
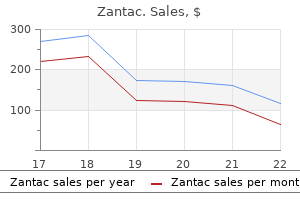
Zantac
Generic 150mg zantac visa
Department of Anaesthesia and Intensive Care Medicine gastritis aguda buy generic zantac 300mg line, Parc de Salut 2010;92:2503-13. Blood loss was measured as haemoglobin (Hb) at 24h and at discharge, visible drain blood loss (ml), calculated blood loss (ml) and transfusion. Results are shown in the table: Group 1 (n=85) Group 2 (n=91) p Basal Hb (g/dL) 14. Meta-analysis of Intravenous Tranexamic Acid in Background and Goal of Study: Maximum surgical blood ordering schedule Primary Total Hip Arthroplasty. As head and neck surgery has numerous different surgical procedures in 1 1 rich vascular supply region and bleeding risk, we wanted to recheck our institutional Kuandykov T. Blood bank was asked to check for the total liver transplantation, multiple changes in haemostasis occur. Changes in platelet preordered red packs, number of transfused packs and C/T ratio was calculated for count and function may increase blood loss. One patient has died due to multiorgan surgery failure associated with massive bleeding and hemorrhagic shock. In the last four1 years, some of our patients suffered haematoma after mastectomy, thus taking them to re-intervention. Antifbrinolytic drugs had shown their effcacy by reducing bleeding in orthopaedic surgery. Materials and Methods: Patients who underwent breast cancer surgery between 2014 and 2018 in our centre were analysed, but only mastectomies (n=139) were selected. We also reviewed if surgeon performed lymphadenectomy and prosthetic implants at the same surgical time, thinking about mechanical factors. Results and Discussion: All the patients were women with similar demographic conditions as shown on Table 1. Statistical differences between the use of tranexamic acid and incidence of haematoma were founded (Odds ratio = 0. More studies are needed in Correlation between fbrinogen and D-dimer levels order to validate other therapies such as recombinant erythropoietin or tranexamic with low-frequency piezoelectric thromboelastography acid on admission. Multivariable analysis does not prove statistical relation between delay time in surgery treatment and transfusion. Studies had proved that patients with prostate cancer have signifcantly higher D-dimer level Azumaguchi R. However, resolution by α-amylase or the possibility of ´effective´ according to the tests results. Group A (n=49) was represented by the patients with dilution was not considered at the same time. Blood coagulation constants checked by from each rat when the hematocrit was 26-30%. After statistical analysis we received strong overall by the Newman-Keuls-type test for multiple comparisons. According to our reports transfusion is related to higher mortality 30 days after surgery and during the frst year. The aim of this study is to describe the evolution of hemoglobin and perioperative transfusion needs and to identify transfusion risk factors. Material & Method: A prospective unicentric observational study including consecutive patients over the age of 65 with the diagnosis of femur fracture and indication of surgical treatment was carried out. The study was approved by the local Ethics Committee and informed consent was requested from the participants. Inherited thrombophilia: abnormal Factor V Leiden mutation and/or increased homocystein IgG/IgM. Vascular (Greece) thrombosis incidence were comparable in Inherited vs Acquired (3/23 (13. The diagnostic secondary liver neoplasm with no evidence of cirrhosis who have met who the criterion (Youden index) is >18 mm, with a sensitivity of 90. Platelet count Background: Persistent or uncontrolled bleeding is a life-threatening condition. This case report discusses a massive bleeding in order to highlight the clinical challenges associated with establishing the diagnosis and treatment approach to this coagulation factor. Red blood cells, platelets, fresh frozen plasma, fbrinogen and tranexamic acid were given. Impact patient after thromboelastometry-guided coagulation on the transfusion of blood products. Patient was rushed to the University Hospital “Virgen del Rocío” from Sevilla, Spain. The anesthetic protocol operating theatre for damage-control surgery with liver packing and drainage. Postoperative management was complicated with haemodynamic correction of conventional coagulation tests and plaquetopenia, a restrictive fuid instability, loss of liver and renal function and severe coagulopathy. The patients of group 1 had a mean age of 52 ± 10 years, unexpected and not explained. As platelets play a pivot role in haemostasis, we9 9 correlate bleeding risk with their count, ignoring that automated cell counters recognize platelets by their size. Considering the catastrophic outcome of a bleeding event vs thrombosis we decided to preclude enoxaparin and apply only mechanic measures. Platelet transfusion practices targeting general population recommendations and non-pharmacological thromboprophylaxis in an otherwise low risk patient lead to a good outcome. Results-Discussion: 901 patients were enrolled in 26 hospitals, bridging in 312 Russian bleeding assessment tools for identifying (34. The aim of study is to evaluate effectiveness of instruments that are used in diagnosing inherited and acquired bleeding disorders. Menstruation – number of days ; painful, painless; excessive, with blood clots, 4 scanty, moderate; additional characteristics: Mamaja B. Description: Test with Desmopressin is not included in the questionnaire because this drug is not Background and Goal of Study: Although numerous factors have been used in Russia as hemostatic. The Bleeding Assessment Tools is probed among demonstrated to infuence the free fap thrombosis rate, the risk factors might differ women, complaining on excessive bleeding. We compared the main thrombogenic risk factors were the following: at least 3 positive answers to questions from 1 to 7 or 2 positive between patients with and without recent trauma undergoing microvascular fap answers from questions from 1 to 7 and at least 100 scores by results of assessing surgery. Incidence of fap thrombosis was Conclusions: Thus, the study of hemorrhagic history using this Bleeding defned as primary outcome; secondary main risk factors for microvascular Assessment Tools allows the doctor to suspect disorders in the hemostasis thrombosis were evaluated. In recent trauma group prolonged surgery correlated with higher Low molecular weight heparin bridging for fap thrombosis risk (r = 0. Association with fap thrombosis 1 2 was not found for other factors such as smoking, advanced age, comorbidities, Hospital Universitari i Politècnic La Fe Valencia (Spain), Hospital 3 thrombocytosis or higher fbrinogen level. General Universitario Gregorio Marañón Madrid (Spain), Hospital Conclusions: Recent trauma was revealed to be one of the main factors Universitario Miguel Servet Zaragoza (Spain), 4Hospital Galdakao for hypercoagulability. Moreover, hypercoagulability detected by Rotational Usánsolo Bizkaia (Spain), 5Hospital Universitari i Politècnic La Fe thromboelastometry and prolonged surgery time might indicate predisposition to Valencia (Spain), 6Hospital Universitario de Gran Canaria doctor Negrín develop microvascular thrombosis, particularly in patients with recent trauma. Nevertheless, current lack of experience and unsuitable monitoring have moved to write dissimilar recommendations and to propose bridging therapy with low molecular weight heparin for high thrombotic risk patients1,2. Possible relationships between bridging therapy and the covariates were assessed by univariate analyses, using the Chi-square and Mann-Whitney U tests and by logistic regression with stepwise covariate selection adjusted for a set of covariates. A detailed perioperative strategy was designed, in a in vitro coagulation properties. The surgery, under general anesthesia, took 3 hours volunteer donors between 19 and 63 years old. Results and Discussion: End-of-storage hemolysis remained within the approved Antifbrinolytic therapy may be a useful adjuvant and must be considered. Both parameters can predict end-of-storage hemolysis at earlier time points of storage. We aimed to evaluate the role of the standard coagulation profle and necessitating an urgent appendectomy. Materials and Methods: We collected data from 105 patients undergone free Patient was on warfarin after prosthetic aortic valve implantation. Surgery was uneventful and patient returned to surgical ward Results and Discussion: We found correlation between fap thrombosis and in stable condition. However, it is known that metronidazole and ciprofoxacine both can cause prolongation of warfarin effect.
Purchase zantac 300mg otc
As the agonists relax and their pulling force diminishes autoimmune gastritis definition buy genuine zantac, it will become easier to per form strengthening exercises on the opposing antagonist muscles. Ask your treating physician to specify which of your muscles are acting as agonists. In general, these are the ones that are being injected with botulinum toxin, and you should practice those stretching exercises specific for them. Also ask your physician which antagonist muscles he would recommend for strengthening. In most cases, these will be the mus cles that correspond to the agonists on the opposite side of your neck, but additional antagonists may need strengthening as well. If you have a physical therapist, he may be able to help in selecting the particular muscles and exercises that are appropriate for you. With a few modifications, they can be performed in almost any setting, at home or at work. All of the exercises described are to be performed slowly—you should perform all of them in slow motion. If any movement produces pain, you should stop and seek further advice from your doctor. Many of the following stretching exercises can be done in the standing or seated position. In the standing posi tion, the height of the handhold should be about the mid-thigh level, close to where the hand rests naturally. In the seated position, a sturdy chair with a suitable leg or cross bar should suffice. For some exer cises requiring a handhold in front of you, the front edge of the seat may be grasped. The illustrations depict a common type of inexpensive metal folding chair available at most office or home warehouse stores. It may be useful for individuals who have a component of rotational torticollis plus retrocollis (as in Figure 21). It is per formed in a seated position on a chair that allows you to grasp and hold underneath (Figure 24). Alternatively, it can be performed in the standing position next to an object that has a handhold at approximately the mid-thigh level. The entire procedure may be reversed if you require stretching of the right-sided muscles. Slowly lean your body forward and toward the right side, and at the same time allow your left shoulder to relax and be pulled downward while keeping your grip on the handhold. Next, turn your head about 45 degrees toward the right, then tilt your head into a direction away Figure 24 80 / the Spasmodic Torticollis Handbook from your left arm. As you do this, feel the stretch in the muscles of your shoulder and the back of your neck on the left side. To make the stretch even more effective, reach over the top of your head with your right hand and gently help pull along the direction of the stretch (Figure 25). Figure 25 81 / Rehabilitation Exercises Exercise two: Sternocleidomastoid on one side this next exercise is intended to provide stretch to one of the major muscles that runs diagonally across the front and side of the neck and has attachments at the collar bone and the back of the skull. The movements in this particular exercise are somewhat complex, and will require some patience and practice to be performed correctly. If you relax your shoulder, you will find that your collarbone is pulled downward. Once your Figure 26 82 / the Spasmodic Torticollis Handbook head has been rotated as far as it can comfortably go, begin tilting your head backward so that your chin moves toward the ceiling. Now tilt your head slightly so that your right ear moves closer to your right shoulder (Figure 27). As you do this, you may feel a stretching sensation from your left collarbone to the side of neck. At this point, you may increase the stretch a little further by cupping the fingers of your left hand around your chin and slowly and gently pushing upwards. This is best done in a seated position in a chair with some support for the back (Figure 28). Now, slowly tilt your head backward so that your chin moves toward the ceiling (Figure 29). Figure 28 84 / the Spasmodic Torticollis Handbook Figure 29 85 / Rehabilitation Exercises Exercise four: Trapezius, levator scapuli, sternocleidomastoid, and scalenes the next exercise is intended to provide stretch for the muscles that lift the shoulder upwards and tilt the head directly sideways, mainly the trapezius and levator scapuli, but also the scalenes and stern ocleidomastoid. Starting from the seated or standing position, grasp a handhold beside you with your left hand (Figure 30). Lean your body to the right while relaxing your shoulder muscles and allowing your shoul der to be pulled downward. At this point, you can increase the stretch a little further by placing your right hand over the top of your head and slowly and gently pulling to the right (Figure 31). This mus cle starts at the neck bones and runs diagonally upward and outward to the base of the skull. First rotate your head toward the left, then tilt your head downward, tucking your chin toward your chest (Figure 32). You may begin feel ing a stretching sensation in the back of your neck, on one or both sides. At this point, you may increase the stretch a little further by placing your fingers against the side of your chin and gently pushing to rotate your chin toward your left shoul der (Figure 33). Strengthening these muscles can help to bring your head back to the neutral position. To strengthen any muscle, it is neces sary to use it to exert a force against resistance. Thus, to perform these exercises, you will need a suitable object against which to push. A pillow-sized block of soft foam rubber works best and may be obtained from a medical supply store or pharmacy. Most of the following exercises can be modified for performance in the sitting, standing, or lying position. In most cases, resistance supplied by an opposing hand or fingers can be substituted for the foam block or pillow, allowing the exercises to be performed in almost any situation. If you are not able to perform an exercise against resistance, try the movement by itself at first, using no type of resistance. Overactivity of the right sternocleidomastoid produces rotational torticollis toward the left (Figure 34), in which case strengthening of the left sternocleidomastoid is required. Place the foam block on top of your right shoulder flush with the wall (Figure 35). Rotate your head until you are pressing as hard as you comfortably can (Figure 36). Some people may only be able to perform this exercise without a pillow; resistance pro vided by placing a hand on the side of the face may suffice. Figure 34 91 / Rehabilitation Exercises Figure 35 Figure 36 92 / the Spasmodic Torticollis Handbook Exercise seven: Trapezius and levator scapuli the next exercise is intended to strengthen the muscles that elevate the shoulder and shoulder blade, mainly the trapezius and the leva tor scapuli. The entire procedure may be reversed if you require strengthening of the right-sided muscles. Try to keep your arm straight and do not try to lift by bending your arm at the elbow. Pull with your shoulder muscles as hard as you comfortably can, hold for 30 seconds, then slowly release and relax. Figure 37 93 / Rehabilitation Exercises Exercise eight: Splenius capitis and others on one side this exercise is designed to strengthen the muscles that lie along the back of the neck on either side of the neck bones. Try to push against the block with the part of your head immediately behind and above your right ear. Push as hard as you comfortably can, hold for 10 seconds, then slowly release and relax. Now lift your head straight upwards, tilting your chin slightly toward your chest. If desired, push against your forehead with two fingers as shown to provide resistance (Figure 41). Figure 40 96 / the Spasmodic Torticollis Handbook Figure 41 97 / Rehabilitation Exercises Exercise ten: Sternocleidomastoid, trapezius, levator scapuli, and scalenes this exercise is designed to strengthen the muscles that tilt the head sideways and elevate the shoulder, including the sternocleidomas toid, trapezius, and levator scapuli. The individual shown in Figure 10 has lateralcollis produced by overactivity of left-sided muscles, and requires strengthening on the right.
Discount 150 mg zantac otc
The nodules in the conjunctiva should be excised; Treatment: If the disease is a primary focus gastritis nsaids buy zantac 150mg low price, it should otherwise the condition is treated on general principles. In all cases systemic antitubercular Conjunctival involvement in leprosy is not uncommon. Later, the lids become softer and are more easily develop independently or in conjunction with facial nerve everted, making the conjunctiva puckered and velvety, and paralysis and lagophthalmos with exposure keratopathy. In some Fungal Conjunctivitis cases a false membrane forms, so that the case resembles a Fungal infections due to Aspergillus, Candida albicans, membranous conjunctivitis. Nocardia, Leptothrix and Sporothrix can infrequently pres Note: As the gonococcus has the power of invading in ent as chronic conjunctivitis. Follicular conjunctivitis with tact epithelium, there is a risk of corneal ulceration in un lymphadenopathy is one mode of presentation. Ulceration usually Treatment is with topical miconazole or clotrimazole occurs over an oval area just below the centre of the cornea, 1%. Rhinosporidiosis is a specifc type of mycotic conjunc corresponding to the position of the lid margins when the tivitis caused by Rhinosporidium seeberi, described from eyes are closed and consequently rotated somewhat up certain geographic regions such as Sri Lanka, Southern In wards. Rarely, oval marginal ulcers are formed as in the dia, Central and South America, and Africa. The ulcers tend to ex dunculated feshy exophytic granulomatous growths, whose tend rapidly, both superfcially and in depth, resulting in surface is irregular and covered with minute white dots, are perforation, usually manifesting clinically as a black spot or characteristic. The lesions are treated by complete surgical area in the ulcer caused by a prolapse of the iris. Also known as Neonatal conjunctivitis and is defned as a Complications: Inadequate treatment may result in mucoid, mucopurulent, or purulent discharge from one or serious sequelae. Any discharge, even a perforation there is always much scarring of this tissue, but watery secretion, from a baby’s eyes during the frst week the nebula clears more in babies than in older people. Per should be viewed with suspicion, since tears are not secreted foration may be followed by anterior synechiae, adherent so early in life. Besides ophthalmia neonatorum, the differen leucoma, partial or total anterior staphyloma, anterior cap tial diagnosis of a child with discharge from the eyes within sular cataract or panophthalmitis. When vision is not com the frst month of life includes a congenitally blocked nasolac pletely destroyed but seriously impaired by the corneal rimal duct, acute dacryocystitis, and congenital glaucoma. Chlamydia Trachomatis Chlamydia trachomatis inclusion conjunctivitis manifests relatively late, usually over 1 week Causative Agents after birth. This is a relatively common cause of ophthalmia Neisseria Gonorrhoeae Neisseria gonorrhoeae manifests neonatorum. Bacterial examination is negative or inconse earliest, typically within the first 48 hours of birth. Both is a venereal infection derived from the cervix or urethra of eyes are nearly always affected, with one usually worse the mother. The conjunctiva becomes intensely infamed, the infammation is less severe than in the gonococcal bright red and swollen, with a thick yellow pus discharge. To examine the baby’s eyes, sence of a subconjunctival adenoid layer in children, there are retractors might be needed to separate the swollen lids and no follicles that appear, in contrast to infection in the adult. There is dense in occasionally, in prolonged cases, the corneal periphery fltration of the bulbar conjunctiva, and the lids are swollen may be invaded by a pannus. Gram-negative intracellular diplococci with poly Other Bacteria Other bacteria such as staphylococci, morphonuclear leucocytes indicate N. Gram-stained smears showing 48–72 hours after birth and herpes simplex virus infection polymorphonuclear leucocytes and lymphocytes with presents 5–7 days after birth. Chemical Toxicity Gram-stained conjunctival smears with many bacteria Chemical toxicity used to be seen within a few hours of and polymorphonuclear leucocytes are indicative of a prophylactic topical treatment with silver nitrate solution in bacterial infection such as Staphylococcus aureus, Strep some cases, and disappeared spontaneously in 24–36 hours. In the past, if maternal infection was suspected a drop of l Conjunctival scrapings obtained for the chlamydial silver nitrate solution 1% was instilled into each eye immunofluorescent antibody test and specimens sent for (Crede’s method). It is rarely seen nowadays as erythromy viral, chlamydial and bacterial culture and sensitivity. Investigations l Staining: Where diagnostic tests are not available, the Treatment gram-stained smear is a useful and sensitive test with a As the disease is preventable, prophylactic treatment is of high positive predictive value for identifying the aetio prime importance. Sometimes the allergen is a bacterial protein of results of the Gram and Giemsa stains. The treatment should endogenous nature, the most common being a staphylococ be guided by the identified oraganisms. A the choice of antibiotic and mode of therapy for differ more characteristic picture is due to exogenous proteins, in ent organisms commonly causing ophthalmia neonatorum which the conjunctivitis may form part of a typical hay fe are summarized in Table 14. Contact with animals (horses, cats), pollens or with a single intramuscular injection of either ceftriaxone certain fowers (primula, etc. The Chlamydial ophthalmia is treated with a suspension of most typical picture of such an acute reaction is that of atro erythromycin ethylsuccinate 50 mg/kg daily in four divided pine or brimonidine allergy, while other drugs tend to produce doses before feeds for 2–3 weeks, or azithromycin 10 mg/kg a more chronic response characterized by follicle formation. Local treatment is with chlortetracycline 1% Symptoms: Itching is a prominent symptom, redness, or erythromycin eye ointment after feeds. In all cases watery secretion which is not purulent and a whitish ropy both parents must receive appropriate treatment for genital discharge are characteristic. Once the sensitivity test Signs: Redness, lacrimation, papillary hyperplasia of is available, the antibiotic may be changed if required. However, velop a muddy discoloration of the conjunctiva, dry eye, conjunctivitis due to Chlamydia trachomatis persists as it secondary changes in cornea such as vascularization and is not affected by neomycin. If herpes simplex viral infection is present vidarabine Treatment: 3% or acyclovir 3% eye ointment is used fve times a day l Elimination of allergen: Logically, treatment is removal for a week and then three times a day till resolution. Sys of the allergen from the environment; if this cannot be temic acyclovir is recommended for systemic involvement done, desensitization may be attempted by a long course after paediatric consultation. If chemical toxicity is suspected no treatment is l Temporary relief may be obtained by decongestant eye needed as it is self-resolving. All affected babies must be drops (naphazoline), antihistamine drugs (antazoline re-evaluated daily for the frst 48–72 hours and repeat azelastine, chlorpheniramine). Non-infectious Conjunctivitis A short course of corticosteroid drops frequently brings Allergic Conjunctivitis relief in severe cases, which do not respond to the topical the allergic reactions of the conjunctiva may assume use of 2% sodium cromoglycate drops. Both types are hot weather, and therefore rather a summer than a spring complicated by a fne diffuse superfcial punctate keratitis. The complaint, found in young children and adolescents, usu ultimate prognosis is generally good with the disease being ally boys. Corneal involvement can take the form of punc usually self-limited over a period of a few years. Children usually for several years with the development of severe dry eyes and have a self-limited disease and eventually ‘grow out’ of the corneal ulcers (shield ulcer), with scarring. Symptoms: Burning, itching, some photophobia and l Topical therapy: Eye drops containing anti-histaminics, lacrimation are the chief symptoms. On everting the and topical cyclosporine are useful to control the allergic upper lid the palpebral conjunctiva is seen to be hypertro reaction and consequent inflammation. Acetyl cysteine phied and mapped out into polygonal raised areas, not unlike used as 10 or 20% drops 3–4 times a day for 1–2 weeks is cobblestones (Fig. Medications are pre milk, and this appearance may also be seen over the lower scribed in a step ladder approach using minimum medi palpebral conjunctiva. The fat-topped nodules are hard, and cations to start with and adding more depending on the consist chiefy of dense fbrous tissue, but the epithelium response. Treatment is titrated to the response and tapered over them is thickened, giving rise to the milky hue. Eosinophilic leucocytes are present in them in great l Local therapy: Subtarsal injections of long acting ste numbers and found in the secretion. In addition, infltration roids such as triamcinolone may be required for severe with lymphocytes, plasma cells, macrophages, basophils refractory cases. The l Surgical treatment: Surgical excision of giant papillae type of patient, the milky hue, freedom of the fornix from may be required. Shield ulcers can be treated with debride implication and the characteristic recurrence in hot weather ment of the surface and application of amniotic membrane will usually prevent misdiagnosis. The limbal or bulbar form is recognized by an opacif l Systemic therapy: Oral anti-allergic medications can cation of the limbus (Fig.
Buy zantac 300 mg with amex
Most patients will tolerate this regimen well chronic gastritis medscape buy zantac from india, but should be under surveillance for breakthrough disease (especially after drug cessation) or adverse drug effects (principally anemia). Special caution must be exercised in handling hypodermic needles and other sharps which could result in parenteral exposure. In several instances, secondary infections among contacts and medical personnel without direct body fluid exposure have been well documented. The patient should be hospitalized in a private room with an adjoining anteroom to be used for putting on and removing protective barriers, storage of supplies, and decontamination of laboratory specimen containers. In the absence of a large, fixed medical treatment facility, or in the event of an overwhelming number of casualties, isolation rooms may not be available for all casualties. Personnel should wear contact and respiratory protection while in this patient care area. Personnel should undergo an external decontamination procedure at the point of leaving the patient care area. A building, room or designated area that is separated from the patient care area should be established for donning and removing protective gear. All waste (including linens) leaving the patient care area should be decontaminated with bleach or quaternary ammonium compounds and double bagged in clearly labeled biohazard waste bags. Laboratory specimens should be double-bagged, and the exterior of the outer bag should be decontaminated before transport to the laboratory. Excreta and other contaminated materials should be autoclaved, or decontaminated by the liberal application of appropriate disinfectants. Clinical laboratory personnel are at significant risk for exposure and should employ a biosafety cabinet (if available) with barrier and respiratory precautions when handling specimens. Access to this space should be limited and thorough decontamination of the space and equipment should be routine. Should the patient die, there should be minimal handling of the remains, which should ideally be sealed in leak-proof material for prompt burial or cremation. Toxins are not man-made, are non-volatile (no vapor hazard), are usually not dermally active (mycotoxins are the exception), and may be much more toxic (based on weight) than chemical agents. A toxin’s lack of volatility is a very important property and makes them unlikely to produce either secondary or person-to-person exposures, or a persistent environmental hazard. The bacterial toxins, such as botulinum toxins, are the most toxic substances by weight known (Appendix I). Less toxic compounds, such as the mycotoxins, are thousands of times less toxic than botulinum, and have limited aerosol potential. The relationship between aerosol toxicity and the quantity of toxin required for an effective open-air exposure is shown in Appendix J, which demonstrates that for some agents such as the mycotoxins and ricin, very large (ton) quantities would be needed for an effective open-air attack in a dispersed tactical environment. For example, botulinum and tetanus toxins are large molecular-weight proteins, and are easily denatured by environmental factors (heat, dessication, or ultraviolet light), thus posing little downwind threat. As with all biological weapons, potential to cause incapacitation as well as lethality must be considered. Depending on the goals of an adversary, incapacitating agents may be more effective than lethal agents. Large numbers of ill patients might overwhelm the medical and evacuation infrastructure and will almost certainly create panic and disruption of the affected population. These findings are followed by symmetrical descending flaccid paralysis, with generalized weakness and progression to respiratory failure. Symptoms begin as early as 12-36 hours after inhalation, but may take several days to develop after exposure to low doses of toxin. Biological agent attack should be suspected if multiple casualties simultaneously present with progressive descending flaccid paralysis. Laboratory confirmation can be obtained by bioassay (mouse neutralization) of the patient’s serum. Because the original toxoid components were produced in 1970, recent evidence suggests that immunologic protection for serotypes B through E may not be adequately obtained with this currently available pentavalent toxoid vaccine. Botulinum toxin is not dermally active and secondary aerosols are not a hazard from patients. These toxins, types A through G, are the most potent neurotoxins known; paradoxically, they have been used therapeutically to treat spastic conditions (strabismus, blepharospasm, torticollis, tetanus) and cosmetically to treat wrinkles. The spores are ubiquitous; they germinate into vegetative bacteria that produce toxins during anaerobic incubation. There are three epidemiologic forms of naturally occurring botulism foodborne, infantile, and wound. Botulinum toxin can be delivered by aerosol or used to contaminate food or water supplies. When inhaled, these toxins produce a clinical picture very similar to foodborne intoxication, although the time to onset of paralytic symptoms after inhalation may actually be longer than for foodborne cases, and may vary by type and dose of toxin. It is feasible to deliver botulinum toxins as an aerosolized biological weapon, and several countries and terrorist groups have weaponized them. The Aum Shinrikyo cult in Japan weaponized and attempted to disseminate botulinum toxin on multiple occasions in Tokyo before their 1995 sarin attack in the Tokyo subway. Botulinum toxins are proteins with molecular masses of approximately 150,000 daltons. Each of the seven distinct, but related neurotoxins, A through G, is produced by a different strain of Clostridium botulinum. All seven types act by similar mechanisms of inhibition of presynaptic acetylcholine release. Although intelligence suggests attack by aerosol dispersal is the most likely scenario for the use of botulinum toxins, the agent could be used to sabotage food supplies. The toxin is taken into the axon, where the A chain exerts its cytotoxic effect; it inactivates the axon, preventing release of acetylcholine and blocking neuromuscular transmission (pre-synaptic inhibition). This interruption of neurotransmission causes cranial nerve and skeletal muscle paralysis seen in clinical botulism. Unlike the situation with nerve agent intoxication, where there is too much acetylcholine due to inhibition of acetylcholinesterase, the problem in botulism is lack of the neurotransmitter in the synapse. Thus, pharmacologic measures such as atropine are not indicated in botulism and could exacerbate symptoms (see Appendix H). Cranial nerve palsies are prominent early, with eye symptoms such as blurred vision due to mydriasis, diplopia, ptosis, and photophobia, in addition to other cranial nerve signs such as dysarthria, dysphonia, and dysphagia. Flaccid skeletal muscle paralysis follows, in a symmetrical, descending, and progressive manner. Collapse and obstruction of the upper airway may occur due to weakness of the oropharyngeal musculature. As the descending motor weakness involves the diaphragm and accessory muscles of respiration, respiratory failure may occur abruptly. Progression from onset of symptoms to respiratory failure has occurred in as little as 24 hours in cases of severe foodborne botulism. However, the psychological sequelae of botulism may be severe and require specific intervention. Physical examination usually reveals an afebrile, alert, and oriented patient, although the paralysis may limit the patient’s ability to respond. Mucous membranes may be dry and crusted and the patient may complain of dry mouth or sore throat. Individual cases might be confused clinically with other neuromuscular disorders such as Guillain-Barre syndrome, myasthenia gravis, or tick paralysis. The edrophonium or Tensilon test may be transiently positive in botulism, so it may not distinguish botulinum intoxication from myasthenia. The cerebrospinal fluid in botulism is normal and the paralysis is generally symmetrical, which distinguishes it from enteroviral myelitis. It may become necessary to distinguish nerve agent and/or atropine poisoning from botulinum intoxication. Nerve agent poisoning produces copious respiratory secretions, miotic pupils, convulsions, and muscle twitching, whereas normal secretions, mydriasis, difficulty swallowing, and progressive muscle paralysis is more likely in botulinum intoxication. The clinical differences between botulinum intoxication and nerve agent poisoning are depicted in Appendix H.
Purchase zantac 300 mg
Reaction to accommodation is preserved (partial iri doplegia) gastritis emedicine zantac 300mg low price, hence this is one of the causes of light-near pupillary dissociation. Holmes–Adie pupil may be associated with other neurological features (Holmes–Adie syndrome). These include loss of lower limb tendon reflexes (espe cially ankle jerks); impaired corneal sensation; chronic cough; and localized -179 H Holmes’ Tremor or generalized anhidrosis, sometimes with hyperhidrosis (Ross’s syndrome). Pathophysiologically Holmes–Adie pupil results from a peripheral lesion of the parasympathetic autonomic nervous system and shows denervation super sensitivity, constricting with application of dilute (0. Cross References Anhidrosis; Anisocoria; Hyperhidrosis; Light-near pupillary dissociation; Pseudo-Argyll Robertson pupil Holmes’ Tremor Holmes’ tremor, also known as rubral tremor, or midbrain tremor, has been defined as a rest and intention tremor, of frequency <4. The rest tremor may resemble parkinsonian tremor and is exacerbated by sustained postures and voluntary movements. Once attributed to lesions of the red nucleus (hence ‘rubral’), the anatomical substrate is now thought to be interruption of fibres of the supe rior cerebellar peduncle (hence ‘midbrain’) carrying cerebellothalamic and/or cerebello-olivary projections; lesions of the ipsilateral cerebellar dentate nucleus may produce a similar clinical picture. If a causative lesion is defined, there is typically a delay before tremor appearance (4 weeks to 2 years). Cross Reference Tremor Hoover’s Sign Hoover’s sign may be used to help differentiate organic from functional hemi plegia or monoplegia. It is based on the fact that when a recumbent patient attempts to lift one leg, downward pressure is felt under the heel of the other leg, hip extension being a normal synergistic or synkinetic movement. The finding of this synkinetic movement, detected when the heel of the supposedly para lyzed leg presses down on the examiner’s palm, constitutes Hoover’s sign: no increase in pressure is felt beneath the heel of a paralyzed leg in an organic hemiplegia. Cross References ‘Arm drop’; Babinski’s trunk–thigh test; Functional weakness and sensory disturbance; Synkinesia, Synkinesis Horner’s Syndrome Horner’s syndrome, or Bernard–Horner syndrome, is defined by a constellation of clinical findings, most usually occurring unilaterally, viz. The first two mentioned signs are usually the most evident and bring the patient to medical attention; the latter two are usually less evident or absent. The sympathetic innervation of the eye consists of a long, three neurone, pathway, extending from the diencephalon down to the cervicothoracic spinal cord, then back up to the eye via the superior cervical ganglion and the inter nal carotid artery, and the ophthalmic division of the trigeminal (V) nerve. A wide variety of pathological processes, spread across a large area, may cause a Horner’s syndrome, although many examples remain idiopathic despite inten sive investigation. Determining whether the lesion causing a Horner’s syndrome is pregan glionic or postganglionic may be done by applying to the eye 1% hydroxyam phetamine hydrobromide, which releases noradrenaline into the synaptic cleft, which dilates the pupil if Horner’s syndrome results from a preganglionic lesion. Arm symptoms and signs in a smoker mandate a chest radiograph for Pancoast tumour. If the Horner’s syndrome is isolated and painless, then no investiga tion may be required. Unilateral miosis may be mistaken for contralateral mydriasis if ptosis is sub tle, leading to suspicion of a partial oculomotor nerve palsy on the ‘mydriatic’ side. Observation of anisocoria in the dark will help here, since increased anisoco ria indicates a sympathetic defect (normal pupil dilates) whereas less anisocoria suggests a parasympathetic lesion. Applying to the eye 10% cocaine solution will also diagnose a Horner’s syndrome if the pupil fails to dilate after 45 min in the dark (normal pupil dilates). Ageusia may also be present if the chorda tympani branch of the facial nerve is involved. Reduction or absence of the stapedius reflex may be tested using the stetho scope loudness imbalance test: with a stethoscope placed in the patients ears, a vibrating tuning fork is placed on the bell. Normally the perception of sound is symmetrical, but sound lateralizes to the side of facial paresis if the attenuating effect of the stapedius reflex is lost. Cross References Ageusia; Bell’s palsy; Facial paresis, Facial weakness Hyperaesthesia Hyperaesthesia is increased sensitivity to sensory stimulation of any modality. Cross References Anaesthesia; Hyperalgesia Hyperalgesia Hyperalgesia is the exaggerated perception of pain from a stimulus which is normally painful (cf. This may result from sensitization of nocicep tors (paradoxically this may sometimes be induced by morphine) or abnormal ephaptic cross-excitation between primary afferent fibres. Cross References Allodynia; Dysaesthesia; Hyperpathia Hyperekplexia Hyperekplexia (literally, to jump excessively) is an involuntary movement disor der in which there is a pathologically exaggerated startle response, usually to sudden unexpected auditory stimuli, but sometimes also to tactile (especially trigeminal) and visual stimuli. The startle response is a sudden shock-like move ment which consists of eye blink, grimace, abduction of the arms, and flexion of the neck, trunk, elbows, hips, and knees. Ideally for hyperekplexia to be diagnosed there should be a physiological demonstration of exaggerated startle response, but this criterion is seldom adequately fulfilled. Familial cases have been associated with mutations in the α1 subunit of the inhibitory glycine receptor gene. Cross References Incontinence; Myoclonus Hypergraphia Hypergraphia is a form of increased writing activity. It has been suggested that it should refer specifically to all transient increased writing activity with a non-iterative appearance at the syntactic or lexicographemic level (cf. Hypergraphia may be seen as part of the interictal psychosis which some times develops in patients with complex partial seizures from a temporal lobe (especially non-dominant hemisphere) focus, or with other non-dominant tem poral lobe lesions (vascular, neoplastic, demyelinative, neurodegenerative), or psychiatric disorders (schizophrenia). Hypergraphia is a feature of Geschwind’s syndrome, along with hyperreligiosity and hyposexuality. Cross References Automatic writing behaviour; Hyperreligiosity; Hyposexuality Hyperhidrosis Hyperhidrosis is excessive (unphysiological) sweating. Localized hyperhidrosis caused by food (gustatory sweating) may result from aberrant connections between nerve fibres supplying sweat glands and salivary glands. Other causes of hyperhidro sis include mercury poisoning, phaeochromocytoma, and tetanus. Transient hyperhidrosis contralateral to a large cerebral infarct in the absence of auto nomic dysfunction has also been described. Symptoms may be helped (but not abolished) by low dose anticholinergic drugs, clonidine, or propantheline. Cross References Ballism, Ballismus; Chorea, Choreoathetosis; Dysarthria Hyperlexia Hyperlexia has been used to refer to the ability to read easily and fluently. Patients with hypermetamorphosis may explore compulsively and touch everything in their environment. This is one element of the environmental dependency syndrome and may be associated with other forms of utilization behaviour, imitation behaviour (echolalia, echopraxia), and frontal release signs such as the grasp reflex. It occurs with severe frontal lobe damage and may be observed following recovery from herpes simplex encephalitis and in frontal lobe dementias includ ing Pick’s disease. Bitemporal lobectomy may also result in hypermetamorphosis, as a feature of the Klüver–Bucy syndrome. Cross References Geophagia, Geophagy; Klüver–Bucy syndrome Hyperpathia Hyperpathia is an unpleasant sensation, often a burning pain, associated with elevated threshold for cutaneous sensory stimuli such as light touch or hot and cold stimuli, especially repetitive stimuli. Clinical features of hyperpathia may include summation (pain perception -185 H Hyperphagia increases with repeated stimulation) and aftersensations (pain continues after stimulation has ceased). The term thus overlaps to some extent with hyperal gesia (although the initial stimulus need not be painful itself) and dysaesthesia. There is an accompanying diminution of sensibility due to raising of the sensory threshold (cf. Hyperpathia is a feature of thalamic lesions, and hence tends to involve the whole of one side of the body following a unilateral lesion such as a cerebral haemorrhage or thrombosis. Generalized hyperpathia may also be seen in variant Creutzfeldt–Jakob disease, in which posterior thalamic (pulvinar) lesions are said to be a characteristic neuroradiological finding. Cross References Allodynia; Dysaesthesia; Hyperalgesia Hyperphagia Hyperphagia is increased or excessive eating. Binge eating, particularly of sweet things, is one of the neurobehavioural disturbances seen in certain of the frontotemporal dementias. Hyperphagia may be one feature of a more gen eral tendency to put things in the mouth (hyperorality), for example, in the Klüver–Bucy syndrome. Cross References Hyperorality; Klüver–Bucy syndrome Hyperphoria Hyperphoria is a variety of heterophoria in which there is a latent upward devi ation of the visual axis of one eye. Using the cover–uncover test, this may be observed clinically as the downward movement of the eye as it is uncovered. Cross References Cover tests; Heterophoria; Hypophoria Hyperpilaphesie the name given to the augmentation of tactile faculties in response to other sensory deprivation, for example, touch sensation in the blind. This may be physiological in an anxious patient (reflexes often denoted ++), or pathological in the context of corticospinal pathway pathology (upper motor neurone syn drome, often denoted +++). It is sometimes difficult to distinguish normally brisk reflexes from pathologically brisk reflexes. Hyperreflexia (including a jaw jerk) in isolation cannot be used to diagnose an upper motor neurone syndrome, and asymmetry of reflexes is a soft sign.
Discount 300mg zantac with amex
When appropriate gastritis green stool buy zantac online from canada, counsel older adults and their caregivers on potential driving cessation, and/or alternative transportation options as needed (see Chapter 6). Older driver abilities are not static and may either improve or decline as their conditions change. For example, an older adult may benefit from physical therapy after a stroke or surgery and regain functional abilities permitting them to return to driving. In addition, specialists in the fields of cardiology, ophthalmology, neurology, psychiatry, psychology, rehabilitation, orthopedics, emergency/urgent care, trauma, and others all encounter older adults with conditions that may have an impact on driving skills. When advising older adults, clinical team members may wish to consult the reference list of medical conditions in Chapter 9. Driving and dementia of the alzheimer type: beliefs and cessation strategies among stakeholders. Life expectancy at birth, at age 65, and at age 75, by sex, race, and Hispanic origin: United States, selected years 1900 2010. Office of Statistics and Programming, National Center for Injury Prevention and Control. High mortality in elderly drivers is associated with distinct injury patterns: Analysis of 187,869 drivers. Fragility versus excessive crash involvement as determinants of high death rates per vehicle mile of travel for older drivers. The perception of meaningfulness and performance of instrumental activities of daily living from the perspectives of the medically at-risk older adults and their caregivers. Journal of Gerontology, Series A: Biological Sciences and Medical Sciences, 60, 399–403. Understanding older drivers: An examination of medical conditions, medication use, and travel behavior. Self-regulatory driving practices among older adults: health, age and sex effects. Epidemiology of older driver crashes-identifying older driver risk factors and exposure patters. Older adult opinions about driving cessation: a role for advanced driving directives. Biopsychosocial risk factors for driving cessation: findings from the health and retirement study. Motor-vehicle crash history and licensing outcomes for older drivers reported as medically impaired in Missouri. Not At Risk: Minimal to No Positive Risk Factors Identified Older adult/caregiver concerns? When taking the patient’s history and reviewing the medical record, be alert to “red flags,” which include any medical conditions, visual, cognitive, or motor changes, medications, functional decline, or symptoms or signs that can affect driving skills and safety. The media often emphasizes age when an older driver is involved in an injurious crash, but this is ageism and not evidenced-based. Phillips, an 82-year-old man with a history of hypertension, congestive heart failure, atrial fibrillation, type 2 diabetes mellitus, macular degeneration, and osteoarthritis, comes to your office for a routine check-up. Phillips ambulates with a wide-based ataxic gait, uses a walker, and has impaired standing balance. He is unable to stand from the exam chair without multiple attempts and use of his arms, and he reports feeling temporarily lightheaded on standing. He is no longer able to read newspaper print and tells you he avoids driving at night and only goes short distances to run errands, get to appointments, and meet weekly with his bridge club. Bales, a 90-year-old woman, lives in a continuing care retirement community with her 92-year-old husband for whom she is the primary caregiver because of his Parkinson’s disease. She has decreased range of motion in her neck and walks without an assistive device but with a wide-based gait. She drinks a moderate amount of alcohol daily and was recently started on oxycodone for chronic pain. The goal of the assessment is to facilitate driving safety among older adults and assure that those who can drive safely are helped to do so. Sensory deprivation such as impaired vision, hearing or decreased sensation in the extremities. Phillips has difficulty with balance and strength as revealed by his inability to get up from the chair without multiple tries and his wide-based gait. This raises a question as to whether he can operate vehicle foot pedals properly or see well enough to both drive and find his way safely. His physical limitations may not preclude driving, but they may be indicators that more assessment is indicated. Be alert to conditions in the older adult’s medical history, examine the current list of medications, and perform a comprehensive review of systems. During an interview of the older driver, clinicians should be alert to “red flags,” i. Phillips (introduced in previous chapter) presents with lightheadedness associated with atrial fibrillation. Phillips should be counseled to cease driving until his symptoms are diagnosed, treated and resolved. Significant pain and associated limitations in function seen with degenerative joint disease, such as those noted with Mrs. Acute or chronic pain can also be distracting and make it unsafe for older adults to drive. Many factors can put individuals at risk of unsafe driving and should be explored during office visits (Table 2. Not noticing workmen or activity on side of the road Inappropriate speeds for the weather/driving conditions History of traffic violations, minor crashes, or warnings Most older adults have at least one chronic medical condition and many have multiple conditions, the most common including arthritis, hypertension, hearing impairments, heart 1 disease, cataracts, dizziness, orthopedic impairments, and diabetes. Some of these conditions have been associated with driving impairment by virtue of both their symptoms and their treatments. These conditions will be discussed in more detail in subsequent chapters, including a reference list of medical conditions and medications that may affect driving in Chapter 9, with some of the more common chronic conditions noted below in Table 2. Older adults generally take more medications than their younger counterparts and are more susceptible to adverse effects. The Beers Criteria for potentially inappropriate medication use in 2 older adults is a useful tool for screening medication lists. Whenever medication is prescribed or the dosage of a current medication is changed, it is important to inform the older adult of potential effects or drug-drug interactions that might affect driving safety. Adverse effects, such as drowsiness, confusion, dizziness, or nausea, can impact the ability to concentrate and drive safely. Concern may be heightened in the face of already-present underlying concerns about visuospatial processing speed, cognition, or functional changes. For example, loss of consciousness, confusion, falling asleep while driving, feelings of faintness, memory loss, visual impairment, numbness or tingling in extremities, and muscle weakness all have the potential to affect driving safety. The clinical team should not make assumptions about whether an older adult is driving and should always be sure to ask about this important activity of daily living. If the older adult or his or her caregiver asks your opinion about whether the individual is safe to drive, any concerns that have been noted should be explored. Has the older adult had any recent accidents, near-accidents, citations or crashes? A list of specific driving behaviors that could indicate concerns for safety are found in the Fitness to Drive 3 measure freely available online. Clinicians should encourage caregivers to monitor and observe skills of the older adult driver in real-world traffic situations, with full disclosure and permission from the older driver. Concern should be noted if caregivers will not drive with the individual or let others drive with him or her. If the older adult is living in a retirement community (or continuing care retirement community, assisted living, etc. Unfortunately, the media often emphasizes age when an older driver is involved in an injurious crash. Although many people experience a decline in vision, cognition, or motor skills as they get older, these changes occur at different rates, and older adults experience functional changes to different degrees. The focus should be on functional abilities and medical fitness to drive versus on age per se. The clinical team should take the approach of optimizing safe 5 driving rather than simply stopping the individual from driving. A health risk assessment is a series of questions intended to identify potential health and safety hazards in the older adult’s behaviors, lifestyle, and living environment (Table 2. The health risk assessment is tailored to the older adult and generally focuses on physical activity, falls, drinking (alcohol), medication management, and driving.
Generic zantac 300mg on line
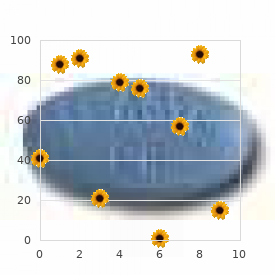
The demographic groups represented in this study correlate to the population that is affected by diabetic foot ulcers chronic gastritis meal plan discount zantac 300 mg with visa. Adverse Events All adverse events that were reported in the study evaluating Integra for the treatment of diabetic foot ulcers at a frequency of ≥ 5% in either cohort are presented in Table 1. This table includes adverse events that were both attributed to and not attributed to treatment. The adverse events are listed in descending order according to their frequency in the Integra cohort. A total of 798 adverse events occurred in 216 of the 307 randomized subjects as presented in Table 1. Of the 798 adverse events, 444 occurred in the Control arm, treated with the standard of care established within this trial. Changes in the serum chemistry that were deemed clinically significant by the Investigators were reported as adverse events. Diabetic Foot Ulcer Study Withdrawals due to Adverse Events and Investigator Decision During the Treatment Phase, of the 62 subjects that discontinued, 29 subjects (9. During the Follow-up Phase, of the 57 subjects that discontinued, nine (9) subjects (2. Effectiveness Results Diabetic Foot Ulcer Study Primary Endpoint Complete Wound Closure – Investigator Assessment: A higher percentage of subjects treated with Integra had 100% complete wound closure of the study ulcer (51. The difference between the two treatment groups was statistically significant (p-value = 0. Complete Wound Closure – Computerized Planimetry: Statistically significant results were obtained by planimetric measurement of complete wound closure. The agreement between the planimetric and Investigator assessments was found to be very strong with a Kappa coefficient of 0. The planimetry assessment of the time to healing correlated significantly with the Investigator assessment (p-value < 0. Rate of Wound Size Reduction: Subjects treated with Integra demonstrated a significantly higher rate of wound size reduction compared to subjects treated with control. Rate of wound healing (wound size reduction) determined by week, using planimetric measurements, was significantly higher (p-value = 0. However, this difference between the treatment groups (∆ = 8%) was not statistically significant (p value = 0. Additionally, subjects treated with the Integra indicated significant reduction in Bodily Pain compared to subjects from the Control group (p-value = 0. A difference trending toward significance was noted for Role Physical category (p-value = 0. No significant differences were observed between the two treatment groups for other Quality of Life metrics including General Health, Social Functioning, Role Emotional, Mental Health or Vitality. Integra provides an alternative method for treatment of diabetic full-thickness foot ulcers which have not adequately responded to conventional ulcer therapy. References Copies of the following references, cited in the above section, are provided in full or abstract in Attachment 1. Where abstracts are provided, copies of the articles will be provided upon request. A comparison of the health-related quality of life in patients with diabetic foot ulcers, with a diabetes group and a nondiabetes group from the general population. Consensus recommendations on advancing the standard of care for treating neuropathic foot ulcers in patients with diabetes. Clinical effectiveness of an acellular dermal regenerative tissue matrix compared to standard wound management in healing diabetic foot ulcers: a prospective, randomised, multicentre study. The efficacy and safety of Grafix for the treatment of chronic diabetic foot ulcers: results of a multi-centre, controlled, randomised, blinded, clinical trial. Scalp Reconstruction After Resection of Malignant Fibrous Histiocytoma Utilizing a Dermal Regeneration Template: A Case Report. The use of a dermal regeneration template (Integra) for acute resurfacing and reconstruction of defects created by excision of giant hairy nevi. Integra Artificial Skin as a Useful Adjunct in the Treatment of Purpura Fulminans. The role of serendipity in the evolving indications for Integra dermal regeneration template. Sucessful use of a physiologically acceptable artificial skin in the treatment of extensive burn injury. Observations on the development and clinical use of artificial skin: An attempt to employ regeneration rather than scar formation in wound healing. Effect of Keratinocyte Seeding of Collagen-Glycosaminoglycan Membranes on the Regeneration of Skin in a Porcine Model. The use of artificial dermis in the treatment of chronic and acute wounds: regeneration of dermis and wound healing. Stacking of a dermal regeneration template for reconstruction of a soft-tissue defect after tumor excision from the palm of the hand: a case report. Grafting of deeply burned problem zones in the lower extremity with a dermal substitute. A new technique to resurface wounds with composite biocompatible epidermal graft and artificial skin. Integra as a dermal replacement in a meshed composite skin graft in a rat model: a one-step operative procedure. Collier M; the use of advanced biological and tissue-engineered wound products; Nurs Stand. Artificial skin as a valuable adjunct to surgical treatment of a large squamous cell carcinoma in a patient with epidermolysis bullosa. Reconstructive surgery using an artificial dermis (Integra): results with 39 grafts. Dermal regeneration template for deep hand burns: clinical utility for both early grafting and reconstructive surgery. Experience with Bilaminate Bioartificial Skin Substitute and Ultrathin Skin Grafting in Non-Burn Soft-Tissue Wound Defects. Modulation of scar tissue formation using different dermal regeneration templates in the treatment of experimental full-thickness wounds. Evaluation of the advantages of Integra for covering Chinese flap donor sites: a series of 10 cases. Role of Embryonic Histogenesis in the Healing of Chronic Wounds Using Integra Dermal Regenerative Template. Scattering of Light from Histologic Sections: A New Method for the Analysis of Connective Tissue. Figus A, Leon-Villapalos J, Philp B, Dziewulski P; Severe multiple extensive postburn contractures: a simultaneous approach with total scar tissue excision and resurfacing with dermal regeneration template; J Burn Care Res; 2007 Nov Dec;28(6):913-7. The Use of a Bilaminate Artificial Skin Substitute (Integra™) in Acute Resurfacing of Burns: An Early Experience. Use of dermal regeneration template in contracture release procedures: a Multicenter evaluation. Integra Bioengineered skin substitute for salvage of complex lower extremity wounds. Poster Presentation at the Symposium for Advanced Wound Care, San Diego, California April 24 -27, 2008. Gavenis K, Schmidt-Rohlfing B, Mueller-Rath R, Andereya S, Schneider U; In vitro comparison of six different matrix systems for the cultivation of human chondrocytes; In Vitro Cell Dev Biol Anim. Aesthetic complex reconstruction of the lower leg: application of a dermal substitute (Integra) to an adipofascial flap. Successful Management and Surgical Closure of Chronic and Pathological Wounds using Integra. Strategies to improve the take of commercially available collagen/glycosaminoglycan wound repair material investigated in an animal model. The co-application of sprayed cultured autologous keratinocytes and autologous fibrin sealant in a porcine wound model. Use of an artificial dermis (Integra) for the reconstruction of extensive burn scars in children.
Cheap generic zantac uk
As per the product monograph gastritis gagging zantac 150 mg line, prasugrel is not recommended in patients ≥ 75 years of age because of the increase risk of fatal and intracranial bleeding; or those with body weight < 60 kg because of increased risk of major bleeding due to an increase in exposure to the active metabolite of prasugrel. Continued Coverage: Treatment with ranibizumab should be continued only in people who maintain adequate response to therapy. Coverage will not be approved for patients: With permanent retinal damage as defined by the Royal College of Ophthalmology guidelines Receiving concurrent treatment with verteporfin. April 7, 2020 A 80 Claim Notes: An initial claim of up to two vials of ranibizumab (one vial per eye treated) will be automatically reimbursed when prescribed by an ophthalmologist. If additional medication is required, a request should be made through special authorization. Claims submitted for greater than 1 vial, or submitted within 30 days of a previous claim will not be reimbursed. Claim Notes: Requests for women with chemically-induced menopause will be considered. Clinical Note: Must be used in combination with lactulose unless lactulose is not tolerated. Claim Notes: A maximum of 60 tablets will be reimbursed annually without special authorization. Claim Note: Prescriptions written by New Brunswick psychiatrists do not require special authorization. Clinical Note: When used for greater than 6 months, rivaroxaban is more costly than heparin/warfarin. For patients who have not received four weeks of therapy with a beta blocker or aldosterone antagonist due to an intolerance or contraindication, details must be provided. Claim Notes: Combination therapy with prostacyclin or prostacyclin analogs will not be reimbursed. Clinical Note: For patients who cannot take metformin due to contraindications or intolerances, details must be provided. Claim Note: the maximum dose of sildenafil that will be reimbursed is 20mg three times daily. Clinical Note: Diagnosis must be confirmed by blood, enzymatic, biochemical or genetic testing. Must be prescribed by a hepatologist, gastroenterologist, or infectious disease specialist (or other prescriber experienced in treating a patient with hepatitis C infection). Growth Hormone Deficiency in Children For the treatment of growth hormone deficiency in children under the age of 19. Claim Notes: Must be prescribed by, or in consultation with, an endocrinologist. Turner Syndrome For the treatment of short stature associated with Turner Syndrome in patients whose epiphyses are not closed. Chronic Renal Insufficiency For the treatment of children with growth failure associated with chronic renal insufficiency, up to the time of renal transplantation, who meet the following criteria: A glomerular filtration rate less than or equal to 1. Claim Note: Somatropin must be prescribed by, or in consultation with, a specialist in pediatric nephrology. Clinical Note: † Patients who are asymptomatic and those who are symptomatic but completely ambulant. Sorafenib will not be reimbursed if used with induction or adjuvant intent along with other curative-intent treatments; for maintenance therapy after trans-arterial chemoembolization; or if patients have Child-Pugh B or Child-Pugh C cirrhosis. Patients who are asymptomatic and those who are symptomatic and in bed less than 50% of the time. Clinical Note: the patient must be under the care of a neurologist or a pediatrician. Renewal criteria: Written confirmation that the patient has benefited from therapy and is expected to continue to do so. Pre-treatment risk factors: Low Karnofsky performance status (<80%) Lactate Dehydrogenase level greater than 1. Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. Claim Notes: the prescribed dosage is 50mg daily for four weeks, followed by two weeks off. Requests for patients currently using taliglucerase alfa who do not have a contraindication or intolerance to velaglucerase alfa will be considered for coverage of velaglucerase alfa only. Claim Notes: Must be prescribed by a gastroenterologist or an internal medicine specialist with a specialty in gastroenterology. Claim Notes: Prescriptions written by neurologists licensed by the College of Physicians and Surgeons of New Brunswick do not require special authorization. For on-going evaluation in patients who have documented evidence of thyroid cancer, have undergone appropriate surgical and/or medical management, and require monitoring for recurrence and metastatic disease. As an adjunctive treatment as pre-therapeutic stimulation for radioiodine ablation of thyroid tissue remnants in patients maintained on thyroid hormone suppression therapy who have undergone near-total or total thyroidectomy for well-differentiated thyroid cancer without evidence of distant metastatic thyroid cancer. As with all other antiplatelet treatments the benefit/risk ratio of antithrombotic effect vs. Ticagrelor is contraindicated in patients with active pathological bleeding, in those with a history of intracranial hemorrhage and moderate to severe hepatic impairment. High risk angiographic anatomy is defined as any of the following: left main stenting, high risk bifurcation stenting. Claim Note: Must be prescribed by, or in consultation with, an infectious disease specialist or medical microbiologist. April 7, 2020 A 97 Claim Note: Combined use of tobramycin either concurrently or for antibiotic cycling during off-treatment periods, with other inhaled antibiotics. Clinical Note: A flare is defined as the recurrence of signs or symptoms and/or erythrocyte sedimentation rate ≥ 30 mm/hour. Patients ≥100kg will be approved for 162mg every week, with no dose escalation permitted. If brain metastases are present, patients should be asymptomatic or have stable symptoms. Claim Notes: the maximum quantity reimbursed is limited to four courses of treatment. April 7, 2020 A 100 Approvals will be for 90 mg given at weeks 0, 4 and 16, then every 12 weeks thereafter Initial approval period: 16 weeks. Ulcerative Colitis For the treatment of adult patients with moderately to severely active ulcerative colitis who have a partial Mayo score > 4, and a rectal bleeding subscore ≥ 2 and are: refractory or intolerant to conventional therapy. April 7, 2020 A 101 Renewal requests must include information demonstrating the beneficial effects of the treatment, specifically: a decrease in the partial Mayo score ≥ 2 from baseline, and a decrease in the rectal bleeding subscore ≥1. These criteria are consistent with the Ontario Guidelines for the Treatment of Gaucher Disease. Renewal criteria: Written confirmation that the patient has responded to treatment and there is no evidence of disease progression. For the treatment of epilepsy in those patients who respond inadequately to alternative treatment combinations or in whom other drug combinations have not been tolerated. Clinical Note: Potential benefits conferred by the use of vigabatrin should outweigh the risk of ophthalmologic abnormalities. Renewal criteria: the physician has confirmed that the patient has not experienced disease progression while on Erivedge therapy. Claim Notes: Must be prescribed by a hematologist, infectious disease specialist or medical microbiologist. Intolerance is defined as esophageal ulceration, erosion or stricture, or lower gastrointestinal symptoms severe enough to cause discontinuation of oral bisphosphonates, or swallowing disorders that will increase the risk of esophageal ulceration from oral bisphosphonates. Refractory is defined as a fragility fracture or evidence of a decline in bone mineral density below pre-treatment baseline level, despite adherence to oral bisphosphonates for one year. Patients who had coverage prior to this date will continue to remain eligible for coverage if a special authorization request, documenting the rationale for continued use, is submitted on an annual basis. Patients who had coverage of Hepsera prior to this date will continue to have coverage. For patients who have had a claim paid for quinine between September 1, 2016 and August 31, 2017, quinine will continue to be a benefit until March 1, 2018. After March 1, 2018, a special authorization request, documenting the rationale for continued use, will be required for coverage to be considered. Requests for special authorization will not be considered for new patients or patients who have not had a claim paid for quinine between September 1, 2016 and August 31, 2017.