
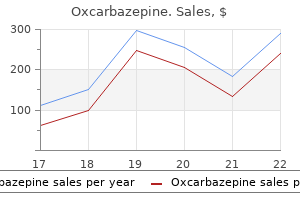
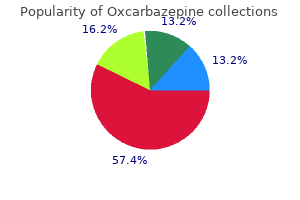
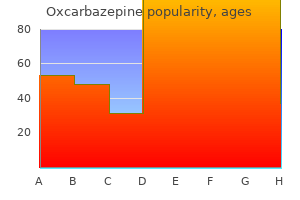
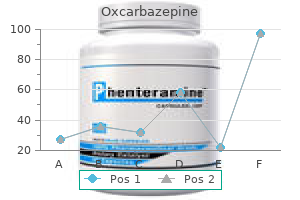
Oxcarbazepine
Order 150 mg oxcarbazepine
Non-24 occurs primarily among blind individuals symptoms 0f gallbladder problems proven 600mg oxcarbazepine, though some sighted persons have the disorder also. For some, Non-24 starts in infancy or early inflexible, and they are unable to entrain to a 24 hour day-night schedule. Still others start out having Delayed Sleep Phase Disorder, and progress to Non-24 as they get older. If a circadian rhythm disorder is suspected, the doctor will Why are some Non-24 people often late for work If they have to get up for work at a time their free running body monitoring sleep-wake patterns using an wrist activity monitor, a device worn like clocks consider sleep time, they may not hear alarm clocks. The sleep history is most useful if it can be awakened, with difficulty, only to fall back to sleep again. This is especially true if obtained when the patient is sleeping on her natural schedule, without attempting they have already become sleep deprived. Many patients will have already researched circadian disorders, and come prepared with a sleep log. People with Non-24 who try to work fixed work hours, such as 9 am to 5 pm, or students who have to attend regular classes, become Often the sleep doctor will order an overnight polysomnogram (sleep study), to sleep deprived. So they may get little or no sleep during the night and be working when the patient can sleep normally, i. In some patients, multiple disorders may be present, or another disorder may be the cause of the reported symptoms. Parents who have Non-24 may have to be awake early in the morning to feed their kids and get them off to school. Sleep doctors treat Non-24 by attempting to entrain the maintaining relationships on such an unusual schedule, shopping when the stores patient to a 24-hour cycle. The patient must first wait until her sleep hours have are open, and being awake for appointments with repair people and doctors. She is then instructed to use bright light in the these are particularly difficult for people whose day length varies, as they cannot morning, restrict light exposure in the evening, and/or take the hormone predict in advance when they will be awake. More awareness that Non-24 is a real disability is needed, together with greater Many doctors prescribe medication to help people sleep. Such people get to sleep when desired, but often it does not improve the quality of understanding would also further efforts to find suitable accommodations. There are many long-term health effects medications and must stop taking them, and some people find them ineffective. These can include depression, lowered immune response, For many Non-24s, sleeping on a normal schedule may be difficult or impossible anxiety disorders, weight gain, fibromyalgia, diabetes, and cancer. They find they can be much more productive and much happier living on the rotating schedule to which their body naturally reverts. But others are chronically For people with severe cases, this may be the only realistic option. Research suggests that some of their internal systems may be out of sync with others for example, Is Non-24 a disability For those for whom treatment is ineffective, Non-24 can their digestive system may not be in sync with their sleep/wake system, similar to make it impossible to maintain a fixed work or school schedule. This material may not be reproduced in any way, including photocopy, without express written permission. Kaiser Permanente has not participated in developing outside publications or Web sites and does not endorse any products or services they contain. Welcome to Kaiser Permanente Living with Fibromyalgia Living with bromyalgia means more than just pain. You may also have stiffness, trouble sleeping, and feel tired, anxious, or depressed. At Kaiser Permanente, we believe in an interdisciplinary approach to helping you with your bromyalgia. At Kaiser Permanente, we avoid the use of opioid or strong narcotic medication for bromyalgia. This booklet provides you with valuable information from our experts in bromyalgia care. Your primary care provider and the interdisciplinary team are here to support you in your health and wellness journey. Effect: easier to fall asleep I do not have to take more than one day off work 1. What: per month because of bromyalgia. Throughout my day, whenever I notice pain or limitations. Other form of relaxation: 3. What: When: When: Effect: Effect: 2. What: When: When: Effect: Effect: 3. Pain causes physical and emotional phenomena that, in turn, cause additional pain. These include changes in neurotransmitter type and balance, synaptic contacts, even possible cell death. Stimuli that were previously not painful may become painful, and pain itself intensies. It has been Fibromyalgia is a common condition that affects two to described since the 1800s under a variety of names: four percent of the U. The professional association of rheumatologists agreed It may start after an infection or viral condition. Notice the movement of your deep breathing while lying down or on your bed or hands. Bend your knees and place your feet a deep breathing, the goal is to have the hand on your comfortable width apart. You may want to stop practicing for a moment and breathe normally close your eyes so you can focus better on the mid until the symptoms pass. This practice Practicing the skill helps to improve concentration and a meditative state. Inhale smoothly through your nose as it helps warm, lter, and moisten the air before it enters the lungs. If using an image helps, picture a balloon in your stomach that inates when you inhale and deates when you exhale. If you time every night, no matter what day of the week share a bed with a restless partner, consider a larger it is.
Buy oxcarbazepine 300mg otc
Incorporation of the pH indicator medicine park oklahoma order line oxcarbazepine, phenol red, reveals colonies fermenting mannitol because acid produced by the colony changes the color of the agar from pink to yellow (Figure 10). Catalase reduces hydrogen peroxide to water and molecular oxygen and the presence Figure 9. Contact between H2O2 and the cells results in the immediate evolution of O2 that can be seen as bubbles (Figure 11). It should be noted that there are two other genera of catalase-positive, gram-positive cocci that are opportunistic Figure 10. Members of the genus Micrococcus are transients of the skin and mucous membranes while Stomatococcus mucilaginosus (weakly catalase-positive) is a commensal of the oropharynx. Stomatococcus mucilaginosus colonies are usually clear to white, mucoid (because of the presence of capsule), and adherent to the surface of the agar. Commercial kits for the rapid detection of clumping factor (cell-bound coagulase) and protein A based on latex agglutination are widely available. In these agglutination tests latex particles coated with fibrinogen and IgG are rapidly agglutinated by S. Management Currently less than 10% of staphylococcal isolates are susceptible to peni cillin. Resistance to this antibiotic is mediated by a plasmid-encoded b lactamase (penicillinase), which hydrolyzes the b-lactam ring of the mol ecule. Catalase test: A, positive; competitively inhibiting the transpeptidase used to cross-link the peptide B, negative. Methicillin is a struc given by Jay Hardy, President of Hardy tural analog of D-alanyl-alanine, and the transpeptidases that are bound by Diagnostics, Glycopeptide antibiotics such as vancomycin act by Staphylococcus binding to the D-alanyl-D-alanine terminus of peptidoglycan precursors aureus preventing cell wall synthesis. Positive and negative thesis of peptidoglycan precursors terminating in the depsipeptide coagulase tests. Vancomycin is reserved for staphylococ cal strains that are resistant to penicillinase-resistant penicillins and clin damycin. Mupirocin may be used to treat superficial or localized skin infections caused by S. In addition to antibiotic therapy, temporary intravascular devices such as catheters should be promptly removed if infection is suspected. Abscesses must be drained and, usually, if the infection involves a prosthetic joint it should be removed. Prevention Prevention of staphylococcal infection relies on the practice of good hygiene. In the hospital setting attempts have been made to eliminate nasal carriage by hospital personnel by the use of antibi otic regimens. What is the causative agent, how does it enter There is a high rate of carriage of methicillin the body and how does it spread a) within the resistant S. Multiple organ Impetigo begins as a small area of erythema that systems are affected such as gastrointestinal, progresses into fluid-filled bullae that rupture and musculature, renal, hepatic, hematologic, and heal with the formation of a honey-colored crust. Bullous impetigo is systemic conditions such as chronic obstructive highly contagious. How is the disease diagnosed and what is the the patient often is febrile and occasionally has a mucopurulent eye discharge. Colonies are round, glossy, domed with an entire edge, and golden Carbuncles are collections of inter-connected yellow in color. There may Determinative tests include: production of be little pain or pain can be throbbing and quite catalase and coagulase; rapid latex agglutination severe. Resistance to Prevention of staphylococcal infection relies on this antibiotic is mediated by a plasmid-encoded the practice of good hygiene. Mupirocin may be Intravascular devices such as catheters should be used to treat superficial or localized skin promptly removed if infection is suspected. Abscesses Low-level resistance to vancomycin, an antibiotic must be drained and, usually, if the infection to which staphylococci had been uniformly involves a prosthetic joint it should be removed. Clinical, microbial, and biochemical aspects of the exfoliative toxins causing staphylococcal scalded-skin syndrome. An exo-enzyme that aids in spreading of bacteria He claims to have felt this way for about 3 days, worse every day. An outbreak of sepsis caused by Staphylococcus aureus Which of the following statements presents the has occurred in the newborn nursery. Development of the syndrome requires infection of a pre-existing burn, not just a cut. Case 34 Streptococcus mitis A 60-year-old male presented at the Emergency Room center) on funduscopic examination (Figure 1A). The was a conjunctival hemorrhage in the left eye patient had a past medical history significant for (Figure 1B). He murmur heard best at the right second intercostal also noted generalized fatigue, myalgia, and arthralgia. He has recently noticed a Extremities: an Osler node was present on the right painful nodule on the tip of his left index finger. Splinter hemorrhages are characteristic of infectious On physical examination, the patient was pale and endocarditis. Close-up of a fingernail showing splinter hemorrhage: dark, thin lines under the nail caused by bleeding. Treatment includes high doses of intravenous antibiotics and, in some cases, surgery to replace the damaged heart valve. Viridans streptococci are responsible for approximately half of all cases of bacterial endocarditis. They comprise a large fraction of the commensal microbiota of the oropharynx and many of them, particularly those that produce extracellular polysaccharide, can cause subacute bacterial endo carditis. As a-hemolytic streptococci are emerging as causes of head and neck infection, and because they are demonstrating increased antibiotic resistance, it is likely that these bacte ria will warrant speciation in the future. The catalase test is used to distinguish streptococci from staphylococci, which are the other principal, medically important genus of gram-positive cocci (see Figure 11 in the Staphylococcus aureus case for the catalase test). As mentioned above, it is difficult to distin guish between certain species of optochin-resistant, a-hemolytic strepto cocci, and to compound this problem there are differences in the ways in which they are speciated by different groups of workers in the field. Viridans group streptococci brane-anchored lipoteichoic acid, except that they lack ribitol or glycerol growing on blood agar. Other than the production of IgA1 protease virtually nothing is known about potential virulence determinants. Optochin susceptibility test for is an inhabitant of the shedding and nonshedding surfaces of the orophar identification of viridans streptococci. If there is a breach in the integrity of the mucosal barrier as a result a-Hemolytic, gram-positive, catalase of tooth extraction, scaling, periodontal surgery or other minor oral sur negative cocci are streaked in bands across gery S. It is worth remembering a blood agar plate and an optochin disc is that even normal chewing results in a transient bacteremia containing placed on each streak. The strains in the center and lower streaks by the bacterium as a member of their endogenous microbiota becomes show a zone of inhibition, indicating that infected when S. There is no they are susceptible to optochin and are horizontal spread of the bacterium from one person to another. During colonization of the oropharynx at birth protection is initially medi ated by the mucous membranes acting as barriers and the large number of innate immune factors present in saliva (see Further Reading: Cole & Lydyard, 2006).
Oxcarbazepine 300 mg with visa
The tissue phase of the infection can also be transmitted congenitally to offspring and to other intermediate hosts through carnivorism medications bipolar purchase generic oxcarbazepine on line. Ingestion of an infected animal will release the brady zoites from the tissue cysts which then infect cells in the new host. The course of the infection is the same whether oocysts or tissue cysts are ingested. In other words, the parasites will go through an acute phase characterized by rapid replication of tachyzoites until the new host develops immunity. This will be followed by a chronic phase characterized by dormant tissue cysts containing brady zoites. Ingestion of an infected intermediate host by the cat will initiate the intestinal stage of the life cycle involving merogony and gamogony in the intestinal epithelial cells. In regards to human transmission, infections are primarily acquired through the ingestion of food of water contaminated with oocysts or the ingestion of undercooked meat infected with tissue cysts. Most infections in the United States and Europe among adults are probably acquired from undercooked meat. The especially high seropositive rate in France (up to 90%) is likely due to a cultural predilection for lightly cooked or raw meat. Toxoplasma can also be transmitted from mother to fetus, often with dire consequences (see below). Tissue cysts from a chronically infected organ donor reactivate when transplanted into a previously uninfected organ recipient. In addition, the immunosuppressive therapy can also reactivate a latent infection in the recipient. Transmission by transplantation is now rare, though, due to screening of donor and recipient before transplantations. Acquisition of tachyzoites from an acutely infected person via blood transfusion is also possible, but rare. Toxoplasmosis in adults and children past the neonatal stage is usually benign and approximately 80% of infected persons are asymptomatic. Acquisition of the infection via either oocysts or tissue cysts results in an acute infection in which tachyzoites are disseminated throughout the body via the lymphatics and hematogenously. Antibody production requires 1-2 weeks and cellular immune ity occurs 2-4 weeks post-infection. Both humoral and cellular immunity are important, but the cellular response appears critical for the conversion from acute (ie, tachyzoites) to chronic (ie, bradyzoites) infection. When symptoms do occur they are generally mild and typically described as mononucleosis-like. A chronic lympadenopathy without fever persisting or recurring for up to a year has also been noted as a symptom of toxoplasmosis. Rarely do immunocompetent individuals exhibit severe symptoms and the acute infection almost always progresses to the chronic stage. This latent chonic-stage infection probably persists for the life of the patient without producing any progressive pathology. Congenital transmission can only occur 8-10% severe brain and eye damage during an acute infection (ie, tachyzoites) acquired moderate-severe visual 10-13% during pregnancy. Mothers with a chronic impairments infection acquired before the pregnancy are not at asymptomatic at birth with some a risk for transmitting Toxoplasma. One-third of 58-72% developing retino-choroiditis or mothers acquiring the infection during pregnancy mental impairments later will pass the infection to fetus. Severity of disease varies with age of fetus and is more severe early in pregnancy. Congenital infection can result in: spontaneous abortion, premature birth, or full-term birth with or without overt symptoms. Typical disease manifestations include: retinochoroiditis, psychomotor disturbances, intracerebral calcification, hydrocephaly, and microcephaly. Twenty percent will exhibit symptoms at birth and 82% will develop symptoms by adolescence. Toxoplasmosis has been long noted as an opportunistic infection in regards to reactivation of latent infections due to immunosuppression associated with organ transplants and certain cancer treatments. Early symptoms of toxoplasmic encephalitis can include headache, fever, lethargy, and altered mental status with progression to focal neurological deficits and convulsions. In other words, the tissue cysts rupture and the release bradyzoites which transform into tachyzoites. The focal lesions are caused by the destruction of host cells in the immediate vicinity of the reactivated tissue cyst. Other forms of the reactivated disease, especially retinochoroiditis, pneumonitis, myocarditis and myositis, may occasionally occur in conjunction with immunosuppression. Diagnosis of toxoplasmosis is rarely made through the detection or recovery of organisms, but relies heavily on serological procedures. Parasites can be detected in biopsied specimens, buffy coat cells, or cerebral spinal fluid. The serologic diagnosis of Toxoplasma is also complex because of the prevalence of sero positive individuals. High antibody titers by themselves are not definitive evidence of an acute infection. Congenital infections are similarly difficult to diagnose serologically because maternal IgG crosses the placenta and persists for several months. Acute infections are characterized by high IgM titers and/or a significant increase in total antibody titer in a sample taken two weeks later. The serology may also correlate with the acute stage symptoms in some individuals. Lack of IgM and lack of changes in the total antibody titers in serial samples is more consistent with the chronic stage of the infection. Most of the patients have multiple ring and/or nodular enhancing lesions with edema. The detection of these lesions combined with serology or symptoms can be used to diagnose toxoplasmic encephalitis. Clindamycine (Cleocin) can be substituted for the sulfadiazine in patient not tolerating sulfa drugs. Symptomatic patients, including those with active retinochoroiditis, should be treated until manifestations have subsided and there is evidence of acquired immunity. Similarly, asymptomatic children under the age of five should be treated for 3-6 weeks to avoid later occurrences of retinochoroiditis. Immunocompromised patients must be treated and therapy should continue for 4-6 weeks after cessation of symptoms. This should then be followed by prophylaxis for as long as the immunosuppression lasts. Corticosteroids to suppress inflammation are co-administered to patients with ocular toxoplasmosis. Acute infections in the fetus or young children may be followed by repeated attacks of retinochoroiditis. If begun early enough, treatment of immunosuppressed patients usually results in improvements, but recrudescences are common. Control measures for toxoplasmosis focus on avoiding the two major sources of infection: o raw meat and material contaminated with cat feces. Cooking meat thoroughly (at least 150 F) and washing hands after handling raw meat will prevent infection with tissue cysts. Activities to reduce infective oocysts include: cleaning the cat litter box within 24 hours, covering sand boxes, and controlling strays. Prevention is especially important during pregnancy when the consequences of infection are most severe. It is especially common in Mexico, Central and South America, south-east Asia, China, elsewhere in Asia, and elsewhere where pig and pork products are consumed. More recently, cysticercosis has become an important parasitic disease in the United States, particularly in California and other states with a large immigrant population from Mexico and Central America. It is estimated that 1000 new cases of neurocysti cercosis will be diagnosed each year in the United States.
Buy discount oxcarbazepine on line
Your chances of triploidy do not increase with Most men carry an X and a Y symptoms detached retina buy generic oxcarbazepine 600 mg on line, and most women carry two Xs. An early copying error is propagated in all subsequent divisions within be copied more than once (duplications), and can get moved from one place to a cell line, resulting in chromosomal abnormalities in some but not all of the another (translocations). Selection is the likely reason: fetuses afected by mosaicism are frequently lost Sometimes inheriting just one mutated copy can cause a genetic disorder-as in during early pregnancy. True fetal mosaicism can cause a large range of clinical outcomes, depending on Other times we have to inherit the same mutation from both parents to have a the chromosomal abnormality involved and which specifc cells are afected. Such muta tions are called recessive, because they cause harm only when two defective copies are present. Trisomies and other aneuploidies are not the only chromosomal abnormalities to consider when choosing a prenatal test. Structural abnormalities, which occur when tiny pieces of single chromosomes are deleted, fipped, or moved during early development, can also cause lifelong mental and physical disability. Other Risk Factors for Aneuploidy Individually, structural abnormalities are very rare, far less common than Down Syndrome, for instance. There is one rare exception: A small percentage of women or their partners who have previously had a fetus with Down Syndrome themselves carry a chro In short, if you want comprehensive testing, consider skipping the screens and mosomal abnormality called a balanced Robertsonian Translocation. You can have genetic testing done to determine if you or your part ner carry a balanced Robertsonian Translocation. We wrote this ebook to Yprovide an in-depth resource with scientifc, evidence-based back ing, to give *you* the power to answer these big questions for yourself, as a parent. The benefts and risks of your options have to be weighed in the context of your life and beliefs. Spon combined ultrasound and biochemical screening for Down syndrome in routine clinical practice. Prediction of miscarriage and combined screening for Down syndrome and other fetal anomalies. Noninvasive prenatal screening for aneuploidy: positive predictive values based on cytogenetic 35. Nonin vasive prenatal testing in the general obstetric population: clinical performance and counseling. The difference is in how the two conditions affect the body, contributing to the difference in symptoms. While both emphysema and chronic bronchitis are both ailments of the pulmonary system, they affect different parts of the lungs, causing different symptoms. Emphysema results when the alveoli are destroyed, usually because of cigarette smoking or some other chemical that is inhaled. The alveoli are small sacs located at the end of the respiratory tree and are where the exchange of oxygen and carbon monoxide take place. They lose their elasticity which causes air to become trapped inside them this explains why exhaling is difficult for a person with emphysema and the damage progressively worsened over time. Mucus forms when the airways are irritated and inflamed, this mucus makes it harder to breath. This causes an increased strain on the heart, eventually leading to right sided heart failure and edema. Cough is a protective reflex and children who have no evidence of illness may cough an It is important however, not to overlook any symptoms that average of 11 times over a day. Also plan a review if the child deteriorates or the Children are not small adults and the causes of cough in cough persists. This should assist with the formation of an accurate Listen to the concerns of parents diagnosis whenever possible and then allow successful management of the cough. Cough in children, regardless of the underlying reason, can cause significant distress, disruption of daily activities and In New Zealand, bronchiectasis and pertussis continue to a lack of sleep for both the child and the parents. Factors such as over-crowding, a Ideas: What do you think is the cause of the cough History and examination guide diagnosis Acute cough is likely to be caused by a viral upper Responses to these questions should help uncover respiratory tract infection parental concerns, suggest areas requiring further direct the majority of children with acute cough will have a viral questioning and guide the type and range of advice given. If the smoke, pets, damp living conditions responses to initial open questions have raised concerns the immunisation status of the child and others in then further direct questioning is required. Complicating that may suggest foreign body inhalation this further is that the initial consultation may be at an Chronic, wet cough with sputum production early stage in an illness when the diagnosis is not clear Continuous, unremitting or worsening cough and there is little indication of the potential severity. A cough associated with a very sudden onset or a history of choking may suggest inhalation of a foreign body, Cough in children can be categorised as: particularly in younger children. It may be overlooked when cases are sporadic and over diagnosed during an epidemic. Nocturnal cough is often a reason for presentation for medical attention because the cough may cause significant Research has shown that subjective reporting of a wet anxiety for the parents, be more noticeable and disturb cough by parents is consistent with findings of airway sleep for the whole family. Although nocturnal cough may Table 2: Neonatal causes of chronic cough9 Diagnosis Features Aspiration (usually milk) A moist cough that follows feeding Irritability, arching or choking after feeds. Usually in a child with an underlying congenital cause such as tracheo-oesophageal fistula or laryngeal cleft. Diagnosis should only be made after other the age of the child when the cough started may be causes have been excluded, such as a transient or important in helping determine the diagnosis. The typical unexplained persistent cough that begins in the neonatal characteristics which may suggest this diagnosis period (the first 28 days of life) requires investigation include: and usually indicates significant disease (Table 2). Discussion with, or referral to , a paediatrician is usually In some cases however, it may be more a recommended. Most cases of foreign body enjoyable activities and be absent during sleep aspiration occur in children aged less than four years. Ask A cough that may occur before speaking and at parents about the potential for foreign body aspiration, times of stress and increases in the presence such as access to any small object or consumption of of parents and teachers small, smooth foods. If the cough may be disruptive to others while foreign body inhalation is suspected then the child should the child appears indifferent to it be referred to secondary care for further investigations. The presence of any associated symptoms absence from school may help determine the underlying cause of a cough. Normal respiratory and heart rates vary Ask about any factors that may trigger the cough with age. Also ask about An assessment of respiratory and heart rate can give environmental factors. Age Respiratory rate Heart rate (years) (breaths/min) (beats/min) Cough that only appears in specific situations. Cough can be triggered in some people by an irritation of the auricular branch of the vagal nerve. In children without (breathe out forcibly) may reveal chest signs that are not symptoms and signs of a specific serious underlying apparent with normal shallower breaths and also may disease process, the recommended approach is to watch, stimulate a cough which enables the quality (dry or wet) wait and review. This may include information on: Sputum the symptoms to expect Sputum culture may be indicated in an older child with the duration of these symptoms a chronic, wet cough. Most young children swallow their sputum and are unable to produce a sample that is of Symptoms and signs of worsening illness sufficient quality to provide useful results. If the child is asymptomatic predominantly lower respiratory infection and be unwell, and normal results are obtained, this does not exclude a with fever, tachypnoea, decreased oxygen saturation and diagnosis of asthma.
Discount oxcarbazepine 300mg without prescription
A model conceptualizing fatigue suggests three different segments of fatigue: Tiredness symptoms celiac disease buy oxcarbazepine australia, Fatigue, and Exhaustion [Olson, 2007]. Tiredness is characterized by forgetfulness, impatience, gradual weakening of muscles and sleepiness improved after rest. Fatigue is characterized by concentration problems, anxiety, gradually reduced endurance unrelated to energy consumption, increased sensitivity, nausea and diarrhea, and limited activity levels for actives regarded as important. Exhaustion is characterized by confusion that resembles delirium, emotional numbness, sudden loss of energy, difficulty staying awake, difficulty controlling body functions and social withdrawal [Olson, 2007]. Fatigue is also reported as a common symptom of other diseases, and has a negative impact on people`s ability to function in daily life [Dittner et al. Meta-theoretical framework critical realism Although method and design are important, it is also important to reflect on the assumptions about reality, particularly as these pertain to methodology [Clark, Lissel & Davis, 2008]. The ontology and epistemology that are chosen may be guidelines when approaching the real world in order to do science [Bhaskar & Danermark, 2006]. The branch of philosophy that has inspired this thesis is critical realism due to that this research project was interdisciplinary, included user-participations and focus group as part of the pilot study and preparation for the main study with quantitative approach and systematic reviews. Critical realism is very inclusive in terms of methods, is intrinsically supporting of interdisciplinarity and enables the possibility of integrating different perspectives and theories [Clark et al. Critical realism is, by philosophical standards, a relatively new approach to ontological, epistemological and axiological issues [Easton, 2010]. In some ways it is diametrically opposed to positivism and social constructivism, but it also seeks to include and transcend the contradictions between these different views. According to critical realism, the bodily dysfunction for example produces impairment, but influence disability and is not merely a social construction. Although disability is a complex phenomenon which is in part caused by socio-cultural attitudes, reducing it to just these set of structures ignores the important bio physical element which cause the physical impairment [Owens, 2011]. Taking the middle ground, critical realism views physical and social entities as having an independent existence, irrespective of human knowledge or understanding [Clark et al. Since a real world exists critical realism holds that some theories approximate reality better than others and that there are rational ways to assess claims to knowledge [Bygestad & Munkvold, 2011a, 2011b]. In critical realism, reality is stratified into three domains (levels of understanding). These include the empirical (fallible human perception and experiences, including science), the actual (events and actions that are more likely to be observed) and the real (underlying power, tendencies, those mechanisms that are productive of different events and other surface phenomena) [Alvesson, 2009; Bhaskar, 1998]. According to critical realism the task of science is to explore the realm of the real (mechanism) and how it relates to the other domains. In this study, we have conducted descriptive research, and according to critical realism descriptive research can sometimes reveal patterns of behavior and social outcome. These patterns invite effort to find causal relationships or social mechanisms that could explain the empirical findings, but we can hardly draw any conclusions of causal nature from our analyses. Thus, it can provide vital descriptive information, which may be useful as support in discussions about causal power [Danermark et al. According to Sayer [1992, 2000, 2004], the best explanations are those identified as having the greatest explanatory power. From the viewpoint of critical realism, mechanisms are viewed as features of something that have the potential power to effect a change. The causality is rarely linear, but more viewed as a product of many factors coming together in certain combinations and given the right circumstances or context to causally generate new events. To explain and understand why phenomena occur, research therefore needs to go beyond the surface of observable factors (the actual) to explore what happens underneath (the real). Put in another way, interpretations rely on assumptions, which together with other assumptions create a system of thinking about the world that we find acceptable [Easton, 2010]. Researchers have to be open to the fact that their explanations must be not only being acceptable to the scientific and wider community, but also changeable. Knowledge of organ pathology is necessary for monitoring, surgery and medical services. Findings from research focused on other hereditary diseases have shown that psychological mechanisms such as stress, anxiety and depression are involved when persons are living with severe life threatening diseases, especially diseases that can be inherited by their children [Geirdal, Dheyauldeen, Harildstad & Heimdal, 2013]. Having chronic pain and fatigue may also cause negative impact on people`s psychological wellbeing and their functioning in everyday life. At the social level, there are several mechanisms connected to living with a severe potentially disabling disease [Danermark, 2001]. Inevitably, this is a complex task because of the range and combined effects of these mechanisms. Some will operate at the individual level, personal level, whilst others are at the societal level. In other words, the effects of these mechanisms will be mediated through people`s day-to-day actions. This is the main reason for that we must abandon any ideas that social work can predict events. In medical social work also the biological and physiological levels plays an important role, in addition to the others. By identifying structures and mechanisms, it is possible to critically analyze and illuminate how they work and how they can be changed [Bhaskar & Danermark, 2006; Danermark & Gellerstedt, 2004]. Following a model based on Danermark & Gellerstedt [2004], we have tried to illustrate some relevant analytical levels in research pertaining to Marfan syndrome in the context of work participation (Table 1). Middle range theories Theorizing is an integral part of the research process and theories may serve as a guiding framework for interpretations [Danermark et al. In line with the ontological and epistemological perspective, as mentioned above, some theories approximate reality better than others. Combining multiple theories generally yields a more complete picture of complex empirical phenomena [Modell, 2015; Zahirul, Mark, Covaleski & Gooneratne, 2015]. The limitations of a particular theory could be addressed by bringing insights from another theory. This implies the need for theoretical pluralism rather than choosing a single theory [Modell, 2015; Zahirul et al. The biopsychosocial theory and model As mention above both the medical and the social models of disability reflect a particular perspective on sickness and disability; all have validity, but each provides only a partial view of human illness [Waddall, 2010; Waddal et al. Tom Shakespeare [2006, 2013] argues that the social model theory has reached a dead end. He emphasises that the dichotomies involve a dangerous polarization of a medical model versus a social model of impairment versus disability and ability and versus disabled people non-disabled people [Shakespeare, 2013]. Neither of these models explains how individuals behave differently with similar health problems, health care, social, and work contexts [Waddell, 2010]. A third model is he biopsychosocial model of disability, developed and introduced by Engel [Engel, 1977, 1980]. Bertalanffy [1969] emphasizes that modern science must think in terms of systems of elements that are in mutual interaction, and that the one-way causality approach has proven to be insufficient. Weiss [1977] argued that system theory is best understood as the logical ordering of nature into more and more complex systems. Here, biological functioning, psychological functioning, and sociocultural functioning are related. Engel, [1977, 1980] argued that the biomedical aspect is important, but how people perceive and communicate their symptoms is influenced by psychological and social/cultural factors.
300mg oxcarbazepine overnight delivery
Available at: as first-line and maintenance treatment for patients with chronic medications zanaflex order oxcarbazepine 150 mg with mastercard. Available at: translocations and karyotype complexity in chronic lymphocytic. Available at: karyotype predicts for inferior outcomes following reduced-intensity. Richter syndrome: Molecular insights and chronic lymphocytic leukemia subcommittee of the chronic leukemia clinical perspectives. Available at: working party and lymphoma working party of the European group for. Two main genetic pathways lead to the transformation of chronic lymphocytic leukemia to Richter 184. Genetic lesions associated with chronic lymphocytic leukemia transformation to Richter 185. Available at: Expansion of Resistant Subclones Precedes Relapse during Ibrutinib. Management of chemotherapy or chemoimmunotherapy with or without stem-cell adverse events associated with idelalisib treatment: Expert panel Version 3. Idelalisib given front-line for treatment of chronic lymphocytic leukemia causes frequent 194. Immunoglobulin replacement in patients with chronic lymphocytic leukaemia: A comparison of two 198. Available at: reactivation in cancer patients undergoing cytotoxic chemotherapy: A. Available at: management of cytomegalovirus reactivation in patients with chronic. Available at: reactivation during alemtuzumab therapy for chronic lymphocytic. Available at: weekly intravenous ganciclovir as cmv prophylaxis in heavily pre-treated. Hepatitis B virus reactivation in B-cell lymphoma patients treated with rituximab: Analysis from the asia 211. How I treat and monitor viral Hepatitis B infection in patients receiving intensive immunosuppressive therapies or 212. Blood patients with chronic lymphocytic leukaemia treated with fludarabine, 2009;113:3147-3153. Valganciclovir prevents cytomegalovirus reactivation in patients receiving alemtuzumab-based 213. Available at: autoimmune phenomena and disease stage and therapy in B-cell. Rituximab for chronic lymphocytic leukemia: Prevalence, clinical associations, and immune cytopenia in adults: Idiopathic thrombocytopenic purpura, prognostic significance. The prognostic significance of a positive direct antiglobulin test in chronic lymphocytic leukemia: A 223. Rituximab therapy for beneficial effect of the combination of fludarabine and chronic lymphocytic leukemia-associated autoimmune hemolytic cyclophosphamide on the incidence of hemolytic anemia. Available at: thrombocytopenia on the clinical course of chronic lymphocytic. Rituximab efficacy and safety in adult splenectomy candidates with chronic immune thrombocytopenic 218. Cyclosporin a for the purpura: Results of a prospective multicenter phase 2 study. Rituximab treatment patients with chronic immune thrombocytopenic purpura: A double-blind of refractory fludarabine-associated immune thrombocytopenia in randomised controlled trial. Successful treatment of pure red cell aplasia with care in patients with immune thrombocytopenia. Thalidomide and lenalidomide-associated thromboembolism among patients with cancer. Lenalidomide plus dexamethasone versus thalidomide plus dexamethasone in newly diagnosed multiple myeloma: A comparative analysis of 411 patients. Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: An open-label randomised controlled trial. Inflammation, tnfalpha and endothelial dysfunction link lenalidomide to venous thrombosis in Version 3. Similarly, In general, leukemia is the most common cancer other types of leukemia have been reported in workers in children. Other inherited affected child may look pale, be often breathless and diseases are also associated with a higher risk bruise and bleed easily and for a prolonged period of of developing leukemia such as: Fanconi anemia time. Aside from addressing the symptoms of leukemia, medical treatment designed to cure involves chemotherapy, interferon therapy and in certain cases a designated monoclonal antibody. The objective of this research was to synthesize studies that characterize the clinical and epidemiological profile of patients with leukemia, the types of treatments used, duration and outcomes for the cases. There were 4,274 articles rescued in the initial search, 188 were selected to compose the review sample after applying all the criteria for inclusion and exclusion adopted. Full articles were grouped into four categories, according to the variables of research: (a) more frequent subtypes of leukemia; (b) most widely used treatment; (c) duration of treatment; and (d) endpoint of the cases. Keywords: leukemia; lymphoma; epidemiology; hematologic neoplasms; multiple myeloma; prognosis; drug therapy. El objetivo de esta investigacion fue sintetizar los estudios que caracterizan el perfil clinico y epidemiologico de los pacientes con leucemia, los tipos de tratamientos usados, la duracion y los resultados para los casos. Habia 4 274 articulos rescatados en la busqueda inicial, se seleccionaron 188 para componer la muestra de revision despues de aplicar todos los criterios de inclusion y exclusion adoptada. Los articulos completos se agruparon en cuatro categorias, segun las variables de investigacion: (a) los subtipos mas frecuentes de leucemia; (b) el tratamiento mas utilizado; (c) la duracion del tratamiento; y (d) el punto final de los casos. En general, la poblacion masculina se ve mas afectada por neoplasias hematologicas. Palabras clave: leucemia; linfoma; epidemiologia; neoplasias hematologicas; mieloma multiple; pronostico; quimioterapia. Among the cancers that affect the general population, leukemia has events from childhood to the elderly stages. Leukemia is responsible for approximately 3% of all cancer cases in Brazil and worldwide3. However, it does not interfere with the production of normal cells, as in the previous type6. Given the importance of this issue and the social impact generated by the diagnosis and treatment of this disease, this study aims to summarize the studies that characterize the clinical and epidemiological profile of patients with leukemia, the type of treatment used, duration and outcomes for the cases. For the execution of searches of electronic databases, the following research question has been defined among the leukemia subtypes, which is the most common, the most common treatment, duration and outcomes found The literature search took place between December 2015 and January 2016, using the proxy licensed by the Federal University of Rio Grande do Norte ( Uncontrolled search was performed only in Science Direct base to obtain a representative sample of published articles that met the inclusion criteria. Articles that were not available in full on the selected databases, studies of literature review type, reflective articles, previous notes, letters to the editor, pilot studies and qualitative research were excluded, as well as those who did not answer the main question of this study. The first selection of studies was carried out by reading the titles and abstracts, with emphasis on objectives and results. For data extraction, the classification of items according to the information presented was carried out: prevalence, treatment, outcome, incidence and treatment, incidence and outcomes, treatment and outcome and incidence/treatment/outcome. In an initial search, there were 4 274 articles rescued, 188 of them were selected for the sample of this review after application of the inclusion criteria. Of the 4 086 studies excluded, 3 970 addressed the topic, but not on the topics of interest to this review, 28 articles were duplicated, 61 were literature review articles, and 27 had scientific events. There were 62 studies on the prevalence of the disease, 7 addressing kinds of treatments, 53 addressing the outcomes, seven on the prevalence/treatment/outcomes, three prevalence/treatment, 33 on the prevalence and outcomes and 23 addressing the treatments and their outcomes. Studies published between 1964 and 2015 were rescued, of which 135 articles were published in the last ten years. After systematic reading, the complete articles were grouped into four categories according to the variables of research: (a) more frequent subtypes of leukemia; (b) most widely used treatment; (c) duration of treatment; and (d) outcomes of the cases. Leukemia is approximately one-third of cancer cases in children aged 0 to 14 years old and 10% of adolescents aged 15 to 19 years old.
Order oxcarbazepine 150 mg with mastercard
Pulmonary cellular glycolysis and oxygen uptake following phosgene exposure are depressed and symptoms in dogs discount oxcarbazepine 150mg without prescription, thus, leads to a corresponding decrease in the levels of intracellular adenosine triphosphate and cyclic adenosine monophosphate (Sciuto et al. This is associated with increased water uptake by epithelial, interstitial, and endothelial cells (Helm, 1980). The semipermeability of the blood-air barrier becomes gradually compromised as a result of fluid entering the interstitial and alveolar spaces. Later, the blood-air barrier disrupts, opening channels for the flooding of alveoli (Diller et al. Compression of pulmonary microvasculature leads to the opening of arteriovenous shunts (Schocimerich et al. The onset of pulmonary edema correlates temporally with the decrease in adenosine triphosphate levels (Currie et al. Interventions that increase intracellular cyclic adenosine monophosphate, such as treatment with phosphodiesterase inhibitors. Lung lavage fluid total and differential cellularity and viability were determined at 0, 4, 20, or 44 hours after exposure. Phosgene at 1 ppm significantly decreased lavage fluid cell viability at all time points but resulted in transient decrease at 0. The authors concluded that phosgene induced alterations in arachidonic-acid metabolism may be involved in its toxicity. The authors concluded that phosgene stimulated the synthesis of lipooxygenase products of arachidonic-acid metabolism, which appear to contribute to pulmonary edema. Increased thromboxane production occurred in human pulmonary microvascular endothelial cells after phosgene exposure in vitro (Cheli et al. Neutrophils migrated to the lung surface in large numbers following phosgene exposure in several animal species (Robinson, 1994; Schroeder and Gurtner, 1992). Pre-exposure injections of cyclophosphamide, which significantly reduced circulating neutrophil counts, also decreased neutrophil migration to the lungs and limited phosgene-induced edema and mortality (Ghio et al. The above studies shed some light on the postulated mechanisms of phosgene toxicity; however, they are inadequate to define modes of action at the cellular level. A single epidemiology study of phosgene-exposed workers (Polednak and Hollis, 1985; Polednak, 1980) was not considered adequate for evaluating carcinogenic potential in humans. Furthermore, no animal cancer bioassays of phosgene have been conducted to evaluate carcinogenic potential in experimental animals. Phosgene has been identified as a reactive intermediate in the metabolism of a number of chemical carcinogens, including chloroform (Pohl et al. Covalent binding of phosgene with cellular macromolecules has been proposed as a mechanism of chloroform-induced hepatic and renal toxicity (Pohl et al. Possible Childhood Susceptibility No published studies are available to evaluate the effects of phosgene exposure on children or young experimental animals. Possible Gender Differences No published studies have directly compared the effects of phosgene inhalation exposure in males and females. Other No published experimental animal or human epidemiological studies are available to evaluate the effects of phosgene in the geriatric population or in individuals with compromised disease conditions, such as asthmatics or those with respiratory impairments. Therefore, exposure by the oral route is unlikely and the lack of data precludes derivation of an RfD. The RfC is an estimate (with uncertainty spanning perhaps an order of magnitude) of a daily exposure to the human population (including sensitive subgroups) that is likely to be without appreciable risk of deleterious effects during a lifetime. Like the RfD, the RfC is based on the assumption that a threshold exists for certain toxic effects. Therefore, the RfC cannot be directly compared to average air concentrations without also examining available benchmarks regarding acute effects from the inhalation of phosgene (see Appendix A). Use of these approaches has the potential to add multiple dimensions of information that include the slope of the dose response curve and the severity of effect. Choice of Principal Study and Critical Effect(s) In the selection of principal studies for identifying critical endpoints of phosgene toxicity, two studies are relevant for deriving the RfC: Selgrade et al. These are subchronic inhalation studies with periods of recovery following exposure. Both studies have limitations, not being of chronic duration; however, they have similar exposure protocols and used the same experimental animal strain (F344 rats) to measure two different endpoints (immune response and pulmonary damage). The most sensitive target organ following chronic inhalation exposure to phosgene appeared to be the lungs. The investigators observed statistically nonsignificant terminal bronchiolar changes and interstitial thickening of the alveolar walls, inflammatory cell influx, and epithelial alterations of the terminal bronchioles at 0. These effects were not statistically significantly increased after a 4-week recovery period; they may be adverse, but they are not persistent. Phosgene is toxic to the immune cells that are in the lungs, but after phosgene exposure stops, the cells repopulate the lung from elsewhere in the body and no permanent damage to immune system cells is evident. It appears that concentration rather than exposure duration is the more critical factor for the extent of toxic response to phosgene, even at these low concentrations. Lung hydroxyproline content and trichrome staining for collagen are standard methods for measuring lung fibrosis and can be considered reliable chronic injury markers. Support for this is found in the present study, which showed lack of reversibility of the collagen accumulation and possibly even a progression during the 4-week recovery period, terminal bronchiolar thickening and inflammatory cell influx, and an increase in the lung displacement volume. Measurements of hydroxyproline in the whole lung, which is considered to be a chemical manifestation of fibrosis, were statistically increased in the high-dose group (1 ppm) only and were persistent after the recovery period. Concentration seems to be more important than duration in determining this pathology response. Collagen staining increased slightly at 4 weeks and increased markedly at 12 weeks in both the 0. Although this assumption is uncertain (see discussion in paragraph 2 below), there is no reasonable alternative assumption. This approach is used when a biologically based dose-response model cannot be formulated. A benchmark analysis was performed for lung effects considered to be adverse, as discussed in Sections 4. The means and standard deviations for this endpoint were obtained in an e-mail dated October 22, 2001, from Dr. However, the exposure group size of eight rats per exposure group is not conducive to obtaining response estimates below 10%. In this case, the multistage model provided the best fit of all the dichotomous models (see Appendix B) to the endpoint characterized as increased collagen staining of terminal bronchioles. Total dose is equal to the concentration (C), which is proportional to the rate at which the agent is delivered to the cells, multiplied by duration of exposure (T). A more detailed examination of these data reveals that hydroxyproline concentration in the 12-week study increased with both C (at fixed T) and T (at fixed C), and it also increased with the product of C T. The experimental data are not definitive enough to derive a numerical description of the dose response surface. There are no data for collagen staining or for hydroxyproline resulting from daily exposures in the range from 1 hour per day to 24 hours per day. However, two studies employing continuous exposure show that toxic effects are proportional to the C T product. Therefore, it is likely that collagen staining would also follow the C T product for exposures of fractions of a day. However, the assumption is made here that continuous exposures for 7 days per week would have the same effect as intermittent exposures for 7 days per week. Therefore, in the standard default method for adjusting for continuous exposures, the traditional 5/7 factor is not needed. This is the standard procedure for dose conversions from animals to humans for Category 1 gases, which are completely and irreversibly absorbed by the lung (U. The thoracic region, which consists of both the pulmonary and tracheobronchial regions of the lungs, was chosen for three reasons. Second, some of the assays measured would not make a distinction between the two lung regions.
Purchase oxcarbazepine overnight delivery
Some initial sleep loss and increased sleep pressure is central to the efectiveness of this therapy symptoms urinary tract infection purchase oxcarbazepine. But during the frst weeks of therapy it is most important to keep the same wake-up time. Instead, on Sunday morning go for that morning walk you never have time for, or get up early and read the newspaper before the rest of the family, or meet friends for breakfast (ideally al fresco in the sunshine). Cognitive therapy aims to change your thoughts and beliefs about your sleep that will, in turn, help you feel more confdent and less anxious and sleep better. Correct your Understanding of Sleep I Just being aware of what is a normal sleep pattern for your age can help. It is unrealistic and unnecessary to get rid of them in order to feel fne during the day. The aim is not to get rid of them but to be able to get back to sleep within a few minutes. Some also say they think they have forgotten how to sleep as if it is something that requires learning to do it. We saw that negative learning (conditioned insomnia) can interfere with the normal sleep mechanism. Research, including some of our own, has shown that good sleepers assume they have been awake already when awoken out of sleep on about 30% of awakenings. However, people with insomnia perceive over 70% of awakenings as simply a continuation of being awake. That is, two separate brief awakenings can be seen as one long awakening with the conclusion that you were awake a long time across the night. For example, in the Roller Coaster Sleep diagram below there are two brief awakenings, one at about 4 a. Therefore, correctly perceiving an awakening from sleep can help protect against insomnia. If you cannot remember much, you can tell yourself that you just woke up and had not been awake for very long. These thoughts and feelings can lead to behaviours that, in fact, increase sleeping difculties. However, this will lead to more time awake in bed that will result in more anxiety. But it will help to remember the following: I the natural sleep pattern is like a roller coaster with 90-minute cycles in and out of deep and light sleep with several brief awakenings spaced across the normal sleep period. So you can see how these beliefs can play a role in perpetuating insomnia and, therefore, working to reduce these beliefs can be therapeutic. However, this strategy is not efective when trying to sleep the harder you try to do it, and the more anxious you become about it, the more elusive it becomes. Failure to get good sleep with these attempts also has the detrimental efect of creating feelings of helplessness and mild depression. Sleep is a basic biological mechanism that will operate best if we stop trying to force it. Often, when people look back at the end of their day, they fnd it has been productive and satisfying, despite feeling very tired in the frst half hour after awakening. Your grogginess might have been no more than the natural sleep inertia experienced upon awakening from sleep. Therefore, if you experience this early morning grogginess of sleep inertia you can tell yourself you were probably having some deeper sleep that will be benefcial to you throughout that next day. Some people may fnd it useful to think about or to actually write down some of their sleep-re lated anxiety producing thoughts. However, If you can change these thoughts to more positive thoughts, you will feel less anxious and more confdent about your sleep. You may like to write down some of your negative thoughts and then practice coming up with an alternative, more positive thought. It is not easy changing the automatic thoughts since they happen without your intentions. They all focus attention on a non-provoca tive process, such as breathing, a pleasant or neutral image, an internalised word, etc. This focus of attention prevents other intrusive thoughts from entering your consciousness, thus avoiding worry about these thoughts and allowing relaxation and sleep. It is important to choose a technique or focus of attention you feel comfortable with. Likewise, relaxation is a mental skill that needs practice to become skilled and maintain the attention focus for longer periods of time. Thoughts are likely to intrude into your consciousness many times while trying to maintain a relaxed state. Be mindful of them, just recognise that it has occurred and regain your focus of attention. Try to fnd about 10 minutes each day to practise before trying to use the technique at night to help you sleep. With practice the length of time you can maintain your focus without intrusive thoughts will get gradually longer and longer. That will allow your alertness to drop steadily until you cross the threshold into sleep. In fact, relaxation techniques and meditation are very helpful for falling asleep and can be used for that purpose. It is best to listen to these audio lessons out of bed rather than when you are attempting sleep. Learn them to the point of being able to hear the instructions in your mind while you are in bed. People then fnd they have to either increase their dose to get the same efect or have to change to another type of sleeping medication. For this reason some practitioners recommend medications on alternate nights only. The patient then experiences better sleeps on pill nights and poor sleeps on non-pill nights. Of course the poor sleep on non-pill nights will increase sleep pressure and help to ensure better sleep on the next night and add to the efect of the pill. Although this alternating pattern might reduce physio logical dependence, the strong association of good sleep with the pill and poor sleep without may produce psychological dependence. Some longer acting sleep medications have a less noticeable rebound efect during withdrawal. However, because they can carry over into the nest day, they can produce a range of daytime side-efects such as drowsiness, dizziness, fatigue, memory loss, reduced ability to concentrate and confusion. These side efects, and an increased risk of falls make them problematic particu larly for older adults.