
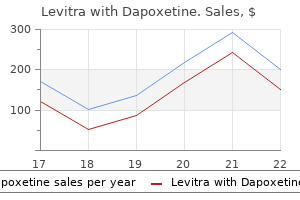
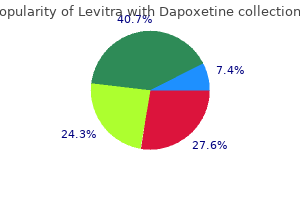
Levitra with Dapoxetine
Order levitra with dapoxetine 40/60 mg line
Efcacy of Helicobacter and emptying: randomized controlled study evaluation pylori eradication therapy on functional dyspepsia: a by real-time ultrasonography natural erectile dysfunction treatment remedies cheap levitra with dapoxetine 20/60 mg fast delivery. Symptom improvement after Efcacy of buspirone, a fundus-relaxing drug, in patients helicobacter pylori eradication in patients with funcwith functional dyspepsia. Clin Gastroenterol Hepatol tional dyspepsia: a multicenter, randomized, prospective 2012;10:1239-1245. Herbal medicines for the treatrandomized, double-blind, placebo-controlled trial. The efect of short-term, low-dose tricyclic and tetraIberogast on proximal gastric volume, antropyloroduocyclic antidepressant treatment on satiation, postnutrient denal motility and gastric emptying in healthy men. Am J load gastrointestinal symptoms and gastric emptying: a Gastroenterol 2007;102:1276-1283. A prospective randomized tensifed medical and psychological interventions in pastudy. Research has shown that if properly developed, communicated and implemented, guidelines can improve care. The advice on dyspepsia and heartburn given in this guideline is based on epidemiological and other research evidence, supplemented where necessary by the consensus opinion of the expert development team based on their own experience. If you wish to replicate or reproduce this guideline, in part or in full, please obtain agreement from the New Zealand Guidelines Group. The New Zealand Guidelines Group asks people wanting to reproduce guidelines to contact them and have stated that access will not be unreasonably withheld. Where guidelines are modified for local circumstances, significant departures from the national guidelines should be fully documented and the reasons for the differences explicitly detailed. Furthermore, the dyspepsia and heartburn symptoms themselves, and the inconvenience resulting from them (including loss of work), carry important personal, social and financial costs. The treatment of dyspeptic symptoms in our current practice is often random, poorly advised and not evidence-based. The cost to the country (and not infrequently to people with dyspepsia and heartburn) needs to be rationalised so that those who are in most need achieve rapid and effective management. The aim of this guideline is to promote up-to-date recommendations for the safe and efficient management of these individuals. The guideline is evidence-based and represents a distillation of a review of the extensive literature in the field. The guideline is aimed particularly at primary health care providers, but also at medical and surgical specialists who are involved in the care of people with dyspepsia and heartburn. This guideline is designed to guide management decisions, not to dictate a blanket policy. The company invited two general practitioners and three gastroenterologists to investigate this issue. Throughout the process the Working Party has expressed and maintained the need for the guideline process to be completely independent. Since 1995, when the National Health Committee produced guidelines for dyspepsia, the evidence has changed considerably. At that time, treatment1 advice was that refiux and ulcer-like dyspepsia may respond better to acid inhibition while other types may respond better to motility agents. Prokinetics were2 seen as more effective for dyspepsia than acid inhibitors, and a review of the evidence concerning the precise indication for their use has been published. Providing specific advice for New Zealand conditions will help counter consumer pressure to follow inappropriate advice. The four regional working groups each established a systematic search of the literature. When the core committee convened they made a decision that the evidence tables would not be published nor would they include the level of evidence for each study in the guideline text. Rather, the committee would put its emphasis on producing a workbook style guideline with detailed references for those who wish to delve into the original research. Their drafts were developed between 1998 and 2001 by which time they had been submitted to the Core Committee for review. Decisions were made by consensus of the various groups, and eventually with the Core Committee. These were then collated and edited by members of the Core Committee and a professional editor/writer. The edited copies were returned to the four working groups to ensure they had maintained their original interpretation. Opportunity was given to update the information with the final drafts being returned in mid 2002. The final draft was again reviewed by the Core Committee and further corrections were made. Most of the suggestions and comments made by reviewers were addressed before submitting the final version. They were discussed with representatives of the Best Practice Advocacy Centre Inc who reviewed the draft fiow diagrams in association with some of their representatives and general practitioners. Other dyspepsia guidelines published between 1998 and June 2003 were perused to ensure appropriate information was considered in developing the New Zealand version of the Guideline. As updates of Cochrane Reviews became available, they were also included in the review process to ensure new developments had been considered. Short-term treatment with proton pump inhibitors, H receptor antagonists and prokinetics for gastro-oesophageal refiux2 disease-like symptoms and endoscopy negative refiux disease. An evidence-based approach to the management of uninvestigated dyspepsia in the era of Helicobacter pylori. American Gastroenterological Association Consensus Development Panel (Chaired by W. Successful implementation of guidelines also requires adequate availability of information for all involved and adequate provision of health care resources. It is not envisaged that the guideline should greatly increase the demand for this procedure. Ensure the early identification of complications especially where those might require surgery. Stimulate early investigation and diagnosis of serious pathology, including cancer. Appreciate the role of surgery where this is demonstrated to present a cost-effective option. Promote reduction in surgical intervention where cost-effective medical alternatives exist. Improve public knowledge, especially as to what constitutes normality and what may be required in diagnosis and treatment. Reduce the incidence of new peptic ulcer disease by appropriate education and public health measures. Thanks go to Mary Trewby and Stewart Wells for editing the guideline, and Reywa Brown, Pers Howe and Annie Bourvis who provided secretarial assistance. A period of three years is suggested; this will need to be negotiated with the New Zealand Guidelines Group and those nominated for the committee (see Chapter 8: Evaluation). In the next update, information on nutrition and diet, as well as alternative and complimentary remedies (eg, slippery elm) may be added if appropriate information is published on these topics. The New Zealand Guidelines Group took over administration of funds from the Royal Australasian College of Physicians. Only a minority of people with dyspepsia have specific abnormalities (eg, erosive oesophagitis, peptic ulcer or cancer). The challenge of this guideline is to present an approach that helps the doctor to choose which people to treat empirically and whom to investigate (when and how), and to guide management of specific diagnoses. The first encounter between the person with dyspepsia and the practitioner starts with the undifferentiated symptoms of dyspepsia or heartburn. Alarm signals are clearly defined to channel the individual for early investigation. Others require more information, exercising both the art and science of medical practice, and guidance is given here to the management of this group.
Syndromes
- Hives and itching
- Fortified foods such as soymilk
- Antibody titer
- Cocaine or other illegal drugs
- Have other family members had this problem?
- Foreign body aspiration
- Medicines to treat symptoms
- Sling surgery
Buy cheap levitra with dapoxetine on line
Amniotic membrane may be used instead of conjunctiva although recurrence is more likely 2 impotence recovering alcoholic purchase 40/60mg levitra with dapoxetine with mastercard. Local beta irradiation has been used but has a significant risk of late scleral necrosis b. Frequency may range from over 50% for bare sclera techniques to 5-20% with conjunctival flaps and grafts B. Dellen associated with swollen or excessively thick conjunctival or amniotic membrane graft at limbus F. Antibiotics can be discontinued once epithelial integrity has been re-established B. Topical corticosteroids are often continued for a few months to reduce the risk of recurrence C. Observation for recurrence is carried out over progressively extended periods of time E. A comparative study of recurrent pterygium surgery: limbal conjunctival autograft transplantation versus mitomycin C with conjunctival flap. A randomized trial comparing mitomycin C and conjunctival autograft after excision of primary pterygium. Vascularization is more delayed in amniotic membrane graft than conjunctival autograft after pterygium excision. Randomised controlled study of conjunctival autograft versus amniotic membrane graft in pterygium excision. Efficacy of subconjunctival 5-fluorouracil and triamcinolone injection in impending recurrent pterygium. Conjunctival autografting combined with low-dose mitomycin C for prevention of primary pterygium recurrence. Protect the cornea from mechanical damage secondary to abnormalities of the eyelid. Noninfectious corneal ulcerations or small perforations especially those requiring cyanoacrylate glue d. Cosmetic tinted and painted lenses (such as in patients with aniridia, iris defects, or corneal opacity) k. Anatomical considerations leading to an inability to place or center a contact lens 2. Larger lens more stable but increases the area of tissue that depends on exchange of metabolic nutrients through the lens D. The higher the Dk the more oxygen permeability; yet the stiffer the contact lens F. The patient seen at slit-lamp biomicroscope within the first 24-48 hours after placement B. Proper lens lubrication with preservative-free artificial tear drops and ointments E. Two or three mm disc punched from plastic surgical drape may be used along with glue as corneal patch for larger perforations H. Remove glue when healed or allow it to fall off as epithelialization occurs under glue E. Call if pain increases, contact lens falls out or a gush of fluid is noted Additional Resources 1. Cyanoacrylate glue for corneal perforations: a description of a surgical technique and a review of the literature. Symptoms of recurrent corneal erosions (sudden onset of eye pain, usually at night or upon first awakening, with redness, photophobia, and tearing) a. History of previous traumatic corneal abrasion, usually secondary to a sudden sharp, shearing injury (fingernail, paper cut, tree branch) a. May have pooling of fluorescein over affected area or negative staining if heaped epithelium 2. Chronic phase: nonpreserved lubricants, hypertonic saline (5% NaCl) ointments; topical corticosteroids combined with systemic tetracyclines B. Procedure is typically performed with patient sitting at slit lamp biomicroscope D. A bent (usually 25 gauge) needle tip (to reduce the risk of full-thickness penetration of the cornea) is used to make numerous superficial puncture wounds into the superficial corneal stroma in the involved area and extending slightly beyond the borders of the previously observed erosions, allowing a firm adhesion to develop as the epithelium heals E. Significant scarring, with increased risk from more aggressive/deeper punctures, may reduce best corrected visual acuity 1. If scarring begins to appear, topical corticosteroids may help to decrease severity B. If microbial keratitis develops, cultures and scrapings should be performed and broad-spectrum topical antibiotic therapy should be initiated pending culture results C. Explanation as to likelihood of the procedure to be effective and the possible need for retreatment Additional Resources 1. Anterior Stromal Puncture for the Treatment of Recurrent Corneal Erosion Syndrome: Patient Clinical Features and Outcomes. Microbial keratitis (to decrease pathogen load in fungal and acanthamoeba keratitis and to enhance corneal penetration of the topical medications) 4. Ocular surface disease (debridement of necrotic epithelium in chemical corneal burns, corneal intraepithelial neoplasia) 5. Irregular or heaped-up traumatic corneal abrasion (See Traumatic corneal abrasion) 6. Corneal topography or keratometry (to detect irregular astigmatism in some cases) D. Pressure patch, bandage contact lens, lubrication, topical antibiotic for recurrent erosion or traumatic corneal abrasion C. Superficial keratectomy with or without the use of diamond burr for recurrent erosions E. Remove the loosely adherent epithelium using a cotton swab, surgical sponge, spatula, blade, or forceps while avoiding trauma to Bowman layer E. Instill antibiotic, nonsteroidal anti-inflammatory drug, and cycloplegic eyedrops. Follow sterile technique and maintain the patient on topical antibiotic until epithelium heals 2. Screen patients for dry eyes and other predisposing conditions such as neurotrophic keratopathy 2. Avoid traumatizing Bowman layer when using a surgical blade to perform debridement 2. Describe expectations for postoperative pain and slow, gradual improvement of comfort and visual acuity Additional Resources 1. Sight-threatening or progressive corneal infiltrate exhibiting one or more of the following: i. Infectious crystalline keratopathy if cultures not easily obtained with superficial scraping 2. Corneal infiltrate in a region of the cornea that is very thin, making risk of perforation during biopsy excessively high b. Confocal microscopic examination, if strongly suggestive of the presence or absence of infectious organisms, may obviate the need for a corneal biopsy B. Anterior chamber paracentesis and aspiration of infiltrate on posterior surface of the cornea D. If patient is very cooperative, all techniques except trap door may be performed with patient seated at the slit-lamp biomicroscope 3. If needed, a cotton tip applicator soaked in lidocaine may be held at limbal position where forceps fixation performed C. Supersharp blade may be used to create a vertical or oblique incision to allow sampling using sterile needle or spatula 2. Braided silk suture can be passed through the infiltrate; then cut into pieces for inoculation 3. A flap (either triangular or rectangular) of anterior stroma is created overlying the active edge of the deep stromal infiltrate with a supersharp or #69 blade, reflected, and the underlying tissue is excised using forceps and a surgical blade b. A 2 or 3 mm corneal or dermatologic trephine is used to perform a partial-thickness trephination overlying the active edge of the deep stromal infiltrate b. Corneal scrapings plated onto culture media as well as glass slides for staining 2. Corneal tissue specimens divided and sent in fixative to histopathology laboratory and in sterile saline to microbiology laboratory 3. Discuss case with pathology laboratory prior to submitting specimen to alert them as to small specimen size and to ensure use of proper container V.
Cheap 20/60mg levitra with dapoxetine mastercard
The normal fow of the anterior capsule is rubbed upon by the iris; the axial aqueous is blocked at the level of the ciliary body erectile dysfunction ugly wife cheap levitra with dapoxetine 40/60mg online, lens region is usually free. These fakes tend to collect in the or anterior vitreous face, causing misdirection posteriorly angle of the anterior chamber and may obstruct the drainof aqueous humour into the vitreous. Small, hyperopic eyes with angle-closure tion of the lens capsule have a high chance of developing glaucoma are more prone to develop malignant glaucoma glaucoma (Fig. It can also occur after cataract surgery, capsulotPigmentary Glaucoma omy or even spontaneously. Pigmentary glaucoma is a secondary open-angle glaucoma Patients complain of severe pain with blurring of vision. Increased pigmentation in the traclinician must rule out a choroidal detachment, pupillary becular meshwork seen as Sampaolesi line on gonioscopy block or suprachoroidal haemorrhage to reach a diagnosis is also characteristic. Cycloplegic agents, especially topical atropine, dethe long-term prognosis is good, and feld loss occurs in crease the tone of the sphincter muscle of the ciliary body, only a few eyes. This causes a thinning and posterior displacement of the lens, deepening the anterior chamber. Elevated Episcleral Venous Pressure Phenylephrine also tightens the zonules by contraction of Secondary glaucoma is readily caused by elevated episcleral the longitudinal muscle of the ciliary body. Medical therapy is effective in some cases, but needs to be continued for months or years. If such conservative measures do not work, a An intraocular tumour may cause secondary glaucoma, not pars plana vitrectomy, with or without lensectomy, reduces by its increase in volume but by infltration of the angle by the volume of the vitreous and re-establishes the fow of neoplastic tissue or aqueous seeding. Prognosis for the control of intraocular pressure is currently better, but the condition tends to recur, and the other eye is at great risk of developing a similar problem. We are now aware that glaucomatous damage ordinarily takes a long time to develop. Symptomatic damage in a patient detected at the age of 45 years might be the result of elevated intraocular pressure for 20 years. Juvenile open-angle glaucoma, often hereditary, is probably second in frequency to pigmentary glaucoma. White, flaky material is much less common and is often associated with specifc deposited all over the anterior chamber, seen here at the pupil. Up to this age, the eye wall is and sclera stretch so that the globe gradually enlarges; distensible, so that the eye can noticeably and progressively this stretching and expansibility may mask the increased enlarge when the intraocular pressure is elevated (Fig. Most cases of primary congenital glaucoma occur spoCommon associations with congenital glaucoma are radically. In approximately 10% in whom a hereditary patneurofbromatosis (see Chapter 32, Ocular Manifestations tern is evident, it is believed to be autosomal recessive. It may occur without other ocular fndings, primary conClinical Features genital glaucoma, or in association with other syndromes, Symptoms: Congenital glaucoma is usually detected by or may occur after injury, congenital cataract extraction, or parents when: infammation, secondary congenital glaucoma. As the cornea stretches, breaks occur in the corneal endothelium, which normally Primary congenital glaucoma occurs due to the failure of pumps water out of the cornea to maintain its transpardevelopment or abnormal development of the trabecular ency. The iris may not completely separate from the the cornea, causing it to swell, and assumes a hazy, cornea so that the angle remains closed by persistent frosted-glass appearance. Depending on the degree of l An infant may become irritable to the point of burying obstruction, the result is a permanent rise in intraocular its head in a pillow to avoid light. Neonatal congenital glaucoma In early cases, there may be: occurs with more extensive congenital malformations and l Ground glass appearance of the cornea has a poor prognosis. This is then repeated on the Juvenile Primary Open-angle Glaucoma other side so that eventually the upper half of the canal wall is opened. Localization of the canal itself, however, is Glaucoma occurring between the ages of 4 and 10 years sometimes diffcult. Surgical treatment is often successful, although more than one operation may be necessary. Maximal tolerated medical therapy is one that may concentration of myocilin may increase resulting in a rise be used to control intraocular pressure, yet allows the patient in intraocular pressure. If, however, this does not control the intraocular pressure adequately, laser trabeculoplasty as described earlier, or surgery may be required. The importance of treatment and regular follow-up must be explained and emphasized. Surgery is commonly undertaken when medical therapy Management requires continued supervision by an ophfails to arrest visual feld loss, as in a non-compliant patient, thalmologist and consists of simple recordings of readings in a patient who cannot report for repeated review, or if the of applanation tonometry and status of the optic nerve head. Once the ganglion cells have been damaged and the vision carried by those Glaucoma-Filtering Operations nerve fbres lost, they cannot be replaced. Loss of vision Glaucoma-fltering operations are employed to control the in glaucoma is irreversible. This bleb is composed of spongy tissue, through controlled, and closely monitored. The initial treatment of glaucoma is generally instead of the normal drainage into the trabecular meshmedical or by laser procedures. In a corneoscleral incision the lips of the wound are defned for each patient with a chronic glaucoma, taking in good apposition and healing rapidly takes place. This is into account the intraocular pressure at which damage ocmuch less likely to occur if there is a gap between the lips curred, the family history, the extent of damage to the optic of the wound which becomes flled with loose scar tissue nerve head, visual feld, and the presence of systemic risk resulting in a fltering cicatrix. Very high intraocular pressures need to be lowered immediately with the use of intravenous acetazolamide or mannitol. Trabeculectomy Oral acetazolamide or glycerol take about half to one hour Trabeculectomy involves the creation of a lamellar scleral to control moderately high intraocular pressures. Lowering fap, under which, a piece of sclera which includes a short the intraocular pressure to near physiological levels allows length of the canal of Schlemm is excised, thus producing topical medication to become effective. Such an operation these systemic medications is not advisable, due to possibly also forms a fltering channel to the subconjunctival space life-threatening side-effects. If the wound heals and excessive scar tissue seals these are used as frst-line treatment for a raised intraocular the fap over the drainage hole, the pressure in the eye pressure. Reformation of the of these medications is often applied during the primary anterior chamber with balanced salt solution, air or viscotrabeculectomy. The most glaucomas, and the fltering bleb that results is a difpresence of a draining bleb covered with thin conjunctiva fuse elevation of the conjunctiva showing microcystoid may lead to the subsequent development of blebitis, or changes at the limbus (Fig. This is most common if antifbroblastic agents have been used to enhance fltration and Complications ensure the success of a trabeculectomy. Cataract is a In the early postoperative period shallowing of the anterior common sequel, particularly if early changes are present chamber and hyphaema may be seen. The glaucoma progression analysis or In refractory glaucomas where a trabeculectomy has failed, the peridata programme analyse signifcant differences in or is likely to fail, valved or non-valved drainage devices threshold values at each location in the feld (Fig.
Buy levitra with dapoxetine 20/60mg amex
Atelocollagen is a collagen solution that is extracted the puncta can be achieved with thermal cautery erectile dysfunction symptoms buy 20/60mg levitra with dapoxetine with amex. Recanalization can occur, depending on the collagen dissolves in a neutral phosphate buffer solution. If this technique used and the infiammatory response that occurs, and in solution is injected through the punctum, it turns into a whitesuch cases a repeat procedure is necessary to completely close the colored gel at body temperature. It appears that techniques involving superficial plug has proven successful in a variety of studies [270e272]. Succauterization have a higher rate of recanalization [305], and that cinylated collagen plugs [273], and hypromellose 2% [274], may be deeper surgical procedures may increase the success rate [296]. The plug is To date, there are no large scale, Level 1 studies to support the supplied on a pre-loaded inserter that dispenses the plug from contention that punctal occlusion of any form is effective in the within a polyamide sheath. However, 14 supportive Level 2 studies are In addition to devices, certain types of cyanoacrylate adhesives listed in Table 4 [252,257,263,270,272,274,283,308e313]. Moisture chamber spectacles and humidifiers clusion, there are a variety of surgical options that can be used, as Moisture chamber spectacles are eyeglasses specially designed described in section 2. Author Subject group N Treatment Reported benefits Comments duration (months) Balaram et al. While the clinical efficacy of moisture signal-regulated kinase stimulated cell proliferation and migrachamber spectacles has been reported in case reports [314,315],to tion via P2Y2 receptor mediated intracellular calcium elevation date, no high level studies have investigated the therapeutic value [328]. Lacritin is a glycoprotein that has prosecretory activity in the Locally placed humidifying devices have also been proposed to lacrimal gland and mitogenic activity at the corneal epithelium and enhance humidity or local air quality. However, only one controlled is reduced in the tears of patients with Sjogrensyndrome [330], and study lends support to their effectiveness in the management of dry other forms of dry eye [128]. Topical secretagogues production of mucin-like glycoproteins in human corneal epithelial 2. It is a purinergic P2Y2 receptor agonist that stimulates water patients received 2% rebamipide four times per day for 52 weeks and mucin secretion from conjunctival epithelial cells and goblet [333]. Lissamine green conjunctival staining, corneal fiuorescein cells, leading to improved tear film stability in dry eye [14,318,319]. Therapeutic failure of commonly used in the treatment of autoimmune diseases and one secretagogue did not predict similar results with the other, transplant rejection. It has potent effects on inducing Neuromodulation is a therapeutic strategy that involves intersecretion of mucins in conjunctival cells, in both in vitro and in vivo facing directly with the nervous system through electrical, elecstudies, suggesting that it might have potential as a future treattromagnetic, chemical, or optogenetic methodologies [363,364]. The goal is the long-term activation, inhibition, modification, and/ Trefoil factors are secretory products of mucin-secreting cells. It or regulation of neural input to correct organ or tissue dysfunction has been found that the levels of Trefoil factor family peptide 3 and manage disease symptoms. In an in vitro lates tear production following chemical or mechanical stimulation study, some proinfiammatory cytokines, but not hyperosmolarity, of the nasal mucosa [365,366]. This device consists of a hand-held stimulator unit equipped found to upregulate genes involved in lipid metabolic pathways, with a disposable two-pronged hydrogel tip and an external and downregulate those related to keratinization, in human meicharger. The intranasal tear neurostimulator allows self-delivery of bomian gland epithelial cells in a number of laboratory-based minute electrical currents to the anterior ethmoidal nerve, thereby studies [348e351]. Oral secretagogues period, mean conjunctival staining and symptom scores were Two orally administered cholinergic agonists, pilocarpine and significantly reduced from baseline. A number of People with Sjogren syndrome treated with oral pilocarpine for other studies are ongoing and results are awaiting publication 12 weeks experienced a beneficial effect on symptoms and reduc[371,372]. These include abdominal breathing for 3 min, production was shown by Schirmer testing [355,356]. The most commonly reported Corneal cold thermoreceptors are activated by drying of the L. Lid hygiene through prescribing topical antibiotic drops or ointment (such as Appropriate lid hygiene is important in the management of a fusidic acid) alone is not commonly recommended over the longer variety of lid conditions that result in dry eye (particularly bleterm, but is adopted by some practitioners [402] and a short dose of pharitis) and, if used appropriately, can reduce lipid by-products a topical antibiotic has been recommended in consensus-based and lipolytic bacteria associated with these conditions [379e385]. Demodex infestation is a causative gesting that baby shampoo may have an adverse effect on goblet factor in many cases of intractable blepharitis and is often associcell function [388]. Historically, the treatment of ocular Demodex included foams, solutions, and wipes; their individual description is outside a wide variety of products, most of which had no high level evithe scope of this review. However, compliance with following been found with the use of topical products containing tea-tree oil lid hygiene instruction is notoriously poor. Paperbark or Tea tree, which is native to Australia) that exhibits Despite the fact that various professional organisations suggest antimicrobial, anti-infiammatory, antifungal, and antiviral Table 5 Level 2 studies of lid hygiene in dry eye disease. Author Subject group N Lid hygiene variations Treatment duration Reported benefits (months) Paugh et al. Author Subject group N Treatment variations Treatment Reported benefits duration (months) Kheirkhah et al. To ocular Demodex than a daily lid scrub with a 50% concentration of enhance the potential performance of lipid-based drops, nanobaby shampoo [417]. The temperature and time sitic drug primarily used to treat strongyloidiasis and control required for melting obstructive material within the meibomian onchocerciasis. It is a low cost, single dose medication that is very gland excretory duct has not been definitively established. One oral dose of ivermectin has been liminary evidence from multiple studies has reported a range of shown to successfully reduce the number of Demodex found melting points (32 45 C) for the contents of the meibomian adjacent to the lashes of patients with blepharitis [411,412]. Perglands, refiecting in part that meibum is a highly complex lipid formance has been improved by combining the use of ivermectin mixture [434,435,437e439]. Meibomian gland material causing with metronidazole [415], or with permethrin cream [421]. More severe obstruction has a higher melting point than material from studies are needed to confirm the role of ivermectin for treating less obstructed glands [434,437,440]. A number of studies have found an repeated eyelid warming with a non-moist device improved tear improvement in signs and symptoms with the use of lipid-based film function in normal individuals and may have beneficial effects L. Author Evidence Patient group N Treatment Reported benefits Comments Level duration Korb et al. Optimal contact between the compress and eyelid should be achieved and the compresses 3. Several preliminary studies on non-dry eye plugged into an electrical outlet to provide latent heat, without participants have investigated the effect of different warm compressure, on the eyelids. All of the compresses sealed watertight chamber to provide a warm, high humidity showed an increase in temperature at the lower lid conjunctival environment over each eye. A preliminary study on normal subjects surface and none caused any damage to the eyelids. However, only found that the device increased the temperature of the eyelids the continuous layered application of warm bundled towels heated [433], and a study on dry eye patients reported that tear film in a microwave was able to maintain a temperature of 40 C on the evaporation was reduced 32% immediately after treatment [452]. This study concluded that a Two randomized, controlled, investigator-masked studies found wet surface improved heat transmission through the lid and should greater efficacy with Blephasteam than with warm towel treatbe used versus dry treatments [433]. Care should be taken not to ment [429,453] and a randomized, investigator-masked, crossover heat the eyelid skin to more than 45 C to avoid thermal damage study conducted on healthy volunteers found Blephasteam [445,446]. Visual acuity also significantly eyelid skin as a patient will not tolerate a cloth that is excessively improved after use of Blephasteam [453]. Ifeye area were also observed in individuals unresponsive to warm rubbing occurs when the corneal temperature is elevated, corneal compress treatment [430]. The risks of ocular massage with elevated corneal temperature have been deemed to 3. The first prospective, open-label, occasional retreatment sessions leading to greater comfort. A randomized, controlled, examiner-masked study month, while the warm compress group showed improvement found the EyeGiene mask was similar in efficacy to a warm towel, only in symptoms. After receiving the crossover treatment, the but not as effective as Blephasteam [429] or as effective in raising warm compress group also demonstrated significant improvement ocular temperature as a fiaxseed-based eye mask [457]. The infrared warm masked clinical trial, compared a single LipiFlow treatment to a compression device consists of an eye mask with two rigid patches robust 3 month regime of twice-daily warm compresses combined over the eyes. Eachpatchhas 19 light emittingdiodes, emittingnear with both lid massage and lid hygiene [72]. These subjects were infrared radiation from 850 to 1050 nm, with a peak at 940 nm. Total subjective symptom scores improved and there was more recent prospective, multicentre, open-label 12 month clinical alsosignificantimprovementintearevaporationratesduringforced trial randomized 200 subjects (400 eyes) and reported that the blinking, fiuorescein and rosebengal staining and meibomiangland single LipiFlow treatment effect, with improved gland function orifice obstruction score [458]. Physical treatments cant and sustained improvement in meibomian gland function and the purpose of applying physical treatment to the meibomian symptoms for up to 3 years after a single treatment [468]. Physical expression for therabeen used in dermatology to deliver intense pulses of non-coherent peutic amelioration of obstructive material should not be confused light from 500 nm to 1200 nm in wavelength to treat various with diagnostic expression, where minimal forces are used to conditions, including skin pigmentation, sun damage and acne determine if the gland is functional [441].
Order on line levitra with dapoxetine
For a post-treatment review erectile dysfunction and pump purchase levitra with dapoxetine 20/60 mg without prescription, an examination of the patient by another dentist may be necessary. The Committee also assesses, in the cases presented for its review, whether there are grounds to believe that a provider has fraudulently submitted claims or claimed for services that were not dentally required. When electronic submission is not possible, a form is available for paper claim submission, claim forms for insured services are provided to all participating dentists. If other identification is accepted and the claim cannot be processed due to identification errors, it will be the responsibility of the dentist to locate the patient/parent/guardian for correct information. In practice, it is easier and faster for the dentist to complete and submit the form either electronically or manually on behalf of his/her patient. It should be indicated on the form submitted that payment is directed to the patient. The dental authorization may be submitted prior to rendering necessary services or coincident with the commencement of treatment. These details include the fee code, the quadrant, tooth numbers, the surface codes, a brief description of the services when required, the rendered dental fee and the estimated lab fee, if applicable, to the treatment. Children with private dental plans are required to access their private coverage first. Additional services and financial discussions must be made with the resident, parent or guardian prior to service delivery. Granted approvals will be on file for a period of 2 years at which time, if dental necessity remains, a new application must be submitted with supporting documentation of continued care. All children who meet the age criteria are eligible for one annual examination, two routine radiographs and one caries prevention service per year. A limited number of other diagnostic and preventive services are insured according to the tariff of fees. Eligibility is determined by the performing dentist according to the coverage guidelines listed below and pre-authorization is not required when the guidelines are determined by the performing dentist to be met. Supporting documents as evidence of eligibility, including chart entries and diagnostics, must be provided in the event of a post audit. Procedures performed for local or generalized pain and/or discomfort which are unsupported by radiographic evidence are not insured services. Some surgical procedures are not only bilateral but involve all four quadrants performed at the same appointment, with separate incisions in each. When two quadrants are involved in surgical procedures, the first procedure will be paid at 100% and the subsequent procedure at 50%. When more than two quadrants are involved, the first two are paid at 100% and subsequent procedures at 50%. Written explanation must be submitted for further assessment of eligibility in these cases. Examinations and diagnosis, complete oral 01101 Examination and diagnosis, complete, primary dentition, to include 36. Examinations and diagnosis, limited oral 01202 Examination and diagnosis, limited oral, previous patient (recall): 23. Radiographs, panoramic 02601 Single film (once per lifetime, only in connection with a specific 54. Radiographs, cephalometric 02701 Single film (once per lifetime, only in connection with a specific 54. Tests, microbiological 04101 Microbiological test for the determination of pathological agents + L 32. Tests, histological Test, histological, soft tissue 04311 Biopsy, soft oral tissue, by puncture + L 75. Nutritional dietary counselling (maximum payable per lifetime is 1 series of 4 appointments) 13101 1 unit of time 26. Sealants, pit and fissure (acid etch preparation included; coverage guidelines apply see preamble in the Dentists Guide) 13401 Each tooth 21. Disking of teeth, interproximal (maximum 3 units per lifetime, primary teeth only) 16201 1 unit of time 56. Space maintainers, stainless steel crown type 15201 Space maintainer, stainless steel crown type, fixed + 168. Space maintainers, maintenance of (this service is not insured if provided to address necessary repairs and adjustments after 30 days following the original placement. Restorations, amalgam, primary teeth Restorations, amalgam, non-bonded, primary teeth 21111 1 surface 46. Pins, retentive per restoration (for amalgams and tooth coloured restorations) 21401 1 surface 16. Restorations, prefabricated, metal, permanent dentition 22301 Permanent anterior 128. Restorations, prefabricated, plastic, permanent dentition 22501 Permanent anterior 134. Restorations, tooth coloured, permanent anteriors, acid etch/bond technique 23111 1 surface 77. Restorations, tooth coloured, permanent bicuspids, acid etch/bond technique 23311 1 surface 83. Restorations, tooth coloured, permanent molars, acid etch/bond technique 23321 1 surface 87. Restorations, tooth coloured, primary, anterior, acid etch/bond technique 23411 1 surface 71. Restorations, tooth coloured, primary, posterior, acid etch/bond technique (see prosthodontics section for inlays, onlays and pins) 23511 1 surface 59. Gold, butt margins (including collarless veneers), custom shading or any aesthetics included in the lab fees are not insured. Crowns, plastic (single units only) Crowns, plastic, processed 27111 Crown, plastic, processed + L 415. Crowns, porcelain/ceramic/polymer glass 27201 Crown, porcelain/ceramic jacket + L 510. Crowns, porcelain/ceramic fused to metal 27211 Crown, porcelain/ceramic fused to metal base + L 510. Recementation/rebonding, inlays/onlays/crowns/veneers/ posts/natural tooth fragments (maximum of 3 units per tooth) For stainless steel crowns, recementation is payable after 120 days following original placement by same or different dentist 29101 1 unit of time 61. Root canals, permanent teeth, retained primary teeth (includes clinical procedures with appropriate radiographs, excluding final restoration) 33111 1 canal 342. Opening through artificial crown (in addition to procedures) 39211 Anteriors and bicuspids 85. Bleaching, non-vital (maximum of 3 units insured per resident) Bleaching endodontically treated tooth/teeth 39311 1 unit of time 56. Periodontal splinting or ligation, provisional, extra-coronal Acid etch joint restorations (per joint) 43211 Per joint 47. Removals, erupted teeth, complicated 71201 Odontectomy, (extraction), erupted tooth, surgical approach, 146. Removals, impactions, soft tissue coverage Removals, impaction, requiring incision of overlying soft tissue and removal of the tooth 72111 Single tooth, 146. Removals, impactions, involving tissue and/or bone coverage (including removal of bone and tooth or sectioning and removal of tooth) 72211 Single tooth, 177. Services delivered in an office setting are subject to the terms and conditions associated with payer of last resort regulations whereby private insurance benefits must be accessed first.
Pegwood (Wahoo). Levitra with Dapoxetine.
- Constipation, indigestion, water retention, and other conditions.
- How does Wahoo work?
- Are there safety concerns?
- Dosing considerations for Wahoo.
- Are there any interactions with medications?
- What is Wahoo?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96367
Purchase 40/60 mg levitra with dapoxetine
Many of us only discover its importance when our mouth becomes dry while presenting at an important speaking engagement erectile dysfunction what doctor proven 20/60 mg levitra with dapoxetine. Apart from moistening our tongues and lips while speaking, saliva has several major functions, which include the lubrication of the bolus for ease of swallowing, the maintenance of oral hygiene, and the regulation of acidity in the oesophagus. Where a person has no oral motor deficits there may still be problems with saliva production, which can result in changes in saliva viscosity. This may affect swallowing, and result in increased dental caries and periodontitis. Poor saliva control can occur in people with developmental, acquired or progressive disabilities. Hypersalivation is rare and not usually a cause of drooling (Tahmassebi and Curzon, 2003). Where a person has oral motor difficulties the problems with saliva may result in saliva overfiow (also called drooling or dribbling) and cause embarrassment and social isolation. Drooling is usually considered normal until a child is over 2 years of age (Morris and Dunn Klein, 2000). However some children with no obvious neurodevelopmental disabilities may drool until six or seven years (Johnson et al. Tahmassabi and Curzon (2003) suggested that, in children with cerebral palsy and an intellectual disability, drooling becomes less apparent after the development of permanent dentition. There are no separate prevalence rates available for those with an intellectual disability or other neurological conditions. People with acquired neurological conditions frequently encounter saliva control problems. Drooling in these conditions is related to impairment of oral control rather than an increase in saliva production. Secretion control problems are seen in adults where dysphagia occurs after multiple strokes involving both cerebral hemispheres or following a brain stem stroke. The problem is usually worse in the acute phase but may continue to be an issue depending on the site and extent of infarction (Smithhard, 1997). People with developmental disabilities, in particular cerebral palsy, often retain immature swallowing patterns. This tongue thrust pattern becomes more apparent as the person matures because the space in the oral cavity increases, resulting in protrusion of the tongue during the oral phase of swallowing and drooling. Drooling is most prominent when the anti-Parkinsonian medication is not effective. The tongue is particularly affected in motor neurone disease (Robbins, 1987) and consequently saliva cannot be collected and propelled into the pharynx. Because pharyngeal impairment frequently co-occurs with oral impairment, aspiration of saliva may be a problem. Understanding the mechanism of saliva fiow and production is essential if one is to understand the management of the range of difficulties with saliva. Diagrammatic representation of afferent and efferent pathways that are involved in refiex salivary secretion under the coordinating control of the salivary centres. Secretions from the sublingual glands fiow through the ducts of Rivius, situated on the fioor of the mouth (see Figure 6. The structure of the salivary glands is typical of all exocrine glands, being composed of small structures called acini, into which the epithelial cells secrete saliva, and ducts that transport the saliva. The parotid glands only produce serous secretions whereas the submandibular and sublingual glands produce both serous and mucoid secretions. Parasympathetic input increases the amount of saliva associated with eating and drinking. Sympathetic input reduces the quantity of secretion when not eating or drinking and during physical activity (see Figure 6. The average person produces and swallows approximately 600 ml of saliva a day (Watanabe and Dawes, 1988). This movement of the saliva is important to protect the teeth from developing caries. Frequent swallowing avoids the pooling of saliva in the mouth, the dribbling of saliva when we incline our head, or the spraying of saliva when we talk. It is not known whether the trigger for a saliva swallow is at the same point as for a nutritional swallow but it is possible these are different (see Chapter 3). A mature swallow is characterized by the oral phase (a voluntary phase) and a pharyngeal phase (an involuntary phase). The oral phase is considered to be more infiuenced by cortical function whereas the pharyngeal phase is thought to be mediated within the brain stem (Bass, 1997). As with speech, the movements of the oral phase of swallowing can be defined as a learned motor sequence (Daniels, 2000). The swallowing sequence is executed so frequently that it becomes automatic; however, because it is under volitional control it is readily modifiable. The obvious difference between swallowing saliva and swallowing food and drink is a comparative lack of anticipation when swallowing saliva. Once in the mouth the size, taste, temperature and texture of the bolus further stimulate the swallow sequence. These inputs lack the strong sensory input of food and fiuid but effective swallowing of saliva relies on an intact sensory system that is able to detect relatively small amounts of secretions within the mouth and pharynx (see Chapter 1 for further information). The ultasound technique was pioneered by Barbara Sonies and although it has been used elsewhere by other researchers (Kenny et al. Limited use of ultrasound to study swallowing may be due to the level of skill needed to interpret the images. It is a safe non-invasive technique that can be applied to a child or adult in any position. This can be done repeatedly and audio and video recordings can be made, allowing detailed analysis. It has potential for measuring and visualizing the swallowing of saliva among individuals with various disabilities. Cervical auscultation has shown promise for measuring swallowing frequency in different populations (Cichero, 1996; Allaire and Brown, 2004). This has been described as two or three clicks depending on whether it is a dry or wet swallow (Cichero, 1996). The best location for placing the stethoscope has been extensively studied (Takahashi et al. Takahashi recommended that the sensor be centrally placed just below the cricoid cartilage. This procedure is non-invasive; however, the assessor needs to be trained in listening to the sounds in order to interpret the swallow sounds. The value of this method is that it can be used on any participant who can tolerate a stethoscope on the neck for a short time, does not involve radiation exposure and is highly portable. Intact pharyngeal sensation is necessary for the initiation and execution of the swallow refiex. Secretions in the pharynx must be cleared regularly to ensure that they are not aspirated. Problems with secretion management are often related to dysphagia and pharyngeal impairment has potentially more serious health consequences than drooling. Consequently, information gained through videofiuoroscopic assessment of swallowing function is useful when planning management strategies for secretion problems. Videofiuoroscopy provides information regarding jaw closure, the ability of the tongue to propel material from the oral cavity into the pharynx. Further, it enables the effectiveness of the pharyngeal structures in clearing the material to be assessed, including determination of pharyngeal pooling of secretions (Logemann, 1998).
Purchase levitra with dapoxetine 40/60 mg mastercard
For those who deliberately choose not to use tests erectile dysfunction drug has least side effects discount levitra with dapoxetine 40/60mg mastercard, lack of utilization does not indicate lack of access but rather expression of a choice. While this is true in general for all genetic testing, the fact that many in the Deaf Community contest the understanding of deafness as a disability is particularly relevant to this particular case study. Hereafter our analysis will proceed on assumption that we are addressing the use of genetic testing among those who want it and can benefit from it, while recognizing that some would not seek testing even if it were freely available at no cost, and access were not an issue. D-1 (ii) Facilitating early interventions such as hearing aids, cochlear implants, or sign language that significantly improve language ability; (iii) Understanding disease progression; (iv) Monitoring associated clinical manifestations and complications, particularly for syndromic hearing loss; and (v) Providing accurate information on the chance of recurrence that some may choose to use in making decisions about having children (and others may not). This problem was characterized most 4 famously in May 1998 by Heller and Eisenberg. The related notion of a patent thicket is that there is so much intellectual property that needs to be accumulated that it becomes difficult to cut through it all. Blocking can happen from just one or a few patents on key sequences, key methods, or other inventions, if they are difficult or impossible to invent around. This is a concern for hearing loss genes because patents on one or a few common variants might enable those who hold the relevant patents to prevent others from testing for other hearing loss genes. One concept in intellectual property that requires aggregation of many patent rights is the incentive for hold-out. The fact that different mutations have different frequencies (and therefore explain different fractions of cases) means that the potential commercial value of a mutation patent varies. Patents covering common variants should, therefore, generally be more valuable for clinical testing than rare ones. This makes patent pooling more complicated, because many pools simply count patents rather than try to weight their value, and this may not work for genetic testing even if all the other issues about setting up patent pools were to get resolved. We characterize a penumbra as activities effectively controlled by a patent holder that are not strictly speaking infringing activities but that in practice are effectively controlled by having one or a few patents. The owner of the key patent thereby controls not only their own intellectual property, but collateral space. By this mechanism, a monopoly on the original discovery is leveraged to future discoveries and future patents on new mutations that no one has discovered before, in the clinical penumbra of the originally patented test. All of these options are socially suboptimal by one criterion or another (fairness, efficiency, or both). Finally, when a clinical condition requires testing for mutations or uses methods covered by many patents, this can increase costs due to royalty stacking (because payments to many patent owners are required). The solutions include having a cap on total royalties, clauses in licenses that permit royalty reduction if further licenses become necessary to practice an invention, patent pools, and renegotiation rules. To our knowledge, royalty stacking was not identified as a major problem, although some have wondered about it in interviews. D-3 fi Testing for Connexin 26 gene mutations, which account for up to half of all non-syndromic recessive hearing loss cases, is patented. There is no evidence that patents have had any positive or negative impact on hearing loss genetics research. However there have been intermittent D-4 enforcement efforts by Athena Diagnostics and some laboratories have stopped testing. The test is not offered by any commercial testing providers, including Athena Diagnostics. Athena Diagnostics has negotiated a sublicense with Pediatrix for Connexin 26 testing. Communication and Marketing fi Patents on hearing loss genes and related genetic tests appear to have little to no impact on dissemination of information about genetic testing or on how tests are marketed. However, there has been intermittent enforcement, and some providers have ceased offering some patented tests. We cannot determine how many laboratories decided against offering tests in the first place due to concerns about patent enforcement. Athena states that no sublicenses for hearing loss testing have been negotiated with universities or academic medical centers to date. Consumer Utilization fi We found no evidence that consumer utilization of these tests is impeded by patents. Access for these consumers therefore depends on the availability of additional providers who may have contracts with Medicaid or entails direct out-of-pocket payment by consumers. Adoption by third party payers fi In our informal phone survey, test providers indicated that genetic tests for hearing loss are usually covered by insurance. Hearing loss typically occurs due to abnormalities in single genes or sometimes gene pairs. A multitude of different genes and gene pairs (at least 65 genes and 110 choromosomal 11 locations) have been implicated. Syndromic cases represent about 30 percent of genetic hearing loss cases overall and encompass at least 400 syndromes and a similar number of genes. D-7 locus (chromosomal location, usually a gene) can present as either non-syndromic or syndromic hearing 13 loss. Mutations in different genes may also result in the similar phenotypes (clinical symptoms and 14 signs). We have found no granted patents in Europe, although applications appear to have been filed. In Europe, the exclusive license for 21 Connexin 26 testing went to Nanogen, a provider of molecular diagnostic services. Based on data gathered through our telephone survey of providers (identified through GeneTests. The unit price for the test offered by Athena Diagnostics is in the middle of the price range of non-profit providers (Table 2). Although diagnostic billing codes provide some standardization for full-sequence tests, techniques and procedures are not identical among laboratories. It is also not clear whether patents and exclusive licensing have contributed to a pricing differential or monopoly pricing by a sole provider. To date, seven (six non-profit and one for-profit) providers offer Connexin 30 deletion analysis in the U. Therefore, testing requires testing methods 41 comparable in complexity and price to testing for inherited susceptibility to colon and breast cancer. The two for-profit providers average a higher list price ($355) than the six nonprofit (university hospitals and medical center based) providers (average $210) (See Table 1). A novel mitochondrial point mutation in a maternal pedigree with sensorineural deafness. A pre-test session to explain the causes and types of deafness, along with testing options and modes of inheritance, is important. The diagnosis of non-syndromic cases is more complex, and relies on details of family history and individual symptoms. Given that 10% of deaf infants have culturally deaf parents, the availability of interpreters and the culturally 60 sensitive interpretation of hearing loss test results are critical. After parents are informed of their options, follow-up and additional genetic testing may be recommended. Such imaging studies may include temporal bone imaging, to look for an enlarged vestibular aqueduct and/or cochlear dysplasia. Genetics evaluation guidelines for the etiologic diagnosis of congenital hearing loss. A delay in detecting hearing loss has important implications for language acquisition and limits subsequent choices among management strategies.
Buy discount levitra with dapoxetine 20/60 mg line
Tear replacement is frequently unsuccessful when used as the sole treatment if additional causative factors are not concomitantly addressed erectile dysfunction pump side effects generic levitra with dapoxetine 40/60mg otc. Realistic expectations for therapeutic goals should be set and discussed with the patient. Patient education is an important aspect of successful management of this condition. Table 4 lists treatments of dry eye syndrome according to the type of therapy used. Of these treatments, those particularly effective for evaporative tear deficiency include environmental modifications, eyelid therapy for conditions such as blepharitis or meibomianitis, artificial tear substitutes, moisture chamber spectacles, and/or surgery such as trichiasis/entrpion or ectropion correction and tarsorrhaphy Specific treatment recommendations depend on the severity and etiological factors of the dry eye disease. Management and Therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye Workshop (2007). Table 5: lists treatments for dry eye syndrome based on the severity level of the disease. Mild Dry Eye Potentially exacerbating exogenous factors are to be eliminated: such as: o Long-term use of antihistamines, diuretics, beta-blockers, anti-depressant, etc. Humidifying ambient air and avoiding air drafts by using shields and by changing the characteristics of airflow at work place, at home, and in the car may be helpful. Measures such as lowering the computer screen to below eye level to decrease lid aperture,73 scheduling regular breaks, and increasing blink frequency may decrease the discomfort associated with computer and reading activities. The use of artificial tears may be increased, but the practicality of frequent tear instillation depends on the lifestyle or manual dexterity of the patient. Artificial tears with preservatives may be sufficient for patients with mild dry eye and an otherwise healthy ocular surface. Contributing ocular factors such as blepharitis or meibomianitis should also be treated (see Appendix). Moderate Dry Eye In addition to the treatments for mild dry eye, the following management options may be applied: Artificial tears: Non-preserved tears (or with preservativefree on surface) are important. Anti-inflammatory therapies: may be considered in addition to tears supplement therapies. It also inhibits mitochondrial pathways of apoptosis of lacrimal gland and goblet cells. While the drop is typically well tolerated, ocular burning was reported in 17% of the patients. Patients prescribed corticosteroids for dry eye should be monitored closely for adverse effects such as increase in intraocular pressure, corneal melting, and cataract formation. Systemic Omega-3 fatty acid supplements: It has been reported to be potentially beneficial, but there have been few studies analyzing their efficacy. Study suggested that higher dietary intake of Omega-3 fatty acids is associated with a decreased risk of dry eye disease in women. It can be done surgically with silicone or thermo-labile polymer plugs that are lodged at the punctal orifice. It is important to perform a temporary punctual occlusion first with collagen plugs to test its effect. Soft contact lenses are effective in preventing recurrence of filamentary keratopathy but are poorly tolerated if the patient has severe dry eye. If the patient has associated neurotropic keratopathy, contact lenses should be avoided. Correction of eyelid abnormalities: resulting from blepharitis, trichiasis, or lid malposition. If occlusion with cautery is planned, a trial occlusion with temporary collagen plugs generally should be performed first to screen for the potential development of epiphora. A stepwise approach to cautery occlusion is generally recommended so that no more than one punctum is cauterized in each eye at a treatment session. In general, laser cautery is not as effective as thermal cautery in achieving permanent, complete occlusion. Tarsorrhaphy: may be required to decrease tear evaporation in patients with severe dry eye who have not responded to other therapies. However, these guide lines are helpful to ease the discomfort and further complications. Air conditioning is as bad as heaters for increasing the evaporation of your tears. To wear glasses on windy days and goggles while swimming: the wraparound style of glasses may help reduce the effects of the wind. To position the computer screen below eye level: Computer screen below eye level keeps the eye open narrowly. To use hot compresses and eye massage: Particularly for blepharitis, meibomianitis and related conditions. Follow-up To assess the response of the therapy as a basis for altering/ adjusting treatment as necessary. To monitor for structural ocular damage, and To provide reassurance and constant counselling. The frequency and extent of the follow-up evaluation will depend on the severity of disease, the therapeutic approach, and the response to the therapy. For example, patients with sterile corneal ulceration associated with dry eye may require daily follow-up. In moderate to severe cases that are unresponsive to treatment or when systemic disease is suspected, timely referral to a specialist Ophthalmologist who is knowledgeable and experienced in the management of these entities is recommended. Referral to medical specialist or rheumatologist can be considered for patients with systemic immune dysfunction or for those who require immunosuppressive therapy. The patient and physician together can establish realistic expectations for effective management. Patients with severe dry eye are at greater risk for contact lens intolerance and associated complications. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. Dry Eye: Prevalence and attributable risk factors in a hospitalbased population. Estimating the prevalence of dry eye among Indian patients attending a tertiary ophthalmology clinic. Prevalence of Dry Eye Diseases in hospital-based population in West Bengal, Eastern India. Results of a population based questionnaire on the symptoms and lifestyles associated with dry eye. Blepharitis in the United States 2009: a survey-based perspective on prevalence and treatment. The association of meibomian gland dysfunction and other common ocular diseases with dry eye: a populationbased study in Spain. Prevalence and association of dry eye in an older population: the Blue Mountain Eye Study. Prevalence of dry eye among an elderly Chinese population in Taiwan: the Shihpai Eye Study. Prevalence and risk factors associated with dry eye symptoms: a population based study in Indonesia. Keratoconjunctivitissicca caused by diphenoxylate hydrochloride with atropine sulfate (Lomotil).
Discount levitra with dapoxetine 40/60mg otc
However erectile dysfunction 4xorigional buy generic levitra with dapoxetine 40/60mg line, instead of these signals being purely used to calculate directionality of sound it can also be used in to separate noise and target sources (Carhart 1965). In normally hearing listeners, binaural squelch is probably largely caused by binaural unmasking. A common experimental format includes finding the threshold when noise and signal are presented without a phase difference between the two ears. The signal is then presented out of phase between the ears (p-radian phase difference) whilst the noise remains unchanged. Similarly, when the phase of the noise is changed then there is also significant improvement (approximately 13 dB) although the change is not as great as that of the signal modification (Moore 2003). This can result in an improvement in threshold of up to 12 dB (Bronkhorst & Plomp 1988; Litovsky 2005). This is primarily associated with confusion between masker and target or the reduction in ability to be able to focus attention on the target sound (Best et al. Similarly, if the target and masker had similar speech materials or carry similar meaning the task becomes more difficult to perform. In a paediatric population, conductive hearing loss makes up approximately 4% of the total diagnoses of hearing loss (excluding otitis media), with an additional 5% of diagnoses comprised of mixed sensorineural/conductive losses (Parving 1983). This is of great importance since patients with untreated hearing loss have been shown to report higher rates of anxiety, depression as well as being less likely to participate in organised social activities when compared to those people who wear hearing aids (Hagr 2007; Kochkin & Rogin 2000; Seniors Research Group 1999). This design consisted of a titanium screw, percutaneous abutment and transducer/sound processor. It had many advantages over its predecessors, including improved transmission of sound (particularly high frequencies) and elimination of discomfort occurring due to pressure on the skin via Softband devices (von Bekesy 1960). Between 1985 (when the first 10 cases were reported by Hakansson (Hakansson et al. Firstly, the titanium implant (3-4mm in length) which is usually placed 55 mm behind the pinna into the mastoid, where it osseointergrates. Secondly, an abutment which connects to the implant and protrudes through the skin in order to connect the sound processor and transfers vibrations. In some cases, where strong amplification is required the microphone and transducer are separated so that the microphone is body worn. This allows a more powerful transducer to be placed on the abutment without feedback. In addition to these core components modern bone-conduction hearing implants commonly have the ability to connect to other devices in order to adjust settings and stream sound from a device. Thus, there must be good evidence for benefits in the quality of life in selected patients (Arunachalam et al. They also deliver more reliable audiological outcomes when compared to reconstructive surgery with can be challenging (Marres et al. The major limiting factor is the relative thickness of the paediatric skull which means shorter screw lengths are required. In addition to this challenge is that patients who require such an intervention often have abnormal skull contour or suboptimal bone quality which increases failure of osseointergration rates up to 15% (Granstrom 2000; Tjellstrom & Granstrom 1995; Granstrom & Tjellstrom 1997). Since sufferers have only one working cochlea they cannot process any interaural cues and so lack the ability to derive any of the normal benefits of binaural processing, such as improved sound localisation and understanding of speech in background noise (Wazen et al. Several countries have also approved cochlear implantation as a treatment option (Agterberg et al. Since then, there has been an increasing numbers of patients being treated with this method (Pai et al. This aims to improve the detections of sound when the sound is laterally projected to the deaf side (Bovo et al. Studies consistently found significant improvements in ease of communication and in the background noise domains. In contrast, scores tended to be poorer in the assessment of aversiveness to loud noise (Linstrom et al. The single-sided deafness questionnaire is a further commonly used assessment tool which found that the majority of patients use their devices between 4-7 hours a day and that there was a perceived benefit in quality of life and in hearing (particularly in quiet) (Hol et al. In this experimental configuration there is an improvement in thresholds due to compensation of the head shadow effect. However in 16 the converse condition where speech is directed to the hearing ear and noise the deaf ear, the hearing threshold worsens due to head shadow being compensated for (Martin et al. Since the benefit in noise occurred regardless of a spatial separation between speech and noise, this benefit must be related to improvement in the stimulus audibility, and so might not be sustained if the stimulus were presented at a higher sound level. Scene classification technology, currently used to benefit cochlear implant users (Wolfe et al. When this side was then aided the additional amplification caused the head shadow advantage to be lost. Although it was not clear if these results were significant, as there was high variation between the participants tested. The deficit was thought to be due to crosstalk limiting the ability for central binaural processing to make use of phase difference cues. On this occasion finding an improvement in localisation in those with bilateral severe conductive loss, however this was not significant. Figure 6 Showing acoustic transfer functions between two loudspeakers and a participant (Reproduced from Liao, 2010) 22 In order to mitigate the effect of the crosstalk signal, crosstalk cancellation is required. The crosstalk cancellation technique requires the cancellation of crosstalk signals from each speaker to the opposite ear. This method was initially proposed by Bauer in 1961 before Schroeder and Atal (1963) employed the methodology. Later, Schroeder used the technique in comparative studies in reverberant spaces as well as concert halls (Schroeder 1973; Schroeder 1969). The primary method of constructing a cross talk cancellation filter is to invert the head responses obtained by modelling or direct measurement of the crosstalk signal. Schroeder used a dummy head microphone to construct an inverse filter or crosstalk canceller. This was then convolved with impulse responses from a concert hall and presented in an anechoic room with and without crosstalk cancellation. One of the primary problems in crosstalk cancellation is that sound waves coming from two different sources produce interference patterns. Depending on the distance between and from the ears, the distance between the loudspeakers as well as the frequency, the interference patterns might cause the signal to be destructive, complementary or constructive (Choueiri 2008). In a perfect crosstalk cancellation system (defined by infinite crosstalk cancellation over the audio band) frequencies where destructive interference happens to occur can be compensated. However this requires a level boost at the loudspeakers not just to cause the crosstalk to be cancelled but also for the frequency spectrum to be reconstructed perfectly at both ears with no spectral coloration (Choueiri 2008). However at these frequencies, the level boosts are required are very prone to small errors this causes small movements in head orientation/position to not only loose crosstalk cancellation but to have the additional interference of undesired acoustic artefacts (Nelson & Rose 2005; Takeuchi & Nelson 2002). There are several different methods of crosstalk cancellation including: ideal, adaptive, recursive and fast deconvolution methods (Liao 2010). Equation 1 is expressed in the frequency domain where and vectors of the direct paths and and vectors of the crosstalk paths. In order for the signal from the left and right speaker to reproduced a crosstalk matrix H is needed (superscript signifying the side signal origin and subscript indicating the. In addition to the ill condition there is also a problem when the phases become very similar as a very small movement of the listener would cause the crosstalk to not only stop working but also be detrimental to the signal when compared to not performing cancellation at all (Liao 2010). Thus ideal crosstalk cancellation cannot be achieved in the real world both due to movement of listeners as well as limitations in speaker output. Instead several other strategies are used which make a compromise to ideal crosstalk cancellation in order to make the cancellation method more robust and practical in a real world setting. Although precise costings do not exist for bilateral fittings there would be an additional cost in the region of fi5000-7000. This means that replacement of the device for a newer device would, in the long term, likely be of greater amplification benefit than having bilateral fittings, as well as being significantly cheaper.
Discount levitra with dapoxetine online mastercard
Treatment Since vernal keratoconjunctivitis is a self-limited disease erectile dysfunction causes premature ejaculation purchase levitra with dapoxetine no prescription, it must be recognized that the medication used to treat the symptoms may provide short-term benefit but long-term harm. Topical and systemic corticosteroids, which relieve the itching, affect the corneal disease only minimally, and their side effects (glaucoma, cataract, and other complications) can be severely damaging. Vasoconstrictors, cold compresses, and ice packs are helpful, and sleeping (and, if possible, working) in cool, air-conditioned rooms can keep the patient reasonably comfortable. Patients able to do so benefit from a marked reduction in symptoms, if not a complete cure. The acute symptoms of an extremely photophobic patient who is unable to function can often be relieved by a short course of topical or systemic corticosteroids followed by vasoconstrictors, cold packs, and regular use of histamine-blocking eye drops. Topical nonsteroidal anti-inflammatory agents, such as ketorolac, mast cell stabilizers, such as lodoxamide, and topical antihistamines (see Chapter 22) may provide significant symptomatic relief but may slow the reepithelialization of a shield ulcer. As has already been indicated, the prolonged use of corticosteroids should be avoided. Supratarsal injection of depot corticosteroids with or without surgical excision of giant papillae has been demonstrated to be effective for vernal shield ulcers. Staphylococcal blepharitis and conjunctivitis are frequent complications and should be treated. Recurrences are the rule, particularly in the spring and summer; but after a number of recurrences, the papillae disappear completely, leaving no scars. The symptoms and signs are a burning sensation, mucoid discharge, redness, and photophobia. Giant papillae are less developed than in vernal keratoconjunctivitis and occur more frequently on the lower rather than upper palpebral conjunctiva. Severe corneal signs appear late in the disease after repeated exacerbations of the conjunctivitis. In severe cases, the entire cornea becomes hazy and vascularized, and visual acuity is reduced. Scarring of the flexure creases of the antecubital folds and of the wrists and knees is common. Like the dermatitis with which it is associated, atopic keratoconjunctivitis has a protracted course and is subject to exacerbations and remissions. As in vernal keratoconjunctivitis, it tends to become less active when the patient reaches the fifth decade. Scrapings of the conjunctiva show eosinophils, though not nearly as many as are seen in vernal keratoconjunctivitis. Scarring of both the conjunctiva and cornea is often seen, and an atopic cataract, a posterior subcapsular plaque, or an anterior shield-like cataract may develop. Keratoconus, retinal detachment, and herpes simplex keratitis are all more likely than usual in patients with atopic keratoconjunctivitis, and there are many cases of secondary bacterial blepharitis and conjunctivitis, usually staphylococcal. Chronic topical therapy with mast cell stabilizers, antihistamines, and nonsteroidal anti-inflammatory agents (see Chapter 22) is the mainstay in treatment. In severe cases, plasmapheresis or systemic immunosuppression may be an adjunct to therapy. In advanced cases with severe corneal complications, corneal transplantation may be needed to improve the visual acuity. It is probably a basophil-rich delayed hypersensitivity disorder (Jones-Mote hypersensitivity), perhaps with an IgE humoral component. Use of glass instead of plastic for prostheses and spectacle lenses instead of contact lenses is curative. If the goal is to maintain contact lens wear, additional therapy will be required. Hydrogen peroxide disinfection and enzymatic cleaning of contact lenses may also help. Alternatively, changing to a weekly disposable or daily disposable contact lens system may be beneficial. If these treatments are unsuccessful, use of contact lenses should be discontinued. Until recently, by far the most frequent cause of phlyctenulosis in the United States was delayed hypersensitivity to the protein of the human tubercle bacillus. This is still the most common cause in regions where tuberculosis is still prevalent. In the United States, however, most cases 232 are now associated with delayed hypersensitivity to S aureus. Mild limbal phlyctenule probably secondary to Staphylococcus marginal disease in a 30-year-old female that improved with corticosteroid treatment. Consistent with this difference is the fact that scars form on the corneal side of the limbal lesion and not on the conjunctival side. Phlyctenulosis is often triggered by active blepharitis, acute bacterial conjunctivitis, and dietary deficiencies. Phlyctenulosis induced by tuberculoprotein and the proteins of other systemic infections responds dramatically to topical corticosteroids. A major reduction of symptoms occurs within 24 hours and disappearance of the lesion in another 24 hours. Topical antibiotics should be added for active staphylococcal blepharoconjunctivitis. Treatment should be aimed at the underlying disease, and corticosteroids, when effective, should be used only to control acute symptoms and persistent corneal scarring. Examination of Giemsa-stained scrapings often discloses only a few degenerated epithelial cells, a few polymorphonuclear and mononuclear cells, and no eosinophils. Treatment should be directed toward finding the offending agent and 234 eliminating it. The contact blepharitis may clear rapidly with topical corticosteroids, but their use should be limited. Long-term use of corticosteroids on the lids may lead to steroid glaucoma and to skin atrophy with disfiguring telangiectasis. When associated with a generalized autoimmune disease, usually rheumatoid arthritis, it is known as secondary rather than primary Sjogren syndrome. The syndrome is overwhelmingly more common in women at or beyond menopause than in other groups, although men and younger women may also be affected. The lacrimal gland is infiltrated with lymphocytes and occasionally with plasma cells, leading to atrophy and destruction of the glandular structures. Dry eye syndrome is characterized by bulbar conjunctival hyperemia (especially in the palpebral aperture) and symptoms of irritation that are out of proportion to the mild inflammatory sign, with pain increasing by the afternoon and evening but being absent or only slight in the morning. Rose bengal or lissamine green staining of the cornea and conjunctiva in the palpebral aperture is a helpful diagnostic test. Demonstration with fluorescein staining of punctuate epithelial erosions found in dry eye syndrome due to Sjogren syndrome, with greater distribution of epithelial lesions inferiorly.