
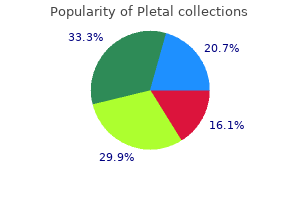
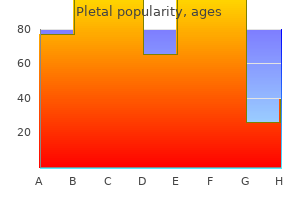
Pletal
Buy 50 mg pletal fast delivery
This would meet the needs of an acclimatized worker producing six to eight kilograms of sweat containing one to two grams of salt during a single shift muscle relaxant parkinsons disease order cheap pletal on-line. During the period of acclimatization, a worker with no previous heat exposure might require supplemental salt because, although maximal sweat rates in unacclimatized workers are lower (four to six kilograms per sweat), salt concentrations are higher (three to five grams per kilogram of sweat) than after acclimatization. Despite the difficulty of trying to equate time spent in physical conditioning, drills, or field exercises with shifts, a similar magnitude of loss may be experienced by military personnel. A salt deficit of 15 to 25 grams may occur during the first several days of increased thermal stress. If field rations are consumed as meals, supplemental salt is not required because each ration, including the accompanying salt packet, contains 31 grams of salt, and daily dietary intake of salt may reach 93 grams. Naval Flight Surgeons Manual An individuals greatest need for salt would occur during the simultaneous stresses of initial physical conditioning and heat acclimatization in a. Costill, Cote, Miller, Miller, and Wynder (1975) found minimal physiological benefit in supplementing drinking water with electrolytes when sufficient quantities of those ions were available in the daily diet, and subjects were permitted to ingest food and drink ad libitum. A physiological plasma sodium chloride level can be achieved by providing adequate water, a normal diet, and a salt shaker on the table for conservative use, with no more than the equivalent of two grams of supplementary salt (preferably not as salt tablets) per day. Progressive dehydration may occur if water is replaced without concurrent replacement of salt because homeostatic controls are designed to maintain a balance between the electrolyte concen trations of the extracellular and intracellular fluid compartments. The renal tubules then fail to absorb water, and dilute urine con taining little salt is excreted. Thus, electrolyte concentration of the body fluids is homeostatically maintained but at the cost of depleting body water and ensuing dehydration. Under continued heat stress, symptoms of heat exhaustion develop similar to those resulting from water restriction but with more severe signs of circulatory insufficiency and notably little thirst. Many authors have reported an excessive intake of alcohol by patients within hours or a day or two prior to the onset of heat stroke. Striking reductions in workers heat tolerance on the day following alcoholic excesses have been described. Hyperthemic Illnessthe classification of hyperthermic illness used in this chapter is the one agreed upon jointly by committees representing the United Kingdom and United States in 1964. A summary of the etiology, signs and symptoms, treatment, and prevention of heat illness is presented in Table 20-6. Heat stroke is a bona fide medical emergency, and if treatment is not instituted immediately, the mortality rate is high. It occurs when the thermoregulatory mechanisms fail for reasons as yet undetermined. The central drive for sweating becomes inoperative, and cooling by evaporation is lost. There is an uncontrolled accelerating rise in Tc due to uncompensated heat storage. Predisposing factors include any of those which adversely affect tolerance to heat. Pro dromal symptoms are headache, malaise, discomfort perceived as excessive warmth, or even those symptoms associated with heat exhaustion. The onset is usually abrupt with sudden loss of consciousness, convulsions, or delirium. Typically, sweating is absent, and the patient himself may have noted this prior to the onset of his other symptoms. Since the patient may continue to ingest water in the absence of sweating, overhydration rather than dehydration may occur. Should diuresis occur as a result of this, it should be interpreted as an additional sign of the critical condition of the patient. During the early stages of heat stroke, the patient may experience a febrile euphoria once sweating has ceased and Tc has risen. Physical signs are a flushed, hot, dry skin; in severe cases, there may be petechiae present secondary to direct thermal injury or vascular endothelium which initiates platelet aggregation. The patients pulse is full and rapid, while the systolic blood pressure may be normal or elevated, and the diastolic pressure may readi ly become depressed. As the patients condition worsens, peripheral vascular collapse may occur manifested by a rapid pulse, hypotension, and cyanosis. If the patient survives until the second day, recovery often occurs, but relapses may occur in the first few days after the temperature has been reduced from the critical level. Otherwise, water should be sprinkled over the patient and its evaporation hastened by fann ing. In addition to these cooling measures, attendants should rub the victims extremities and trunk briskly to increase circulation to the skin. The patient should be transported as soon as possible to a facility properly equipped to perform definitive treatment. During transportation, cooling efforts should be continued by permitting passage of air currents through the open door of the field ambulance or helicopter. Once the patient reaches the hospital, he should be placed immediately into a tub of water and ice. Rectal 20-42 Thermal Stresses and Injuries temperature should continue to be monitored every ten minutes until stable. During the first several days, the patient is susceptible to hypothermia as well as relapses of hyperpyrexia. Rapidly increasing temperatures can usually be managed with ice water sponge baths and fanning; precipitous drops in temperature may require judicious use of warm blankets. Shivering is associated with increased involuntary muscular activity which is undesirable because it accentuates tissue hypoxia and lactic acid acidosis. If simple warming measures fail to control shivering, the physician may administer small intravenous doses of diazepam (10 mg. Central venous pressure, serum electrolytes, and hourly urinary output must be carefully monitored to avoid hyperhydration. Replacement fluids should be sufficient to repair imbalance of serum electrolytes and to restore acid-base balance, but care must be exercised to detect early signs of pulmonary congestion, rising venous pressure, or renal failure. Administra tion of oxygen by face mask or nasal catheter may be useful to combat tissue anoxia. Convulsions may be controlled by intravenous use of diazepam or short-acting barbiturates (sodium pen tothal). Serious physiological damage and altered response to heat stress may persist long after recovery from heat stroke. There is evidence to suggest that heat stroke victims may be more susceptible to recurrent episodes of heat illness under less intense environmental conditions. Therefore, they should never be returned to heat stress similar to that which precipitated their illness without an evaluation and appearance before an appropriate Medical Board. Heat hyperpyrexia is a milder form of the same illness in which there is partial, rather than complete, failure of the central drive for sweating. Treatment is directed towards lowering core temperature as in heat stroke, but due to the less severe nature of the illness, less drastic measures may be adequate. Heat syncope is the clinical manifestation of circulatory hypostasis and is an entity familiar to military medical personnel. It is most commonly seen in personnel standing in parade formation in hot outdoor climates. Naval Flight Surgeons Manual enforced immobility of standing in parade formation. The syncope results from a pooling of blood in dilated vessels of skin and lower parts of the body. The momentary cerebral ischemia is relieved promptly once the patients posture becomes horizontal as a result of the faint, and recovery is complete once the patient is moved to a cooler area. Disorders of salt and water depletion include the clinical entities of heat exhaustion and heat cramps. These conditions are most commonly seen in unacclimatized personnel who have sweated profusely while performing heavy exertion under conditions of ther mal stress. The sweating mechanism remains functional under adequate central drive, but the pa tients have mismanaged the replacement of water and salt lost in sweating. Patients with heat exhaustion suffer peripheral vascular collapse as a result of dehydration and depletion of circulating blood volume. The depletion of the circulatory blood volume may be absolute and secondary to failure to replace water and salt lost in sweat, or relative due to circulatory strain from competing demands for blood flow to skin and large skeletal muscles.
Buy generic pletal online
Sigurdsson V et al: Erythroderma: A clinical and follow-up study of 102 patients spasms piriformis purchase pletal 50mg with mastercard, with special emphasis on survival. In adults, the symptoms are more severe dilemma in that both noninfectious and infectious causes and include prolonged fever, malaise, and arthralgias. Among the noninfectious causes already a few days after onset of illness, small erythematous macules discussed are drug eruptions, vasculitis, and exfoliative ery appear on the trunk, face, and proximal extremities. In addition, systemic lupus erythematosus, juve mary lesion evolves rapidly into a clear vesicle that, if left nile rheumatoid arthritis, and Kawasakis disease may be undisturbed, becomes cloudy. Pruritus neous reactions that, in general, are not pathognomonic is often intense. Healing with scarring is not uncommon, either for infection or for a specific organism. Cutaneous manifestations of sepsis were addressed pressed individuals, varicella may be especially severe and earlier. In such patients, Three to 5 days later, discrete erythematous macules secondary bacterial infection is an added risk. Culture of a lesion may con this media, pneumonia, viral myocarditis, liver function firm the diagnosis but requires approximately 10 days of abnormalities, and thrombocytopenia. An immunofluorescent antibody test using materials from a lesion is also available. General Considerations Rubeola is an acute epidemic disease characterized by Differential Diagnosis marked upper respiratory symptoms and a widespread ery Varicella may be confused with widespread impetigo, dis thematous maculopapular rash. It is caused by a paramyx seminated herpes zoster, disseminated herpes simplex, ovirus transmitted by inhalation of infected droplets. The lesions in smallpox begin as red macules and Clinical Features evolve in synchrony through vesicular and pustular stages, and they predominately affect the face and extremities. Cool compresses and antihistamines may help to ings, including urticarial plaques, petechiae, and palpable remove crusts and alleviate pruritus. The complication and case-fatality rates for respiratory infection to fulminant septicemia. Peak incidence ofthe clinical presentation in immunocompromised patients infection is in the winter and spring. One-third of such patients present nization of the nasopharynx is common and provides a with no rash. Measles virus may be isolated from the blood, urine,the cutaneous lesions are a consequence of damage to small nasopharyngeal washings, and throat or from conjunctival dermal blood vessels both by direct bacterial involvement of secretions. Treatment Therapy is supportive because no proven antiviral agent is Clinical Features available. The onset may be are other treatment options for measles pneumonitis and insidious, following a flulike illness, or abrupt, with fever, encephalitis. Obtundation, hypotension, and death may ensue within hours despite Meningococcemia appropriate antimicrobial therapy. Absence of meningeal signs is a feature of this acute fulminant form of meningo coccal disease. Petechial (or, less commonly, urticarial or morbilliform) Other complications of invasive meningococcal disease rash on the trunk and lower extremities; also on the are arthritis, myocarditis, pericarditis, cervicitis, and palms, soles, and mucous membranes; petechiae are Waterhouse-Friderichsen syndrome. More rare meningo frequently palpable, with gun-metal gray centers and coccal diseases include occult bacteremia and chronic irregular borders. If complicated by purpura fulminans, extensive hemor rhagic bullae and areas of necrosis. This Other features of meningococcal meningitis or dissemi may be by culture, Gram stain, or immunologic tests. Confirmation of Neisseria meningitidis by culture, Gram Counterimmunoelectrophoresis or latex agglutination with stain, or immunologic tests. Other laboratory General Considerations studies are otherwise nonspecific but should be performed N. Meningococcal infection must be considered in patients with the combination of fever and a petechial rash, espe Clinical Features cially in association with meningitis. Vasculitis and other causes of purpura also are myalgia, and nausea or vomiting are initial features. Bilaterally sym Hemodynamic and other supportive measures must be pro metric petechiae of the palms and soles is a major finding. However, these tests are not reliably positive before the second week of the illness. A Giemsa stained smear of tissue sections occasionally may demon strate the organism. Gangrene of the earlobes, Diagnosis can be confirmed by serologic tests, but these digits, nose, etc. The major indication for operative treatment is fasciitis spreading despite empirical antibiotics in an acutely ill patient. Typically occurs following surgery or penetrating trauma; diabetes may be a predisposing condition. Mehta S et al: Morbidity and mortality of patients with invasive Severe systemic toxicity is usually present. The pathogenesis involves the introduction of organisms into the subcutis with subsequent spread through fascial planes. Rapid onset of fever, vomiting, watery diarrhea, sore throat, and profound myalgias, with hypotension. The infection spreads rapidly and deeply, result mation of the involved skin and of the palms and soles ing in local tissue ischemia. The extremities are the most commonly affected site, but the trunk, perineum, General Considerations and abdomen also may be affected.

Generic 50mg pletal fast delivery
The therapeutic range long-term use muscle relaxant allergy purchase pletal 50 mg free shipping, thus limiting its usefulness to situations in for warfarin depends on the indication for which it is used, which only short-term anticoagulation is required. There is also significant variability of antico and is excreted in urine and bile. The anticoagulant effect of agulant response during long-term therapy in individual warfarin is not immediate. In addition, elderly patients appear to be more sensitive patient characteristics and preferences. More fre reduces the risk of recurrence compared with 6 months of quent monitoring is advisable for elderly patients, those who therapy from 20. Numerous drugs influence the anticoagulant effect of treatment of patients with peripheral arterial embolism and warfarin through multiple mechanisms, and bleeding unre may prevent thrombosis of peripheral arterial bypass grafts lated to the anticoagulant effect of warfarin may result from in high-risk patients. Antiplatelet agents are preferred over effects on other hemostatic pathways (eg, aspirin and other warfarin for the prevention of acute myocardial infarction in antiplatelet drugs and heparin), as well as effects on intestinal patients with peripheral arterial disease; for prevention of mucosa (eg, aspirin). The frequency of monitoring should be risk of cerebral hemorrhage if blood pressure is not moni increased in patients taking warfarin whenever new medica tored and controlled. Warfarin is not better than aspirin for tions are started to allow proper dose adjustments. Warfarin is effective for management of multiple is often used to prevent thrombosis of vascular access thromboembolic conditions and is used when long-term catheters in cancer patients and to prevent thrombosis asso anticoagulation is required. Candidates for long-term anti ciated with thalidomide therapy, but efficacy has not been coagulation include those with artificial heart valves, chronic established for these situations. Depending on the patients risk for also may increase the cumulative risk of bleeding. Management of hemorrhage associ warfarin therapy (ie, dose, monitoring, adjustment, and peri ated with warfarin is similar to that encountered with operative management). Included in Table 39-9 are sug heparin in terms of using clinical criteria to determine the gested strategies for reversal of warfarin when time does not urgency of the situation. Initial dose: 5 mg/d (lower in patients who are elderly, on multiple medications, malnourished, or have liver disease). Supplement with fresh frozen plasma or prothrombin complex concen trate if needed. Patients who are known to be defi gangrene, abdominal pain, and renal and other visceral cient in protein C or protein S should receive warfarin only infarctions owing to cholesterol emboli. Warfarin crosses the placenta and may result in fetal Patients who cannot tolerate warfarin may be treated with bleeding. These metabolites substituted prior to pregnancy (except for women with may cause a red-orange discoloration of the urine. Warfarin does not cause anticoagulation in hours, and it is cleared slowly from circulation with a half-life infants who are breastfed by mothers taking warfarin. Like warfarin, its anticoagulant effect can be Other infrequent side effects of warfarin include alopecia, reversed by vitamin K and fresh-frozen plasma. In patients with crosses the placenta and causes fetal malformations and fetal underlying arterial vascular disease, warfarin therapy has bleeding, so it should be avoided during pregnancy. Thrombolytic therapy may be used in the treat agents is complex and involves many components of the nat ment of acute arterial thrombosis, including myocardial urally occurring fibrinolytic system. Thrombolysis can improve neu 2 free plasmin, which results in degradation of fibrin and other rologic function in patients with acute nonhemorrhagic stroke coagulation factors. Only an Thrombolytic agents are also used to reestablish patency of estimated 2% of all stroke patients are able to receive clotted indwelling venous catheters and vascular grafts. Streptokinase increases antithrombotic agents, and choice of specific agent for throm early mortality and intracerebral hemorrhage when used in bolytic therapy are evolving. Thrombolysis reduces mortality the treatment of acute stroke and is not recommended. Bolus fibrinolytic agents, stroke who are more than 3 hours from the onset of symp reteplase and tenecteplase, are potentially advantageous toms. This approach has an even higher risk of hemorrhage because they can be given quickly and could be available in the (10% overall), but in centers equipped with a stroke unit and prehospital setting. Reteplase appears to be equivalent in safety all necessary personnel and technologic support quickly and efficacy to alteplase, whereas tenecteplase has a somewhat available, it may prove to increase the number of patients lower rate of major bleeding. Any available fibrinolytic agent who could benefit from thrombolysis for acute stroke. When cost-effective analyses have been done, improvement in overall outcome compared with anticoagu streptokinase appears to be marginally more cost-effective than lation alone. Urokinase exchange abnormalities, or significant impairment in right is used primarily for dissolution of catheter thromboses. Echocardiography to assess right ven-the principal goal of fibrinolytic therapy is to reestablish tricular function plays a key role in determining the potential patency of an occluded blood vessel (or indwelling catheter). The role of heparin combined with fib severe venous occlusion and threatened gangrene of the rinolytics for patients with acute myocardial infarction is limb. Despite a high rate of clot lysis, there is no good evi controversial, and the combination appears to be associated dence that thrombolytic therapy reduces the rate of post with a high rate of major bleeding. Antiplatelet agents have been shown to be very arterial thrombus in medium and large peripheral arteries. Platelets play fibrinolytic agent administered through a catheter proximal a key role in the development of coronary thrombosis. Surgery can be recently completed will provide additional information avoided in 35% of these patients, and overall mortality about the safety and efficacy of various combinations of appears to be somewhat better than with immediate surgery. In addition, the combination of venous catheter without excessive pressure, which could dis reduced-dose fibrinolytic therapy with invasive coronary lodge the clot or rupture the catheter. Hemorrhagic complications can be Alteplase is approved for use in acute nonhemorrhagic minimized if patients are selected properly and monitored stroke and is effective when administered intravenously carefully. Thrombolytic therapy ence with danaparoid during pregnancy to determine its ter results in decreased plasma fibrinogen concentration and atogenicity. Maternal bleeding occurs with the same increased fibrin degradation products, but these tests are not frequency as in other situations requiring anticoagulation predictive of efficacy or clinical bleeding. Bleeding can complicate deliv if prolonged, may correlate with minor bleeding but is not ery. Intracerebral hemorrhage is more common in patients cause an anticoagulant effect in babies who are breastfed by who are elderly or underweight, who have prior neurologic mothers taking warfarin. Guidelines for the management of disease, or who are receiving antithrombotic drugs. Women antithrombotic agents during pregnancy are outlined in appear to have a higher risk of intracerebral hemorrhage.
Discount pletal 100 mg free shipping
Patients who have had ear surgery or manipulation of the stapes may have all the usual findings muscle relaxant anticholinergic order pletal australia, except nystagmus. In isolated serous labyrinthitis, there is usually return of labyrinthine function over weeks or months. If any fistula is suspected or injury occurred in surgery, systemic antibiotics are in dicated. With fistulas, there is often a permanent nerve-type hearing loss, and some patients have chronic positional vertigo. Suppurative labyrinthitis results in violent and sudden onset of vertigo, disturbed equilibrium, nystagmus, and vomiting. Complications such as men ingitis or brain abscess lead to toxic symptoms of headache, malaise, and fever. Vigorous therapy with antibiotics and surgery must be instituted, and some small mortality can be expected even with treatment. For those who recover, there is usually no recovery of the cochlear or vestibular responses, and three to five weeks are required for compensation. It is often impossible to be sure of complete eradica tion of disease, and there is questionable compensation of loss of hearing and labyrinthine func tion and occasional residual ataxia. Naval Flight Surgeons Manual Toxic labyrinthitis is one of the most common types seen, and a great deal of disagreement re mains about its classification. The etiology ranges from acute febrile diseases to toxic or chemical substances to idiopathic. The most common characteristic is whirling vertigo with gradual onset reaching a maximum in 24 to 48 hours, and at its height, there may be nausea and vomiting. There may be no cochlear or vestibular abnormalities in those cases associated with or following acute febrile illness, but when associated with drugs, either system may be affected. Most commonly, toxic labyrinthitis is associated with pneumonia, cholecystitis, influenza, allergy, extreme fatigue, overindulgence in food or alcohol, and certain ototoxic drugs (Table 8-5). Palliative treatment with antivertiginous drugs (Table 8-6) and bed rest is helpful. The physi cian should always be aware of a missed or changing diagnosis with these patients. Table 8-5 Ototoxic Drugs 8-20 Otorhinolaryngology Table 8-6 Antivertiginous Drugs Epidemic Vertigo. Although to a great extent this disease may be of central origin, it is impor tant to differentiate if from other vertiginous conditions, and this can often only be done by ex dusion. Characteristically, symptoms are acute onset of severe dizziness, nausea, vomiting, a slight fever, headache, and asthenia, with a duration of several weeks to months. There is usually an epidemic character to the disease, and it is associated with either an upper respiratory infection or gastroenteritis. Caloric and audiological tests usually are normal, but spinal fluid may show some lymphocytic cells. Cases with gastrointestinal symptoms are more frequent in mid-January, and those with upper respiratory symptoms occur in the autumn. Naval Flight Surgeons Manual Treatment is supportive, with variable help from antivertiginous and antinausea drugs such as Dramamine, Vontrol, Torecan, and Tigan. These patients should be able to return to flying within one month after all symptoms have ceased. Vestibular neuronitis is characterized by an attack of sudden, debilitating vertigo, nausea, vomiting, and spontaneous nystagmus. In most cases, there appears to be an antecedent or concomitant infection in the upper respiratory tract, maxillary sinuses, or teeth. Vestibular symptoms decrease somewhat after a few hours, but they remain fairly severe for the first week, slowly decreasing over the next four to eight weeks. Management is directed toward supportive treatment of the symptoms and an aggressive workup to rule out other possible diagnoses. Vestibular neuronitis is a self-limiting disease, although return to work may require from three to twelve weeks. Generally, an aviator is per manently grounded for military flying because of the sudden debilitating nature of the attacks which can be recurrent even as long as four years after the initial attack. Although much disagreement persists as to whether this is a disease or a symptom complex, and its etiology is still unknown, there is usually the classical triad of episodic vertigo, tinnitus, and deafness. The average age of onset is 44 (Cawthorne & Hewlett, 1954), and it is predominantly unilateral, with only about ten percent of the patients having bilateral involve ment. The onset of symptoms is insidious, usually with a sensation of dullness or fullness in the ear, and an initial fluctuation in hearing of 10 to 30 dB, usually in the low tones. The hearing improves somewhat between attacks, but it continues to deteriorate as time goes on. Tinnitus, varying from a whistle to a roar, develops, followed by a turning or whirling vertigo that may lead to nausea, vomiting, and even prostration. Any head movement aggravates the condition, with the vertigo lasting several hours. Some patients can have fleeting attacks lasting several minutes, and still others have attacks lasting a week or longer and may take months to regain normal equilibrium. Besides the fluctuating hearing, spontaneous nystagmus, usually rotary and often direction changing, and a direction-fixed, positional nystagmus are the most common findings. Aside from the hearing loss, Menieres patients frequently have recruitment and diplacusis, low threshold discomfort, and low discrimination scores. A fairly reliable diagnostic test is the glycerin test, where a pa 8-22 Otorhinolaryngology tient ingests 1. Audiograms are taken immediately and at one, two, and three hours after ingestion. A positive test is said to be an improvement in hearing of 15 dB in any one frequency from 250 to 4000 Hz or 12 percent improvement in the discriminating score. For many years, some physi cians have controlled their patients with a neutral-ash, salt-free diet, supplemented with diuretics. Shea (1975) recommends a regimen of bed rest, Valium, low salt, diuretics, and no smoking, plus inhalation of five percent carbon dioxide and 95 percent oxygen for 30 minutes q. Other drugs, given individually, that are reported to be effective for an acute attack are l/150 grain Atropine I. Vasodilators, such as nicotinic acid, beta-pyridylcirbinol, Roniacol, or Arlidin, are usually ineffective in Menieres, as are the antivertiginous drugs. There have been several surgical treatments for Menieres with some success in a certain percentage of patients. These range from the endolymphatic shunt to destructive labyrinthotomy in the most severe, uncon trolled cases. Patients with a diagnosis of Menieres are permanently grounded, and only the pa tient with a rare surgical cure has ever been allowed to fly by the Federal Aviation Agency. An acoustic neuroma is a fairly rare, extremely slow-growing neoplasm that originates on the vestibular portion of the eighth cranial nerve in the internal auditory canal. It constitutes about eight to ten percent of all brain tumors and is most common in the fourth and fifth decade of of life. Early diagnosis, which offers the best chance for a surgical cure and the least morbidity and mortality, is often based on a strong suspicion. Symptoms, often difficult to pinpoint but most often present, are steady, unilateral tinnitus, hearing loss, and a feeling of unsteadiness. Some patients have vague complaints of headache, local retroaural discomfort, and facial paresthesia or pain. A significant finding is speech discrimination much more severe than indicated by a pure-tone hearing test. Diagnostic evaluation should include a complete audiological examination of pure tone and speech, stapedial reflex, and acoustic reflex decay. Naval Plight Surgeons Manual Suspected cases, which are not diagnostic should be kept under the watchful eye of an otolaryngologist or neurologist and not dismissed or forgotten after the initial workup. Benign paroxysmal positional vertigo must be differen tiated from Menieres and eighth nerve tumors. In general, onset of nystagmus and vertigo occur when the head moves to a certain position. There usually is a latent period of several seconds, and the nystagmus fatigues with repeated testing.
Buy pletal from india
Signs of central neurological dysfunction include diplopia spasms meaning in urdu buy discount pletal 50 mg on line, ataxia, dysphagia, dysphonia, or sensory or motor complaints. Important historical factors include prior head injury, recent viral infection, toxic exposure, or medication use. Physiological Substrates of Vertigo Spatial orientation is accomplished by utilizing sensory information from the visual, vestibular, and somatosensory systems, which are processed in the brain stem, then finally integrated into the cortical perception system. Disruption or altered processing of signals from the visual, vestibular, 7-26 Neurology or somatosensory system may cause disorientation or vertigo. For example, a patient who has undergone cataract extraction may have distortion of his visual system and may be profoundly disoriented. A patient with a peripheral neuropathy may have a diminished sense of propriocep tive input from joints and muscles, resulting in substantial disequilibrium, particularly in a low light situation, where the reduction in visual input further degrades orientation. Vertigo is defined as a hallucination of movement or erroneous perception of self or object motion. It is usually an unpleasant sensation due to distortion of static gravitational orientation perceived by the cortical spatial perceptional system. This erroneous perception of motion of person or environment may be linear or angular (rotatory). This section will focus primarily on the vestibular system and its relationship to vertigo and disequilibrium. The orientation function of the vestibular system is twofold: 1) maintenance of postural tone and 2) stability of visual ocular position. The utricle and saccule are linear accelerometers detecting linear motion in the front to back (transverse) plane and side to side (saggital) plane, respectively. These linear motion detectors provide input to the postural maintenance section of the vestibular system. This vestibulospinal system is responsible for maintaining an erect posture and counteracting the effects of gravity on body position. The angular accelerometers, the semicircular canals, provide input to the oculomotor system, which maintains ocular stability, particularly during movement. Linear accelerometers are found in such primitive creatures as the jellyfish, and angular accelerometers are found in such primitive creatures as the octopus. As animals evolved evolutionarily, these linear and angular accelerometers became more sophisticated. Vertigo and disequilibrium may result from a mismatch of sensory signals from either the static or dynamic spatial orientation systems. There is overlap among the visual, vestibular, and somatosensory signals that are centrally processed. Central compensatory mechanisms enable deficiencies in one area to be overcome by other intact sensory systems. As a result of this reprocessing of signals by the central nervous system, symptoms of peripheral labyrinth dysfunction will eventually recover. Symptoms of central nervous system dysfunction, although usually milder, tend to persist over time. The intensity of the vertiginous or disequilibrium sensation is a function of the degree of mismatch between functioning and dysfunctioning or nonfunctioning sensory systems. Because of the interaction between the various central processing systems, other symptoms besides vertigo may be experienced. Vertigo may be due to excessive physiological stimulation or pathological dysfunction. Gait imbalance or ataxia results from inappropriate or abnormal signals from the vestibulospinal system. Nausea and vomiting may occur from activation of the chemoreceptor trigger zone (medullary vomiting center). Naval Flight Surgeons Manual observed with dysfunction of the vestibulo-ocular brain stem processing center or peripheral vestibular system. Physiological Vertigo Syndromes In physiological vertigo the sense of disequilibrium is due to physiological excess of visual, vestibular, or somatosensory signals which cannot be compensated for by the other systems. In pathological vertigo there is an abnormal sensory signal (from the sensors) or abnormal signal processing (by the central nervous system). Examples of physiological vertigo (due to inap propriate stimulation) include motion sickness, space sickness, height vertigo, visual vertigo, somatosensory vertigo, head extension vertigo, and bending over vertigo. These physiological vertigo states have significance in aerospace medicine, particularly the type of motion sickness seen in neophyte fliers airsickness. With a head movement in one direction, the visual scene should move in the opposite direction. As we have evolved in a one G horizontal plane, we are accustomed to gravitational movements in the horizontal plane only, not the vertical plane. The angular accelerometers (semicircular canals) sense turns and the linear accelerometers (otolith organs) detect to and fro and side-to-side mo tion. Motion sickness appears to be worse at frequencies of vibration or oscillation from 0. Although infants under age two are quite resistant to motion sickness, it becomes a pro blem particularly in the adolescent and young adult. Motion sickness is worsened by removing or altering the surrounding visual environment. Motion sickness is worse in aircrew, particularly Naval Flight Officers, who stare at their instruments, when the outside reference horizon is lost (instrument flight conditions), or during rapid changes in aircraft attitudes. This may be augmented by reducing anxiety (relaxation techniques, reducing life stress), keeping well hydrated, getting a good nights sleep, engaging in regular exercise, eating regular meals, and avoiding tobacco, caffeine, and alcohol. In aviation personnel who wear contact lens it is important to continue to wear the same contacts and not alternate between contact lenses and glasses because this will change the vestibulo-ocular reflex and make one more prone to visual conflict. In aviators who only wear their glasses at night, they may develop motion sickness and disorientation for the same reason. One of the most effective medications is scopadex (25 mg of scopolamine hydrobromide with 5 mg of dexamphetamine). Phar macological intervention is a temporizing measure and a positive effect should be seen within 7-28 Neurology three to five doses, and should be used in conjunction with continued flight training to be max imally effective. In the balance practice, the patient stands in the tandem posi tion with one foot in front of the other with the head extended (as if looking at the ceiling), hands placed across the shoulders and the eyes closed. Enhancement of this test can be performed by standing on one foot, which is extremely difficult. This test enables the person to become habituated to sensory stimuli without visual input. This position places the linear accelerometer (otolith organs) outside of their normal range of sensitivity and may allow the patient to adapt to sensory conflict. Inflight techniques for managing airsickness include avoiding hyperventilation, establishing a reference horizon, and going on 100 percent oxygen. The most important con sideration with airsickness in flight is to maintain flight safety (aviate, see and avoid other air craft) and establish crew coordination. Space sickness probably results from vestibular mismatch be tween the otolith organs and the semicircular canals, or the side to side difference in otolith input in the microgravity environment. Space sickness occurred in 35 percent of Apollo astronauts, 60 percent Skylab crew, and has plagued 67 percent of the Space Shuttle missions, where over 50 percent have moderate or severe symptoms. It seems to occur when astronauts engage in free movement, unlike the restrained position in the space capsule of the Mercury and Gemini mis sions. It begins 15 minutes to six hours after launch, but may be delayed up to 48 hours, with peak severity occurring two to four days into the flight. Height Vertigo Height vertigo is a type of physiological vertigo due to visually induced instability and occurs when the observer is a certain height above the ground where stationary objects in the visual field are far off in the distance. Height vertigo usually occurs above three meters and reaches its max imum at 20 meters of height. Ordinarily, the body has a normal amount of body sway which is constantly being corrected for. Naval Flight Surgeons Manual body sway must occur before a movement is detected and compensated for.

Chinese RR (Rehmannia). Pletal.
- Are there any interactions with medications?
- Diabetes, anemia, fever, osteoporosis, allergies, or other conditions.
- Dosing considerations for Rehmannia.
- How does Rehmannia work?
- What is Rehmannia?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97099
Buy pletal 50mg without prescription
A metabolic acidosis with an increased anion gap age drug rehabilitation programs back spasms 40 weeks pregnant cheap 100 mg pletal visa. If the adolescents may be found with which of the following agents are suicidal, obtain psychiatric consultation once they following a toxic exposure Cyclic antidepressants and fab fragments Erickson T, Kulig K: Gastric Decontamination. Cyanide and methylene blue Toxicology: Diagnosis and Management of the Poisoned Child. B-blockers and glucoagon Erickson T, Thompson T, Lu J:the approach to the patient with an unknown overdose. Single-dose activated charcoal hyperthermia secondary to neuroleptic malignant is the most efficacious mode of gastric decon syndrome. Agents that classically produce a metabolic acido be indicated following large iron, lead paint chip sis with increased anion gap include iron, salicylates, and drug packet ingestions. Gastric lavage may still cyanide, carbon monoxide, metformin, methanol, be indicated following a potentially life-threatening and ethylene glycol. Cyclic antidepressants are effectively ergic toxidrome, which is most consistent with treated with sodium bicarbonate administration, diphenhydramine (benadryl) ingestion. Other anti while Fab fragments are indicated for digitalis cholinergic agents include cogentin, jimson weed, toxicity. Methylene blue are sympathomimetics producing hyperthermia, is indicated for symptomatic methemoglobinemia. Glucagon effectively reverses Methadone and phenobarbital produce an opioid and the clinical effects of b-blocker toxicity that includes sedative hypnotic syndrome, respectively. After a therapeutic dose, 90% of the drug starting on about day 5, and go on to complete is metabolized to inactive sulfate and glucuronide recovery. Less than 5% is excreted unchanged in sive encephalopathy, renal failure, coagulopathy, the urine. It is most of 140 mg/kg followed by 17 additional doses of effective if started within 8 hours after an acute 70 mg/kg given at 4-hour intervals. Persistent vomiting that interferes with therapy can be suppressed with metoclopromide 1. Which of the following statements about the stages all situations: acute overdose, repeated (chronic) of acute acetaminophen toxicity is true Marzullo L: An update of N-acetylcysteine treatment for acute acetaminophen toxicity in children. Persistent vomiting that interferes with quent, but indicative of a poor prognosis. Standard doses of activated charcoal can be given if the patient arrives within 1 hour of ingestion. Enteric-coated preparations will also Magnesium salicylate have delayed absorption. Wait two more hours and repeat the salicylate the plasma level in patients who chronically receive level. This level is about 7 hours doses of 10 to 20 mL/kg until adequate perfusion is after ingestion. The aspirin is still being absorbed because of its nate in an initial bolus of 1 to 2 mEq/kg followed by anticholinergic effects. Aspirin follows linear kinetics since the repeat + Obtain serial arterial or venous blood gases. The units are incorrect as the level should be and in patients with underlying disease states that will 1. A 2-year-old boy is brought in by parents who found the child playing with an empty bottle of baby aspirin. The child had appeared well until he late in the presentation, so this is to be expected started vomiting 30 minutes ago, which has since and does not affect management. Observe two hours, if the child looks well and is aspirin causes a nonanion gap metabolic aci no longer vomiting send him home. You should begin a bicarbonate drip to increase obtained for which of the following indications in the ionized fraction of salicylate and increase this patient Which of the following is correct regarding aspirin may compromise salicylate elimination. Tachypnea results from stimulation of the res bottle of aspirin in a suicide attempt after getting piratory center. Also, the management of this patient is which of the fol time of ingestion may be incorrect. The goal in systemic alkalinization is to increase sure that the clinical presentation is consistent with the urine pH above 7. Potassium is exchanged for hydrogen in the may have been more than 10 tablets in the bottle. Aspirin does taste bad but it is amazing and has a metabolic acidosis several hours after what some kids will eat. Aspirin actually distributes more quickly to organs such as the brain, lung, Michele Zell-Kanter and kidney in children than in adults. Treatment will not be effective unless electro and epigastric pain, all of which can occur at thera lytes are appropriately replaced. If the patient is hypoka rotoxicity, including acute tubular necrosis, acute lemic, the kidney will hold on to potassium and interstitial nephritis, and acute renal failure. Aspirins pharmacokinetics change to zero clinical symptoms, an arterial blood gas is indicated. Tolmetin has a propensity for causing seizures vomiting soon after drinking the charcoal. Ibuprofen has a propensity for causing seizures to begin drinking the charcoal again. Give the patient an antiemetic and then have the meningitis patient begin drinking the charcoal again.
Buy pletal cheap
Complex partial be an afebrile seizure quinine spasms cheap pletal 100 mg on-line, the rapid return to normal seizures result in impaired consciousness and level of consciousness makes this less likely. Motor involve Without a documented fever, this cannot be a ment is not always present, complex somatosen febrile seizure. A tic is a movement disorder sory symptoms such as numbness, tingling, or without loss of consciousness. A pseudoseizure paresthesias of an extremity, or visual phenom tends to be a diagnosis of exclusion, but the ena are always present. Autonomic symptoms patient often avoids painful stimuli and returns to include sweating, change in heart rate, pupil a normal level of consciousness after the seizure. A meticulous attention to maintaining patency of simple partial seizure results in no impairment the airway and adequacy of oxygenation and in consciousness. Oral suctioning may be required, so preceded by blurred vision, followed by a loss this should be available. A pseudoseizure tends to be is administered to all patients via non-rebreather a diagnosis of exclusion, but the patient often mask or bag-mask ventilation. Venous access avoids painful stimuli and returns to a normal is secured as soon as possible. A bedside glucose check with centrotemporal spikes, also known as benign should be performed on all patients to detect rolandic epilepsy, has an onset between 3 and hypoglycemia. Other laboratory studies are based 13 years of age and is the most common partial on the type of seizure, history, and likely etiologies, epilepsy syndrome in children. A lumbar puncture upon awakening, and consists of facial move should be performed in any patient suspected of ments, grimacing, drooling, and vocalizations. Neuroimaging should be reserved for those spasms), is characterized by sudden symmetric with a postictal focal deficit (Todds paralysis) that bilateral tonic contractions of the extremities, does not quickly resolve, a child whose level of head, and trunk. The onset is at 5 to 12 months consciousness remains decreased, or who has not of life, with spasms occurring upon falling asleep returned to baseline mental status within several or after awakening, with occurrences a few times hours. Patients who have had a febrile seizure may be discharged, with follow-up Chest pain is a worrisome symptom that often causes by their primary care provider, unless an underly parents to bring their child to the emergency depart ing infection precludes discharge. If a metabolic abnormality source, whereas adolescent patients usually have 10 such as hypocalcemia (<7 mg/dL) is found, it chest pain of psychogenic origin. Prostaglandin A pain (>6 months duration) usually have idiopathic or is the treatment for a cyanotic infant with a ductal psychogenic chest pain. Diazepam for home use is not appropri if they have a history of congenital heart disease, ate in this case. Carbamazepine (Tegretol) is including chest pain, dyspnea, dizziness, nausea, the only one of these drugs in which a therapeutic vomiting, and fatigue. Physical examination unaffected side and the practitioner reaches under may reveal decreased breath sounds or rales. The etiology is unclear, + Physical examination may reveal decreased breath but is thought to occur from the parietal pleura, inter sounds and crepitus. Males are more often affected than females Local nerve blocks, corticosteroid injections and sur B. Patients with chronic chest pain usually have a ible chest pain elicited by palpating the costochon cardiac etiology dral joints. Supraventricular Tachycardia she experienced the acute onset of right sided chest B. Antibiotics be the most sensitive and specific test to detect myo cardial injury You suspect your pediatric patient is having a myo usually 10 to 12 years of age. Tietzes syndrome is an inflammatory condition 2 mm of the costochondral junctions, and not related to C. The other tests would not be specific for myocardial There is no history of foreign body ingestion or injury. She is stable so immediate needle decompression or chest tube placement is not needed and a chest film is reasonable to evaluate the extent of the pneumothorax. If unsuccess + posttraumatic (including instrumentation and for ful, surgical consultation mandated. At your exam, the infant seen as persistent diarrhea followed by the appear is afebrile, consolable, and well appearing. Discharge home with parents and instructions + High dose steroids to administer a vegetable based laxative. Discharge home with dietary instructions of + Nasogastric tube bananas, applesauce, toast, and arrange for + Parenteral antibiotics follow-up with pediatrician in 24 hours. Physical exam reveals an afebrile infant in no distress, abdomen is soft and Brown L, Jones J: Acute abdominal pain in children: classic nondistended with a small round mass palpable in presentations versus reality. Discharge home with instructions to continue ing strategies for the diagnosis of appendicitis in children. A 3-year-old is brought by parents for vomiting gist whether an air/barium enema should be and abdominal pain, which is intermittent in nature. Give oral liquid Physical exam reveals a listless afebrile child who challenge to child. The abdominal oral liquids are well tolerated, discharge home exam is soft and nontender. Rectal examination is with specific instructions to return should strongly positive for occult blood. The next appro child resume vomiting or abdominal pain priate management step should be returns. Discharge home with laxative and instructions tion and discharge home if child appearance to follow-up with pediatrician if not improved improves and tolerates oral liquids. Perform ultrasonography and evaluate for a tar reveals a soft abdomen with a 2 cm mass noted in get or bulls eye on transverse or cross section the right scrotum. Discharge home with instructions to collect be considered should be: stool for culture. A 6-month-old presents with colicky abdominal following sedation attempt to relocate the mass pain which results in bouts of inconsolable cry using continuous bimanual pressure. Administer antibiotics, perform lumbar punc shaped mass in the right lower quadrant. Obtain a testicular ultrasound and consult films are done which reveal air fluid levels but no urology.

Purchase pletal cheap online
This is due to the ability of cocaine to prevent reuptake of catecholamines into the adrenergic neuron; thus back spasms 6 weeks pregnant order pletal 100mg on-line, like norepinephrine, epinephrine remains at the receptor site for longer periods of time (see Figure 6. This may lead to an increase in peripheral resistance and an increase in blood pressure. Inhalation anesthetics: Inhalational anesthetics sensitizethe heart to the effects of epinephrine, which may lead to tachycardia. The weak I2 activity of norepinephrine also explains why it is not useful in the treatment of asthma. Baroreceptor reflex: In isolated cardiac tissue, norepinephrine stimulates cardiac contractility; however, in vivo, little if any cardiac stimulation is noted. This is due to the increased blood pressure that induces a reflex rise in vagal activity by stimulating the baroreceptors. This reflex bradycardia is sufficient to counteract the local actions of norepinephrine on the heart, although the reflex compensation does not affect the positive inotropic effects of the drug (see Figure 6. Effect of atropine pretreatment: If atropine, which blocks the transmission of vagal effects, is given before norepinephrine, then norepinephrine stimulation of the heart is evident as tachycardia. Therapeutic uses: Norepinephrine is used to treat shock, because it increases vascular resistance and, therefore, increases blood pressure. However, metaraminol is favored, because it does not reduce blood flow to the kidney, as does norepinephrine. Norepinephrine is a potent vasoconstrictor and will cause extravasation (discharge of blood from vessel into tissues) along the injection site. The duration of action is 1 to 2 minutes following the end of the infusion period. In addition, norepinephrine may cause blanching and sloughing of skin along injected vein (due to extreme vasoconstriction). Its nonselectivity is one of its drawbacks and the reason why it is rarely used therapeutically. Cardiovascular: Isoproterenol produces intense stimulation of the heart to increase its rate and force of contraction, causing increased cardiac output 6. It is as active as epinephrine in this action and, therefore, is useful in the treatment of atrioventricular block or cardiac arrest. Isoproterenol also dilates the arterioles of skeletal muscle (I2 effect), resulting in decreased peripheral resistance. Because of its cardiac stimulatory action, it may increase systolic blood pressure slightly, but it greatly reduces mean arterial and diastolic blood pressure (see Figure 6. Pulmonary: A profound and rapid bronchodilation is produced by the drug (I2 action, Figure 6. Isoproterenol is as active as epinephrine and rapidly alleviates an acute attack of asthma when taken by inhalation (which is the recommended route). Other effects: Other actions on Ireceptors, such as increased blood sugar and increased lipolysis, can be demonstrated but are not clinically significant. Therapeutic uses: Isoproterenol is now rarely used as a broncho-dilator in asthma. Pharmacokinetics: Isoproterenol can be absorbed systemically by the sublingual mucosa but is more reliably absorbed when given parenterally or as an inhaled aerosol. Adverse effects:the adverse effects of isoproterenol are similar to those of epinephrine. Cardiovascular: Dopamine exerts a stimulatory effect on the I1 receptors of the heart, having both inotropic and chronotropic effects (see Figure 6. Renal and visceral: Dopamine dilates renal and splanchnic arterioles by activating dopaminergic receptors, thus increasing blood flow to the kidneys and other viscera (see Figure 6. Therefore, dopamine is clinically useful in the treatment of shock, in which significant increases in sympathetic activity might compromise renal function. Therapeutic uses: Dopamine is the drug of choice for shock and is given by continuous infusion. In addition, it enhances perfusion to the kidney and splanchnic areas, as described above. An increased blood flow to the kidney enhances the glomerular filtration rate and causes sodium diuresis. In this regard, dopamine is far superior to norepinephrine, which diminishes the blood supply to the kidney and may cause renal shutdown. Adverse effects: An overdose of dopamine produces the same effects as sympathetic stimulation. Therapeutic uses: Dobutamine is used to increase cardiac output in congestive heart failure (see p. The drug increases cardiac output with little change in heart rate, and it does not significantly elevate oxygen demands of the myocardiumaa major advantage over other sympathomimetic drugs. Adverse effects: Dobutamine should be used with caution in atrial fibrillation, because the drug increases atrioventricular conduction. Oxymetazoline is absorbed in the systemic circulation regardless of the route of administration and may produce nervousness, headaches, and trouble sleeping. When administered in the nose, burning of the nasal mucosa and sneezing may occur. Phenylephrine is a vasoconstrictor that raises both systolic and diastolic blood pressures. It has no effect on the heart itself but rather induces reflex bradycardia when given parenterally. It is often used topically on the nasal mucous membranes and in ophthalmic solutions for mydriasis. Phenylephrine acts as a nasal decongestant and produces prolonged vasoconstriction. The drug is used to raise blood pressure and to terminate episodes of supraventricular tachycardia (rapid heart action arising both from the atrioventricular junction and atria). Because of its effects on the vagus nerve, methoxamine is used clinically to relieve attacks of paroxysmal supraventricular tachycardia. It is also used to overcome hypotension during surgery involving halothane anesthetics. In contrast to most other adrenergic drugs, methoxamine does not tend to trigger cardiac arrhythmias in the heart, which is sensitized by these general anesthetics. It can be used to minimize the symptoms that accompany withdrawal from opiates or benzodiazepines. Clonidine acts centrally to produce inhibition of sympathetic vasomotor centers, decreasing sympathetic outflow to the periphery. The drug is useful as a bronchodilator in the treatment of asthma and to reverse bronchospasm 6. Compared with the nonselective Iadrenergic agonists, such as metaproterenol, these drugs produce equivalent bronchodilation with less cardiac stimulation. A single dose by a metered-dose inhalation device, such as a dry powder inhaler, provides sustained bronchodilation over 12 hours, compared with less than 3 hours for albuterol. Unlike formoterol, however, salmeterol has a somewhat delayed onset of action (see Figure 6. These agents are not recommended as monotherapy and are highly efficacious when combined with a corticorsteroid.