sent to them. Amendments to a submitted abstract: Within 10 days of submitting their abstract they were able to login again to the system to make amendments. Each Chair received an electronic file containing all the abstracts to be presented in his session. Presenters had a maximum of 10 minutes for presentation and 5 minutes for questions. Free Paper Session: Chairs for paper sessions were invited to participate 4 months before the Congress. Presenters had a maximum of 7 minutes for presentation and 3 minutes for questions. Each chair received an electronic file containing all the abstracts to be presented in his sesion. Presenters had a maximum of 3 minutes for presentation and 2 minutes for questions. Poster Session: Commentators for poster sessions were invited to participate 4 months before the Congress. Each Commentator received an electronic file containing all the Posters to be presented in his sesion. Poster Instructions: Presenters will be next to their poster during the poster viewing hours. Due to the strict times of the scientific program we request that you kindly respect the time alloted for the poster session. Video Session: Chairs for paper sessions were invited to participate 4 months before the Congress. Each chair received an electronic file containing all the videos to be presented in his sesion. In order to reduce room rental cost, we suggest not more than 2/3 meetings per day. Therefore abstracts accepted as Free Papers were re-scheduled as Mini Orals and Mini Orals were upgraded in order to replace those Free Papers. All this modifications were done considering the scores each paper had been given by the reviewers. On behalf of the Organizing Committee, it is our pleasure to invite you to participate in the following session/s: Speaker / Chairman / Co-Chairman Session: . However due to the society regulations, travel and accommodation expenses will not be covered. Upon your reply, the Organizing Committee will notify you of the date and time of your presentation. On behalf of the Organizing Committee, please find below the program of your participation: Monday, April 19 1:00 18:00 Session: Chairman. Note: Speakers will have 10 minutes for presentation (2 minutes for the introduction and 8 minutes for the video presentation). Discussion will take place after each presentation As mentioned in our previous communication, regarding registration fees, as Co-Chairman you will have 25% registration fee waived. In order to register for the congress we would appreciate using the following link for Speaker/Chairman/Co-Chairman: Discussion: minutes after each presentation or further information regarding the scientific program please visit. Upon confirmation of your participation, the Organizing Committee will send you further instructions regarding the on-line reviewing system. Once you have entered this information you will see the abstracts that you have been assigned for review. Clicking on the link beside the abstract title, the system will show the abstract text and below, the review form. In case you have any conflict of interest with the abstract, please check the checkbox I cannot evaluate this abstract due to a conflict of interest. Once you have finished the evaluation of the abstract, click the button send review. On behalf of the Organizing Committee we are pleased to inform you that your Paper. We would like to inform you that you paper entitled: has been accepted by the Scientific Committee for ini Oral presentation, in the following session: Session: .
Buy 2.5 mg bystolic with visa
The authors identified several limitations with the meta-analysis heart attack songs videos buy 5 mg bystolic free shipping, such as the heterogeneity of the pooled data, taking diagnostic rates at face value, and that only one study met the highest level of evidence criteria for clinical interventions. Patients were identified from pediatric sub specialty clinics as likely to have a genetic disease, and about half were purposely recruited from outside the Clinical Genetics clinic. Eligibility criteria included that their disease was well characterized clinically and was likely genetically heterogeneous, the standard of care at the time was to diagnose through targeted genetic testing, the targeted genetic testing included multiple genes, and the existing multigene test had incomplete sensitivity. Both parents had to be available for testing as well, if needed to resolve complex results. In the standard approach, the average number of conventional genetic tests needed for a diagnosis across the cohort was 3, covering an average of 19 genes. Eligible patients were <4 months old and had illnesses suggestive of a genetic disease, but were of unknown etiology. There were 129 infants in the study period that were potential candidates, and 65 (50%) were ultimately enrolled. Standard genetic testing was defined as any genetic test considered standard of care, and therefore available to order through the electronic medical record. In those that had standard genetic testing, a diagnosis was identified by the test in 23% (7) of test cases, and 24% (8) of controls. It was declined for two patients as they were not acutely ill and about to be discharged. Trio testing was performed on 29 cases, 1 quad (parents plus two affected children), 9 duos (mother-infant) and three infants only. In examining the standard genetic testing results, the authors note that 4 infants received a diagnosis from these results. The most common standard test was chromosome microarray, but routine chromosome analysis, fluorescent in situ hybridization, and various biochemical tests were also utilized. Thirteen children had a change in care as a result which included starting new medications (5), discontinuing medications (2), surgical procedures were changed (4). Pathogenic or likely pathogenic variants were found in 100 individuals (27%), with variants of uncertain significance in an additional 42 (11%). They sequenced 217 individuals from 156 independent cases or families across a broad spectrum of disorders in which previous screening had identified no pathogenic variants. The investigators quantified the number of candidate variants identified using different strategies for variant calling, filtering, annotation and prioritization. They found that jointly calling variants across samples, filtering against both local and external databases, deploying multiple annotation tools and using familial transmission above biological plausibility contributed to accuracy. Overall, the investigators identified disease causing variants in 21% of cases, with the proportion increasing to 34% (23/68) for Mendelian disorders and 57% (8/14) in family trios. They also discovered 32 potentially clinically actionable variants in 18 genes unrelated to the referral disorder, although only 4 were ultimately considered reportable. According to the investigators, their results demonstrate the value of genome sequencing for but also highlight many outstanding challenges, including the challenges of interpreting unrelated variants. The participants were families with an infant younger than 4 months with an acute illness of suspected genetic cause. Whole Exome and Whole Genome Sequencing Page 15 of 24 UnitedHealthcare Commercial Medical Policy Effective 09/01/2019 Proprietary Information of UnitedHealthcare. A change in clinical care or impression of the pathophysiology was reported in 49% of newly diagnosed families. Clinical data were collected principally through chart review, which may have led to under or overestimates of changes in clinical management. The authors did not ascertain information about long-term consequences of diagnosis, such as the impact of genetic counseling. Comparisons of costs of genomic and conventional diagnostic testing excluded associated costs of testing, such as outpatient visits, and may have included tests that would nevertheless have been performed, irrespective of diagnosis. Original raw data files were not available from this lab to determine if the variants were present but filtered out, or if the genes were not adequately covered. The diagnoses included in the cohort included retinitis pigmentosa (n = 311), retinal dystrophy (n = 101), cone-rod dystrophy (n = 53), Stargardt disease (n = 45), macular dystrophy (n = 37), and Usher syndrome (n = 37). In the remaining 5 individuals, the Whole Exome and Whole Genome Sequencing Page 16 of 24 UnitedHealthcare Commercial Medical Policy Effective 09/01/2019 Proprietary Information of UnitedHealthcare. The detection rate varied by phenotype, ranging from 84% in individuals with Usher syndrome to 29% in those with cone dystrophy. Only 30% of individuals with African ancestry had cases solved, compared to 55% of European ancestry or 57% of South Asian ancestry. Factors that may influence this study compare to others is the technology used, phenotype screening and phenotypes used. Five physicians proposed initial clinical follow-up based on the genetic findings. Depending on sequencing platform, 10% to 19% of inherited disease genes were not covered to accepted standards for single nucleotide variant discovery. Genotype concordance was high for previously described single nucleotide genetic variants (99%-100%) but low for small insertion/deletion variants (53%-59%). Curation of 90 to 127 genetic variants in each participant required a median of 54 minutes per genetic variant, resulted in moderate classification agreement between professionals, and reclassified 69% of genetic variants cataloged as disease causing in mutation databases to variants of uncertain or lesser significance. In the end, a total of 52 cancer patients had a usable trio of sample sets that included ten breast, 12 colorectal, seven endometrial, four prostate, 14 renal, and five thoracic cancers. There was relatively high agreement in regions that sequence reliably, but lower concordance in regions of complexity, and there were also differences found between different variant software used (Shimmer vs Stelka). Overall, 73 variants in 207 samples in 46 relevant genes were identified, and verified through conformational testing using a different technology. Turnaround time was a challenge, and at the beginning of the study, results took >80 days to complete. The authors reported that there were limited treatment options available based on results, including even when considering available clinical trials. Genome-scale sequencing may be appropriate as an initial genetic test under certain circumstances. The guidelines highlight that healthcare providers need to be prepared to provide detailed information on other lab tests performed, clinical evaluations and testing, and patient phenotype. Testing of additional family members may be required to interpret the test results of the patient. Finally, as new data emerges, the interpretation of a variant may change over time and the healthcare provider must be prepared to monitor and manage changing interpretations. Four new genes were added to the list of recommended secondary findings, Whole Exome and Whole Genome Sequencing Page 18 of 24 UnitedHealthcare Commercial Medical Policy Effective 09/01/2019 Proprietary Information of UnitedHealthcare. The new, updated secondary findings list includes 59 medically actionable genes recommended for return in clinical genomic sequencing (Kalia et al. It is recommended that a research setting where testing is offered on a case by case basis is the best current approach. Whole-genome sequencing offers additional but limited clinical utility compared with reanalysis of whole-exome sequencing. Microarrays and next-generation sequencing technology: the use of advanced genetic diagnostic tools in obstetrics and gynecology. Genetic test utilization and diagnostic yield in adult patients with neurological disorders. Whole Exome and Whole Genome Sequencing Page 19 of 24 UnitedHealthcare Commercial Medical Policy Effective 09/01/2019 Proprietary Information of UnitedHealthcare. Whole-genome sequencing is more powerful than whole-exome sequencing for detecting exome variants. Utility of whole-genome sequencing for detection of newborn screening disorders in a population cohort of 1,696 neonates.
Bystolic 2.5 mg amex
Reference Maione A et al: Proteinuria and clinical outcomes in hypertensive patients hypertension 1 discount 2.5 mg bystolic overnight delivery. See calcific uremic gene arteriolopathy cast nephropathy, 166 cutaneous losses, 8 central diabetes insipidus, 13 cyclosporine, 259 central pontine myelinolysis, 19 cystic diseases, of kidneys. See hemolytic uremic white coat, 237 syndrome hyperventilation, respiratory hyperaldosteronism alkalosis and, 91 primary, 33 hypervolemic hypernatremia, 16 secondary, 34 hypervolemic hyponatremia, 20 hypercalcemia, 50 treatment of, 19 familial hypocalciuric, 51 hypoaldosteronism, 36 of malignancy, 49 acquired hyporeninemic, 87 hyperglycemia hyperkalemia and, 32 hyponatremia and, 23 hypocalcemia, 54 osmotic diuresis and, 24 hypocitraturia, 219 282 Index hypokalemia, 37 IgM nephropathy, 133 distal renal tubular acidosis with, immunosuppressive medications 88 adverse reactions, 259 with high blood pressure, 39 mechanisms of action, 258 with high urinary potassium immunotactoid glomerulopathy, 165 excretion, 38 infections Liddle syndrome, 42, 227 posttransplant, 260 with low blood pressure, 40 microbial etiologies, 261 with low urinary potassium of urinary tract, 199, 203 excretion, 41 asymptomatic bacteriuria, 201 with normal blood pressure, 40 funguria, 202 with normal urinary potassium inherited diseases, of kidneys. See systemic lupus with hyperkalemia, 87 erythematosus with hypokalemia, 88 smoking-associated nodular with normal potassium, 88 glomerulosclerosis. See urinary tract infections 177 uveitis, tubulointerstitial nephritis cystinuria, 178 with, 191 Dent disease, 179 granulomatous interstitial V nephritis, 180 vaptans, 19, 20 lead nephropathy, 181 vascular diseases, of kidneys. See vesicoureteral refiux syndrome of inappropriate antidiuresis, 26 W Wegener granulomatosis. With few exceptions Medicaid benefciaries under age 65 must enroll in HealthChoice. Tese periods occur after initial eligibility determinations and temporarily lapses in Medicaid coverage. This section details Priority Partners outreach and support services, non-emergency transportation services, state support services and other information. This section briefy outlines some of the optional benefts that Priority Partners may provide. This section describes services requiring preauthorization, services not requiring preauthorization, preauthorization procedures, medical necessity criteria and other procedures and criteria. This section provides information on pharmacy beneft management, specialty pharmacy, prescriptions and the Priority Partners formulary, the Maryland Prescription Drug Monitoring Program, Corrective Managed Care Program and the Maryland Opioid Policy. This section covers the claims submission process, billing inquiries, the appeal process, quality initiatives and other claims and appeal information. Claims Submission, Provider Appeals, Priority Partners Quality Initiatives and Pay-for-Performance. Members must complete an updated eligibility application every year in order to maintain their coverage through the HealthChoice program. Medicaid-eligible individuals who are not eligible for HealthChoice will continue to receive services in the Medicaid fee-for-service system. Carve-out services (which are not subject to capitation and are not Priority Partners responsibility) are still available for HealthChoice members. We are responsible for reimbursing out-of-plan providers who have furnished these services to our members. The legislation improves the portability and continuity of health benefts, ensures greater accountability in the area of health care fraud and simplifes the administration of health insurance. When faxing information to Priority Partners, verify the receiving fax number is correct, notify the appropriate staf at Priority Partners and verify the fax was appropriately received. When leaving messages for Priority Partners associates, leave only the minimum amount of member information required to accomplish the intended purpose. The record usually contains your symptoms, examination and test results, diagnoses, and treatment. Tat information, referred to as your health or medical record, and legally regulated as health information may be used for a variety of purposes. The following are some examples of our possible uses and disclosures of health information. For example, your health care provider may send claims for payment of medical services provided to you. Examples of these oversight activities are audits, inspections, investigations, accreditations, and licensure. Inspect and copy: You have a right to see your health information upon your written request. If you want copies of your health information, you may be charged a fee for copying, depending on your circumstances. You have a right to choose what portions of your information you want copied and to have prior information on the cost of copying. If you request an amendment to records that we did not create, we will consider your request only if the creator of the records in unavailable. Accounting of disclosures: You have a right to request a list of the disclosures made up of your health information after April 14, 2003. Exceptions are health information that has been used for treatment, payment, and operations. Notice: You have the right to receive a paper copy of this notice and/or an electronic copy by email upon request. For More Information this document is available in other languages and alternate formats that meet the guidelines for the Americans with Disabilities Act. To Report a Problem about our Privacy Practices If you believe your privacy rights have been violated, you may fle a complaint. Providers further agree to inform benefciaries of their right to appeal a coverage determination pursuant to the applicable grievance procedures and according to law. Please note that information changes frequently and should not be used to determine member eligibility. Please contact your Provider Relations network manager at 410-762-5385 or 888-895-4998 or the Credentialing department at 410-424-4619 if you have questions about the credentialing process. The credentialing manager or designee will convene an appeal panel comprised of three qualifed practitioners. For the purpose of this requirement, a clinical peer is a provider with the same type of license. The panel shall not include any individual who is in direct economic competition with the afected provider or who is professionally associated with or related to the provider or who otherwise might directly beneft from the outcome. Knowledge of the matter shall not preclude any individual from serving as a member of the panel; however, involvement with any earlier decision concerning the initial determination or corrective action will require the individual to remove him/herself from the panel. Within 10 calendar days of either a frst or second-level panel review, and after reviewing any written statements submitted by the provider and any other relevant information, the panel will render a decision. This notice will be sent either by certifed mail return receipt requested or express mail with receipt of delivery. In accordance with the Maryland Annotated Code, Health General Article 15-1005, we must mail or transmit payment to our providers eligible for reimbursement for covered services within 30 days after receipt of a clean claim. If additional information is necessary, we shall reimburse providers for covered services within 30 days after receipt of all reasonable and necessary documentation. We shall pay interest on the amount of the clean claim that remains unpaid 30 days after the claim is fled. However, we are responsible for reimbursement to providers for professional services rendered during the remaining days of the admission if the member remains Medicaid eligible.
Fliggers (Orris). Bystolic.
- Purifying blood, skin diseases, bronchitis, cancer, improving appetite and digestion, inflammation of the spleen, liver and kidney problems, vomiting, constipation, bad breath, teething pain, and other conditions.
- How does Orris work?
- What is Orris?
- Dosing considerations for Orris.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96636
Generic bystolic 5 mg otc
If you are not sure of their purity arrhythmia game purchase generic bystolic pills, test one by eating it and searching for it in your immune system five minutes later. In spite of craving a pickles/chocolate pudding/carbonated beverage lifestyle, you must eat mainly good food. Her hormone test showed slightly high (125 pg/ml) estrogen levels for day 22 (if it really was day 22! Obvi ously, something was irritating the ovaries into overproduction of estrogen. She was switched to milk (3 glasses 2% a day) as her primary beverage besides water. She was toxic with nickel (dental metal) which would invite hordes of urinary tract bacteria, dangerously close to the ovaries. She broke out in hives from a new hair spray polluted with praseodymium which got into her ovaries. They wormed the dog monthly and did not want to part with it since they did not believe it mattered. She had seven laparoscopies for endometriosis and very hard cramps with her period. Her ovaries and uterus were toxic with mercury and thallium from polluted dental alloy. Christopher Gravely, a young man of 26 and Frederica, 22, promised faithfully not to get pregnant until their cleanup was complete. Eight months later he had completed all his tasks, his low back and pain with urination had stopped, and this encouraged him to continue with his fertility program. She, too, was started on the kidney herbs and instructed to get metal tooth fillings replaced. She was to drink three glasses of 2% milk a day and take a magnesium tablet and stop drinking other beverages. Three weeks later her husband canceled her appointment because she was too embarrassed and delighted to call herself. To digest it, they first break the urea molecule apart into two ammonia molecules. Nickel is plentiful in the soil which is undoubtedly where these bacteria belong, breaking up and utilizing the urine and droppings left there by animals. They perform an essential task in our environment, destroying animal excrement and thereby cleaning-up the soil around us. If we did not supply them with nickel, as if we were just another patch of earth, they could not gain a foothold in our urinary tract and then to the prostate. You will later wash the knife but not before you have eaten enough nickel to supply all the bacteria in your body with the daily allowance of their essential element, nickel. The skin oils dissolve nickel from metal jewelry (sometimes leaving your skin with a greenish black color) and transport it into your body. Notice that you get a fresh attack after accidentally using metal cutlery in a restaurant or eating mayonnaise-style salad with a metal spoon stuck in it. Read about the benefits of flaxseed, too, but remember to test every product for pollutants before accepting it as a supplement. Prostate problems of all kinds clear up when bacteria are zapped, the Kidney Cleanse is done, dental cleanup is done, and the Bowel Program is followed. Richard Traylor, age 71, had suffered from prostate and urinary tract disease for three years. He was started on the kidney herbs and in two weeks (13 days) he had a considerable im provement in urine flow. He got rid of his water softener (such salts are polluted with chromate), toothpaste (strontium source) and opened the crawl space vents (source of radon). He was so pleased he decided to install a crawl space fan and pursue a parasite program and dental health just to see what extra health improvements he might get. He could now barely walk, due to weakness and pains of several kinds; his prostate problems began several years ago. He was started on only half a dose of the herbal recipe to give them a chance to dissolve more slowly. At this time we found Ascaris (both kinds) which he killed with a frequency generator. After killing them immedi ately with a frequency generator and getting instant relief of pain, he got his own device and did not need to return. A half year later he had no remaining pains and was able to father his first child. If the lobe on your right side with the pain persists, especially if it gallbladder tucked inside. Toxic items are changed chemically into non toxic items that the kidney is able to excrete into the bladder. If the bile ducts are choked with debris so only half as much (often only a cup instead of a quart! Taking cholesterol-lowering drugs should be reserved for cases where natural excretion cannot be regained. If your side pain is accompanied by bloating and gas, you know you have a digestive problem. To clear the clogged passages of the bile ducts, you simply do the liver cleanse (page 552) over and over until the problem is gone. If there are living parasites in the bile ducts, they will not let the bile ducts clear themselves. The thymus is an immunity-giving gland, so anything in the thymus is a very serious matter. Three weeks later the benzene was gone, his side was very much better and he could begin a kidney cleanse for his low back pain. Midabdomen Pain, Stomach Pain the colon crosses over from your right side to the left side at the midabdomen. But if the bile is full of live parasite stages and bacteria they may try to colo nize the stomach, too. Your nose and mouth mucous traps a lot of these whereupon you swallow them and they glide into the stomach. Your dentalware may be cleaned up in a few dental visits but the liver cleanses must go on for a year or two before it is reasonably clean. You may get pain relief in a few weeks but this should not derail your intention to revitalize yourself completely with a cleaned liver and stomach. Hiatal Hernia When bacteria have spread to the diaphragm and weak ened it, along with the upper stomach valve, food is al lowed to get pushed up right through the diaphragm. It is quite possible the baby had these also, giving him a nasty tummy ache in addition to the gas pains. The only progress we have made to date with this disease is to give drugs to soothe the symptoms. Some never leave the stomach, causing children stomach aches and, of course, a large entourage of bacteria which, in turn, have their viruses. Asthma sufferers become allergic to many air pollutants such as pollen, animal dander, smoke. The production of histamine in the lungs and the vast interconnectedness of histamine to allergies has been well studied scientifically. Use cardboard, newspaper or anything that you can afford to throw away with the mess. It is also an al lergic reaction, to the pet and to other inhaled bits of matter. Smoke of any kind, fragrance and chemicals of any kind, all household cleaners, polishes, and so forth should be removed. Install central air conditioning if possible, with maxi mum filtering (but never with chemicals added to the filter and never with a fiberglass filter) at the furnace. When you suddenly need them, try to identify your source of reinfection or allergens.
Purchase bystolic 2.5 mg on-line
Ureteral stenting or nephrostomy diversion should be considered after delayed reconstruction due to the increased risk of postoperative urinary extravasation prehypertension statistics best buy bystolic. The overall rate of patients who undergo a nephrectomy during exploration is around 13%, usually in patients with penetrating injuries and higher rates of transfusion requirements, haemodynamic instability, and higher injury severity scores [98]. Other intra abdominal injuries also slightly increase the need for nephrectomy [99]. Mortality is associated with overall severity of the injury and not often a consequence of the renal injury itself [100]. In gunshot injuries caused by a high-velocity bullet, reconstruction can be difficult and nephrectomy is often required [101]. Watertight closure of the collecting system, if open, is desirable, although closing the parenchyma over the injured collecting system also has good results. If the capsule is not preserved, an omental pedicle flap or peri renal fat bolster may be used for coverage [102]. Following blunt trauma, repair of vascular injuries (grade 5) is seldom, if ever, effective [104]. Repair should be attempted in patients with a solitary kidney or bilateral injuries [105], but is not used in the presence of a functioning contralateral kidney [26]. Nephrectomy for main artery injury has outcomes similar to those of vascular repair and does not worsen post-treatment renal function in the short-term. Isolated grade 1-3 stab and low-velocity gunshot wounds in stable patients, after complete staging, B should be managed expectantly. Radiological embolisation is indicated in patients with active bleeding from renal injury, but without B other indications for immediate abdominal operation. Intraoperatively, renal reconstruction should be attempted once haemorrhage is controlled and there is B sufficient viable renal parenchyma. Repeat imaging 2-4 days after trauma minimises the risk of missed complications, especially in grade 3-5 blunt injuries [106]. Repeat imaging can be safely omitted for patients with grade 1-4 injuries as long as they remain clinically well [107]. Nuclear scans are useful for documenting and tracking functional recovery following renal reconstruction [108]. Follow-up should involve physical examination, urinalysis, individualised radiological investigation, serial blood pressure measurement and serum determination of renal function [68]. A decline in renal function correlates directly with injury grade; this is independent of the mechanism of injury and the method of management [109, 110]. Follow-up examinations should continue until healing is documented and laboratory findings have stabilised, although checking for latent renovascular hypertension may need to continue for years [111]. In general, the literature is inadequate on the subject of the long-term consequences of renal tissue trauma. Delayed complications include bleeding, hydronephrosis, calculus formation, chronic pyelonephritis, hypertension, arteriovenous fistula, hydronephrosis and pseudo-aneurysms. Delayed retroperitoneal bleeding may be life-threatening and selective angiographic embolisation is the preferred treatment [112]. Perinephric abscess formation is best managed by percutaneous drainage, although open drainage may sometimes be required. Percutaneous management of complications may pose less risk of renal loss than re-operation, when infected tissues make reconstruction difficult [86]. Renal trauma is a rare cause of hypertension, and is mostly observed in young men. The frequency of posttraumatic hypertension is estimated to be less than 5% [113, 114]. Hypertension may occur acutely as a result of external compression from peri-renal haematoma (Page kidney), or chronically due to compressive scar formation. Treatment is required if the hypertension persists and could include medical management, excision of the ischaemic parenchymal segment, vascular reconstruction, or total nephrectomy [115]. Urinary extravasation after reconstruction often subsides without intervention as long as ureteral obstruction and infection are not present. Persistent urinary extravasation from an otherwise viable kidney after blunt trauma often responds to stent placement and/or percutaneous drainage as necessary [117]. Arteriovenous fistulae usually present with delayed onset of significant haematuria, most often after penetrating trauma. Post-procedural complications include infection, sepsis, urinary fistula, and renal infarction [119]. In numerous case reports, transcatheter embolisation appears to be a reliable minimally invasive solution [120]. Acute renal colic from a retained missile has been reported, and can be managed endoscopically if possible [121]. C First follow-up should be approximately 3 months after major renal injury with hospitalisation. Each C follow-up should include: physical examination, urinalysis, individualised radiological investigation, serial blood pressure measurement and renal function tests. Medical management and minimally invasive techniques should be the first choice for the C management of complications. The incidence of associated injury in penetrating renal trauma ranges from 77% to 100%. Gunshot wounds are associated with adjacent organ injury more often than stab wounds. Most patients with penetrating renal trauma have associated adjacent organ injuries that may complicate treatment. In the absence of an expanding haematoma with haemodynamic instability, associated multiorgan injuries do not increase the risk of nephrectomy [29]. Blunt and penetrating injuries contribute equally to combined renal and pancreatic injury. Renal preservation is achieved in most patients, and the complication rate is 15% [122]. A similar rate of complications (16%) is reported in patients with simultaneous colon and renal injury [123]. In cases where surgical intervention is chosen, all associated abdominal injuries should be managed C where appropriate simultaneously. When deciding on conservative management all injuries should be considered independently. Predisposing factors include hypertension, renal medullary disease, central biopsies, and numerous needle passes [128]. Arteriovenous fistulae and pseudo-aneurysms can occur in 1-18% of allograft biopsies [125]. Extrarenal pseudo-aneurysms after transplantation procedures generally occur at the anastomosis, in association with local or haematogenous infection. Arterial dissection related to transplantation is rare and presents in the early postoperative period [129]. Iatrogenic renal trauma associated with endopyelotomy is classified as major (vascular injury), and minor (urinoma) [130]. Patients undergoing cryoablation for small masses via the percutaneous or the laparoscopic approach may have asymptomatic perinephric haematoma and self-limited urine leakage. Renal foreign bodies, with retained sponges or wires during open or endourological procedures, are uncommon. A pseudo-aneurysm should be suspected if the patient presents with flank pain and decreasing haematocrit, even in the absence of haematuria. A close watch on irrigation fluid input and output is required to ensure early recognition of fluid extravasation. Intra-operative evaluation of serum electrolytes, acid-base status, oxygenation, and monitoring of airway pressure are good indicators of this complication. In arterial dissection related to transplantation, symptoms include anuria and a prolonged dependence on dialysis. Common symptoms of pseudo-aneurysms are flank pain and visible haematuria within 2 or 3 weeks after surgery [133]. Pseudo-aneurysms appear on ultrasound as anechoic cysts, with intracystic flow on colour Doppler. Potential complications of retained sponges include abscess formation, fistula formation to the skin or intestinal tract, and sepsis.
Cheap generic bystolic uk
Urinary excretion of total coproporphyrin is normal blood pressure 160100 purchase bystolic in united states online, whereas the proportion of isomer 1 is higher than in normal controls (>80%). Total coproprophyrin excretion is greater than normal, as in other hepatobiliary disorders, and isomer 1 makes a smaller proportion (<80%) than in Dubin-Johnson patients. Background Drugs are the second most common cause of acute liver failure, and are the predominant cause of liver injury in the Western world. Rarely do these patients have a background history of liver disease (Andrade et al. If a medication is having a toxic effect on the liver, it should be stopped quickly in the hope that the liver damage will not progress. However, despite that, many cases follow a sub-acute course with progression to liver failure. Excluding the cases of acetaminophen (45%) overdose, 15% of cases were idiosyncratic reactions to drugs. Marked elevations in transaminases reflect an hepatocellular pattern in 87% of patients, while 13% had a cholestatic pattern. Hepatocellular variety has been documented to carry worse prognosis, compared to cholestatic. There are numerous mechanisms of liver injury, but it is not always possible to determine which mechanism of injury is responsible for the hepatotoxicity (Table 5). Finally, drugs or drug metabolites may act as haptens and bind covalently to + hepatic proteins. Clinical Presentation There are a variety of presentations for the persons with drug associated hepatotoxicity, ranging from the finding of abnormal liver enzyme tests in the asymptomatic persons, to life First Principles of Gastroenterology and Hepatology A. Clinical features of acute liver failure fi Whole body o Systemic inflammatory response o High energy expenditure and catabolism fi Liver o Loss of metabolic function o Decreased gluconeogenesis leading to hypoglycemia o Decreased lactate clearance leading to lactic acidosis o Decrease ammonia clearance leading to hyperammonemia o Decreased synthetic capacity leading to coagulopathy fi Lungs o Acute lung injury o Adult respiratory distress syndrome fi Adrenal gland o Inadequate glucocorticoid production contributing to hypotension fi Bone marrow o Frequent suppression, especially in viral and seronegative disease fi Circulating leukocytes o Impaired function and immunoparesis contributing to high risk of sepsis fi Brain o Hepatic encephalopathy o Cerebral edema o Intracranial hypertension fi Heart o High output state o Frequent subclinical myocardial injury fi Pancreatitis o Particularly in paracetamol-related acute liver failure fi Kidney o Frequent dysfunction or failure fi Portal hypertension First Principles of Gastroenterology and Hepatology A. Shaffer 488 o Might be prominent in subacute disease and confused with chronic liver disease Permission to reprint: Bernal et al. Acetaminophen Acetaminophen is an effective over-the-counter analgesic, and is safe when taken in a daily dose that does not exceed 4 gm. For example the malnourished, alcoholic taking an acute dose of acetaminophen of >100mg/kg or a 10 to 20 gm dose over three days will develop: acute zone 3 necrosis, extending to bridging or panacinar (massive) necrosis. Liver failure may result from attempted suicide or therapeutic misadventure, as confirmed by a recent literature review (Larson et al. Fatal cases usually involve 20 gm acetaminophen (caution in the heavy alcohol abuser, where even 2 gm may be fatal). Over 20% develop severe liver injury, and of these, 20% die from the hepatotoxicity. This in turn leads to the production of reactive oxygen species, hepatocellular apoptosis, and centrilobular necrosis. Hyperacute injury to the liver occurs within 48 to 72 hours after acetaminophen ingestion. Death can occur in 4 to 8 days from cerebral edema, sepsis, liver and multi-organ failure. After 4 hours of taking an overdose, when most of the acetaminophen has been emptied from the stomach and absorbed, blood levels reflect the prognosis. The risk is assessed with the Prescott nomogram, which plots the plasma concentration of acetaminophen versus hours post ingestion. Note that with chronic intake, blood levels of acetaminophen are not a reliable indicator of liver injury as it is with acute overdose. From an understanding of the metabolism of acetaminophen we can appreciate the reason for the lag interval, variable dose dependency, effects of alcohol, drugs, fasting, and malnutrition, and the potential therapeutic benefit of a cysteine donor. With acute doses of acetaminophen (> 10 g/day), and during the first 48 hours after overdose the primary pathway is overwhelmed and the secondary pathway becomes involved (Figure 2). Antiretroviral Agents Hepatic damage is not uncommon with nucleosides and nucleotide reverse transcriptase inhibitors, as well as protease inhibitors. Therefore, it is important to consider all these factors, as they contribute to liver damage. This leads to fatty liver (micro and/or macrovascular steatosis), First Principles of Gastroenterology and Hepatology A. The onset of these abnormalities will usually be about 6 months into the treatment. Acute hepatitis occurs in 3% to 30% of persons taking the protease inhibitor ritonavir. Acute liver failure is rare; the unconjugated hyperbilirubinemia seen in 7% of persons given protease inhibitors does not forebode progression to severe cholestasis. With Diclofenac, for example, 5 hepatotoxicity occurs in about 5 persons per 10 exposed, but clinical hepatitis is uncommon, and fatalities are exceedingly rare. Anti Tuberculosis Therapy For every 100,000 persons given Isoniazid, about 2000 will develop hepatitis, and approximately 150 will die from acute liver failure. After acetaminophen, isoniazid-hepatitis is the second most common reason for the liver transplantation for drug-induced liver injury. It is important to stress that the hepatotoxicity of isoniazid does not relate to the dose or blood level. Immunosuppression agents Azathioprine or methotrexate may frequently be used in persons with chronic hepatitis or inflammatory bowel disease (Crohn disease or ulcerative colitis). Regardless, all patients are recommended to be on folinic acid to reduce side effect profile. A liver biopsy can be considered if cumulative dose of 1000-1500mg has been achieved. Oral Contraceptives There is a widespread use of oral contraceptive agents in young women, and several cholestatic hepatic toxicities are recognized (Table 12) Table 12. Hepatobiliary complications of the use of oral contraceptive agents o Gallstone o Cholestasis o Unmasking cholestatic disease such as primary biliary cirrhosis 4. Drugs causing Chronic Hepatitis Some drugs such as nitrofurantoin, methyldopa and minocycline may cause chronic hepatitis, especially in older women who have been on the drug for a long interval. In another form of chronic drug-associated hepatotoxicity, anti-nuclear and anti-smooth muscle antibodies develop. In the same token, there are drugs which are relatively contraindicated in persons with liver disease (Table 14). It is unreasonable to commit these long list to memory, but this information would be useful for you to have handy on your iPhone. A regenerating nodule will partially block the blood flow in the hepatic sinusoidal and hepatic vein (Figure 8). In time however 50 mg these collaterals may burst and lead to life threatening bleeding such as from esophageal varices. A more physiological consideration is whether the cause is presinusoidal (prehepatic and many intrahepatic conditions), postsinusoidal (posthepatic plus two intrahepatic conditions; alcoholic terminal (central) hyaline sclerosis in zone 3, and veno occlusive disease), or sinusoidal (alcoholic hepatitis or established cirrhosis). The resistance may rise in the liver because of mechanical pressure on the vessels from inflammation, swelling of the hepatocytes, collagen deposited in the space of the Disse, fibrosis and architectural change) or because of the activation of the hepatic stellate cells (aka myofibroblasts, fat storing or Ito cells)leading to vasoconstriction of the sinusoids and elevated microvascular pressure. The portal disease may be measured directly by the percutaneous insertion of a needle into the portal vein, liver or spleen. Normal anatomy Before considering what happens to the patient with cirrhosis, we need to review briefly the normal gross anatomy of the liver (Figure 1), including the portal venous system (Figure 2). Extrahepatic Short gastric vein Left gastric vein Splenic vein Inferior mesenteric vein-tributaries Umbilical vein from the left colon and rectum Superior mesenteric vein-tributaries from B. Progressive branching of the intrahepatic portal vein and its distribution to the lobes of Obliterated umbilical the liver. There are numerous causes of portal hypertension (Figure 5), the most common of which is the increased portal pressure which occurs as a result of cirrhosis. As a result of the portal hypertension, a collateral circulation develops between the portal and the systemic circulation (Figure 8).