
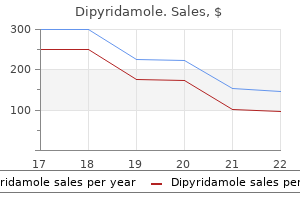
Dipyridamole
Dipyridamole 100mg cheap
At times blood pressure medication that does not lower heart rate order dipyridamole 25 mg amex, the march may segments, or only one part of a single limb, respectively (93). Others view focal cortical children and found that the majority (25 out of 60) began in myoclonus as one manifestation of focal motor seizures, given the face (eight in the periocular and five in the perioral that myoclonus in this instance results from a hypersynchroregion), 17 in the hand, seven in the arm, two in the shoulder, nous discharge arising from a distinct population of cortical and nine in the leg and foot (88). Focal cortiLastly, the term hemiconvulsions refers to unilateral clonic cal myoclonus has been described in patients with focal seizures. In a report of hemiparesis are described in the childhood syndrome of four children with perirolandic cortical dysplasia presenting hemiconvulsion-hemiplegia-epilepsy. In the last 3 years, she has been experiencing daily very brief seizures involving the muscles of the lower face on the right side without alteration of awareness. Because of its very high voltage, the artifact appears widespread on this printed page. Note that in this instance, the terminal muscle jerk is indeed associated with myogenic artifact primarily involving the right-sided derivations. It becomes evident that different Finally, the paradoxical term negative myoclonus is types of tonic seizures utilize different neuroanatomical reserved for cases of sudden, brief relaxations in tonic muscle pathways, which is hardly surprising given that tonic contraction (89). Negative myoclonus (which also encomseizures may be a common clinical manifestation resulting passes the phenomenon of asterixis typically seen in toxicfrom a variety of different pathophysiologies underlying metabolic encephalopathies) is a nonspecific manifestation symptomatic and less frequently idiopathic epilepsies. Nonepileptic focal tonic symptoms can result from subEpileptic negative myoclonus can be either unilateral or cortical pathology. In addition, erogeneous epilepsies ranging from the benign idiopathic paroxysmal tonic phenomena may be seen as part of certain epilepsies to severe epileptic encephalopathies (96). Tonic Seizures Tonic seizures consist of sustained muscle contractions that Oculocephalic Deviation usually last for more than 5 to 10 seconds and result in posand Versive Seizures turing of the limbs or whole body (97). From the standpoint of clinical semiology, tonic seizures can be described according Foerster and Penfield first described versive seizures in 1930. Generalized tonic seizures involve axial and limb contraction of head and eye muscles (105). Unequal or sciousness is often lost by the time a patient experiences verasynchronous contraction of muscle groups involving both sion, occasionally patients may be aware of the forced, involsides of the body results in bilateral asymmetric tonic seizures. Contraction restricted to a portion of the body on one side As discussed, cortical stimulation studies have confirmed only gives rise to focal tonic seizures (98). Stimulation of more posterior points focal tonic seizures are attributed to activation of Brodmann (closer to the central sulcus) elicited contralateral, ipsilateral, area 6 (and the mesial frontal region in particular), some overor upward eye movements. Head rotation was usually seen in lap in symptomatology occurs, with ictal involvement of the conjunction with contralateral eye rotation. The vast majority of these patients had eye deviation to one side resulting in sustained unnatural posiextratemporal epilepsy. The symptomatogenic zone is less clear in cases of about interpreting the direction of eye and head turning, if the symmetric, bilateral tonic seizures. However, these seizures seizure does not become secondarily generalized (111,112). A: Interictal left centroparietal sharp wave as seen on a longitudinal bipolar (upper part) and referential montage (lower part). This interictal finding was present during the first 24 hours of admission for acute exacerbation of his habitual focal motor seizures. C: the ictal onset is punctuated by the appearance of evolving lowto high-amplitude paroxysmal fast activity arising from the left centroparietal region. Chapter 13: Focal Motor Seizures, Epilepsia Partialis Continua, and Supplementary Sensorimotor Seizures 175 have a misleadingly widespread appearance because of the status epilepticus. Consciousness is usually preseries of 19 patients with refractory frontal lobe epilepsy, served, and cerebral function of the uninvolved cortex remains Salanova and associates reported absence of interictal sharp intact. A variety of motor phenomena may be observed in the waves in 7 of 19 (37%) patients (123). Secondary bilaterally context of focal motor status ranging from overt to more subsynchronous discharges may be seen in up to two-thirds of tle motor manifestations, such as epileptic nystagmus for patients with frontal lobe epilepsy (124). As in 1895 as a disorder of persistent localized motor seizures a rule, the patterns are more widespread and more difficult to (134). In general, unilateral involvement with synchronous patients presenting with circumscribed focal clonic seizures, activation of agonists and antagonists is observed. The jerks investigators observed that these seizures were always associare predominantly seen involving the muscles of the upper ated with a localized polyspike and wave intracranial ictal half of the body. By definition, the jerks are spontaneous, although they may be aggravated by physical activity, psychic exertion, and/or sensory stimuli (140). In addition, special stereoencephalographic or electrowas associated with a regional nonprogressive lesion in the corticographic recordings may prove helpful in resolving the sensorimotor cortex, whereas type 2 was typically seen in the underlying spike focus. In a study of 21 adults presenting with may be amenable to curative resective surgery. Hyperglycemia, hyponafew days, but may last as long as 3 months or longer (159). It is nantly in areas of pre-existing focal cerebral damage in 21 important to note that depending on the clinical scenario there patients with evidence of nonketotic hyperglycemia (153). Furthermore, one should not overlook the comin the setting of ketotic hyperglycemia (137,154). There may be very few or no paroxysmal spread, multiregional, or synchronous suggesting progression abnormalities; and the background rhythm may be normal. The typical seizure is freIt should be emphasized that only a minority of patients quently referred to as a bilateral asymmetric tonic seizure. Common descriptions include a feeling of basal frontal regions, the dorsolateral convexity of the frontal tension, pulling, or heaviness in an extremity or a sense that the lobe, and the mesial parietal regions (50). Toward the end of the seizure, a few rhythmic fuse unilateral or bilateral seizure onset. Moreover, extremities are also involved in the tonic posturing, with abducunless the location of the epileptogenic focus/generator has tion at the hips and flexion or extension at the knees (50). They observed that the head and eyes appear as if nosed as having psychogenic nonepileptic seizures (113). Only 50% of 16 at the raised arm, while both lower extremities remain patients with supplementary sensorimotor seizures, who extended or slightly flexed at the hips and knees. Among the less It is important to distinguish midline interictal epilepticommon motor manifestations, coarse movements of the tonic form discharges from vertex sharp transients of sleep. If present, vocaldistinction may not be possible, when sharp waves are seen ization may be prominent during the tonic phase reflecting the only during sleep. The presence of prominent after-going tonic involvement of the diaphragm and laryngeal muscles, slow waves, occurrence of polyspikes, and/or consistently which contract against semiclosed vocal cords (169). In general, the dorsolateral convexity, resulting in unilateral clonic movenormal sleep-related transients display a symmetric field patments or contralateral head version. Clonic moveAppearance of the same midline sharp waves or spikes during ments can be seen toward the end of the tonic seizure (169). Bilateral asymmetric tonic seizures arising from sleep and wakefulness were captured during video-electroencephalograph evaluation.
Buy genuine dipyridamole line
Comparative characteristics of individual medications from the group of sulfonylurea (Glibenclamide blood pressure levels.xls order 25mg dipyridamole with visa, Glipizide), biguanide (Metformin), and other medications (Acarbose). Pharmacological effects, indications, contraindications and clinical uses, dosing regimen. Comparative characteristics of Hydrocortisone acetate, Prednisolone, Dexamethasone, Triamcinolone, Flumetazona, Beclomethasone, Sinaflan. Medications of male sex hormones (Testosterone propionate, Methyltestosterone, Testenat). Medications of estrogen Estrone, Estradiol Dipropionate, Ethinylestradiol, Sinestrol. Mechanism of action, indications and clinical uses, side effects gestagen products progesterone. Comparative characteristics of contraceptives Marvelon, Postinor, Depo-provera, Logest. A woman, 28 years old, was admitted to a hospital in relation a thyroid gland, the patient complained of the dyspeptic with danger of miscarriage. Earlier she had two cases of disorders, appearance of a tumescence on the front surface of preliminary labor. Analysis of the blood revealed leukopenia and luteum that needs to be introduced in this case. The patient suffering from diabetes mellitus complained of of myometrium contractionsfi Which drug should be introduced for the elimination of (vasopressin) the given statefi After removal of the thyroid in a patient the attacks of A * Insulin convulsions are observed. In 3 weeks the signs of arthritis were almost complaints were arisen: undue fatigability, emotional lability, eliminated and the patient stopped taking him drugs. The after there was a relapse, and the new attack was significantly syndrome was diagnosed. What drug should be administered more severe than at the beginning of the disease. Accelerates excretion of iodides from thyroid gland stimulation of labor activity of uterus. Destruction of cells of thyroid gland wrongly introduced almost double dose of insulin. Oppression of metabolism in thyroid gland sweating, tachycardia, convulsions and loss of consciousness 19. At investigation of a sick woman hyperactivity of thyroid diabetes mellitus and is treated by insulin. A 60 years old patient has been suffering within 9 years from hormone diabetes mellitus and is treated by insulin. Oppression of activity of the enzymes participating in doctor has administered to him betaadrenoblocker propranolol synthesis of iodine-containing hormones of thyroid (anaprilinum) in connection with arterial hypertension. Activation of production by hypothalamus of thyroliberine darkening in eyes, arterial pressure was depressed and in some D. Sharp impairment of cerebral circulation treatment by the basic drugs and impossibility of a surgical E. In an hour after last introduction of this 90 drug hypoglycemic coma has developed. What drug oppresses absorption of glucose in small drugs should be used for treatment of this statefi Acute bronchitis is arisen in a patient suffering from diabetes worsened after the injection of insulin with long action duration: mellitus. What antimicrobial drug is undesirable for administering general asthenia, cold sweat, tremor of extremities developed to this patientfi Inhibition of translation derivative of sulfonylurea with average action duration (8-24 E. Antibiotics of Penicillin group suffering from diabetes mellitus with lowered ability of pancreas D. The patient suffering from severe form of diabetes mellitus is examination hyperglycemia and glycosuria are revealed. At the examination of 70 years old patient hyperglycemia is Which of numbered drugs, used for treatment of dermal revealed. What drug is expedient for treatment of this state diseases, is contra-indicated to this patientfi The doctor has administered Retabolilum (nandrolone portions according to phases of a circadian rhythmfi Adaptation of receptors to glucocorticoids had strengthened discontinuation of usage caused exacerbation E. After a A Nuclear receptors course of radiation therapy the doctor has administered a B Membrane receptors synthetic drug of nonsteroid structure which eliminates C Ribosomes stimulatory influence of oestrogens on tumoral growth. The woman of 28 years was admitted to the department of A Gluconeogenesis activation pathology of pregnancy due to threat of abortion. In her B Glycogenogenesis activation anamnesis there are two events of premature birth. Specify a C Intensification of glucose absorption in the bowels drug of the yellow body hormone which should be administered D Inhibition of glycogen synthesis in this case. Indicate the drug which stimulates synthesis of proteins, insulin injection his condition grew exerts positive influence on calcium and nitrogen exchange and worse: there appeared anxiety, cold sweat, tremor of limbs, also promotes increase of appetite and body weight. What drug should 72 During an acute experiment some of diluted solution of be administeredfi This will result in hypersecretion of the B Insulin following hormone: C Mercazolilum A. A doctor 73 Chronic overdosage of glucocorticoids leads to the administered him a medication for internal use. An elderly female patient suffers from the type 2 diabetes 74 A patient with diabetes mellitus complicated by angiopathy mellitus accompanied by obesity, has been recommended a drug which is a sulphonyl urease atherosclerosis, coronary artery disease. Examination revealed that the cervix was mellitus was prescribed glibenclamid internally. Hydrocortisone 71 A nurse accidentally injected a nearly double dose of insulin 76 A patient has a systemic inflammatory lesion of connective to a patient with diabetes mellitus. Enzymatic drugs and their inhibitors the list of basic terms in the topic Term Definition Water-soluble vitamins Drugs like water-soluble vitamins. Lipid soluble vitamins Drugs like lipid soluble vitamins Antivitamins Substances that reduce absorption of vitamins Individual work Theoretical questions: 1. Pharmacology of Thiamine Chloride (bromide), Riboflavin, Pyridoxine, Nicotinic Acid, Cyanocobalamin, Folic Acid, Ascorbic Acid, Calcium Pangamat, Calcium Pantothenate. Strengthening of the antitoxic function of the liver is the parenteral way of introduction of vitamin B12 prefered E. There is an inhibited coagulation in the patient with bile ducts increase of body temperature, etc. What vitamin decreasing the obstruction, bleeding due to the low level of absorbtion of a toxic influence of vitamin D should be administeredfi The patient who was treated by a vitaminic drug for vitamin B1 to eliminate metabolic acidosis. Which biochemical prophylaxis of vasospasms of the brain, has developed mechanism of action of vitamin B1 ensures the positive effectfi Activation of adenylate cyclase trunk, giddiness, sense of flush of blood to a head. Protections of ascorbic acid, assistance to its transport symptoms: pain in arms and legs, impairment of skin sensitivity, and accumulation muscle weakness, edemas and increased amount of pyruvate.
Buy dipyridamole us
Major or Mild Neurocognitive Disorder Due to Multiple Etiologies Diagnostic Criteria A arteriosclerotic heart disease generic 100 mg dipyridamole with amex. Note: Please refer to the diagnostic criteria for the various neurocognitive disorders due to specific medical conditions for guidance on establishing the particular etiologies. The cognitive deficits are not better explained by another mental disorder and do not occur exclusively during the course of a delirium. Coding note: For major neurocognitive disorder due to multiple etiologies, with behavioral disturbance, code 294. All of the etiological medical conditions (with the exception of vascular disease) should be coded and listed separately immediately before major neurocognitive disorder due to multiple etiologies. As this field evolves, it is hoped that both versions will serve clinical practice and research initiatives, respectively. The personality disorders are grouped into three clusters based on descriptive similarities. Cluster C includes avoidant, dependent, and obsessivecompulsive personality disorders. Moreover, individuals frequently present with co-occurring personality disorders from different clusters. Data from the 2001-2002 National Epidemiologic Survey on Alcohol and Related Conditions suggest that approximately 15% of U. Dimensional Models for Personality Disorders the diagnostic approach used in this manual represents the categorical perspective that personality disorders are qualitatively distinct clinical syndromes. An alternative to the categorical approach is the dimensional perspective that personality disorders represent maladaptive variants of personality traits that merge imperceptibly into normality and into one another. Their integration, clinical utility, and relationship with the personality disorder diagnostic categories and various aspects of personality dysfunction are under active investigation. The enduring pattern is inflexible and pervasive across a broad range of personal and social situations. The pattern is stable and cf long duration, and Its onset can be traced back at least to adolescence or early adulthood. The enduring pattern is not attributable to the physiological effects of a substance. The pattern is stable and of long duration, and its onset can be traced back at least to adolescence or early adulthood (Criterion D). Specific diagnostic criteria are also provided for each of the personality disorders included in this chapter. The clinician should assess the stability of personality traits over time and across different situations. Assessment can also be complicated by the fact that the characteristics that define a personality disorder may not be considered problematic by the individual. Deveiopment and Course the features of a personality disorder usually become recognizable during adolescence or early adult life. By definition, a personality disorder is an enduring pattern of thinking, feeling, and behaving that is relatively stable over time. Some types of personality disorder (notably, antisocial and borderline personality disorders) tend to become less evident or to remit with age, whereas this appears to be less true for some other types. The one exception to this is antisocial personality disorder, which cannot be diagnosed in individuals younger than 18 years. Although these differences in prevalence probably reflect real gender differences in the presence of such patterns, clinicians must be cautious not to overdiagnose or underdiagnose certain personality disorders in females or in males because of social stereotypes about typical gender roles and behaviors. Some personality disorders may have a "spectrum" relationship to other mental disorders. Personality disorders must be distinguished from personality traits that do not reach the threshold for a personality disorder. Personality traits are diagnosed as a personality disorder only when they are inflexible, maladaptive, and persisting and cause significant functional impairment or subjective distress. When personality changes emerge and persist after an individual has been exposed to extreme stress, a diagnosis of posttraumatic stress disorder should be considered.
Order cheap dipyridamole on-line
Patients with other seizure types or epilepsy prevent exacerbation of this condition (126) arrhythmia band order dipyridamole discount. Fracture of the of bradycardia, asystole, or both mandate initial lead testing electrode, related to fatigue at the junction between contact in the operating room (24,133,134); the anesthesiologist and the lead wire, was a common problem with early devices should be notified immediately before this test. Substitution of a quadrifilar wire and, later, a following intraoperative bradycardia has been shown to be trifilar lead body coil improved electrode tolerance that had safe, with no change in cardiac rhythm upon initiation of postbeen compromised by repetitive neck motion. Correct placement of the lead electrodes around Model 302 but has a lead body designed with three high the vagus nerve is critical. Two methods have been developed fatigue silicone tubes; the bifurcation is still caudal to the to help confirm correct placement of the electrodes intraopanchor tether, but designed with a smoother transition to eratively (136), depending on the type of anesthesia used for facilitate a smooth strain relief bend. For patients receiving general anesthesia, the structed with a trifilar lead body coil and a continuous bilularynx and vocal cords can be monitored by fiberoptic men lead body silicone tube with the bifurcation cephalad to endoscopy for contraction of the left lateral larynx wall and the anchor tether; this design makes the handling characterisvocal cord tightening. For patients being implanted under tics of the Perennia lead feel stiffer during the implantation local and regional anesthesia, stimulation intensities can be procedure compared with the Model 302 and 304 leads. Incisional infections are unusual and generally respond to Prophylactic antibiotics may be administered both in the antibiotic therapy. The patient can be diswith or without infection occurs in 1% to 2% of implantacharged after the procedure, which usually lasts for less than tions and resolves with aspiration and antibiotics; the rare 1 hour, or can be observed overnight. Discharge education cases of refractory infection require removal of the generashould include care of the incisions and use of the magnet. Unilateral vocal cord paralthe first 3 months of stimulation unless an early response is ysis, which accompanies approximately 1% of implants, noted. The subsequent stimulation schedule is ulator is actually delivering a pulse (Table 70. Inhalation of ipratropium bromide or lowering of the stimulus systemic adverse effects or cognitive side effects (160,161); frequency or current is recommended. An analysis of total mortality and sudden death QoL independent of treatment effect on seizure frequency, as in epileptic patients (to August 1996) revealed the expected well as increased daytime vigilance, have also been reported rate in individuals with severe, intractable epilepsy (149,150). The severe dysseizure or improve the postictal phase empowers the patient phoric or psychotic conditions emerged once seizure frequency and provides a sense of control over epilepsy. Children between $15,000 and $25,000) can be prohibitive without with a history of dysphagia may experience swallowing difficoverage by a third-party payer. These cost benefits are sustained over time and are sufficient to cover or exceed the cost of the device. Diagnosing refractory epilepsy: response to work because of health-related concerns (P 0. Predictors of pharmacoresistant which further reflect positive changes in the QoL of both epilepsy. Antiepileptic drug therapy in the United States: a review of formed among patients both with and without the device clinical studies and unmet needs. Unexpected places: how did vagus nerve stimulation become a treatment for epilepsyfi Prevention of intractable partial seizures by intermittent vagal stimulation in humans: preliminary results. Vagus nerve stimulation dramatically improve the overall treatment of all patients with therapy for partial-onset seizures: a randomized active-control trial. A randomized controlled trial of chronic vagus nerve stimulation for treatseizure types. Earlier use of adjunctive vagus nerve stimulation therapy for refractory epilepsy. Vagus nerve stimulation for 1 year in 269 patients on unchanged antiepileptic drugs. Vagus nerve stimulation for refractory available free to patients, nurses, and physicians from epilepsy: a transatlantic experience. Evaluation of refractory References epilepsy treated with vagus nerve stimulation for up to 5 years. Is vagus nerve stimulation a treatment therapy in patients with refractory epilepsy. Vagus nerve stimulation for symptopediatric patients with refractory epilepsy: retrospective study. Human vagus nerve electrophysiology: a epilepsy in children: indications and experience at the Hospital for Sick guide to vagus nerve stimulation parameters. Anatomical, physiological, and theoretical basis for the dren with refractory epilepsy. Suppression of interictal spikes and seizures by stimula24-month treatment with vagus nerve stimulation on behaviour in children tion of the vagus nerve. Vagus nerve stimulation for treatment of epilepsy does not alter subsequent vagus nerve stimulation-induced seizure supin Rett syndrome. Slow hyperpolarization in cortical neurons: a poseffective in treating catastrophic 1 epilepsy in very young children. Vagus nerve stimulation improves seizure-attenuating effects of vagus nerve stimulation. Left vagal nerve stimulation in children pathways in the inhibitory control of the substantia nigra over generalized with refractory epilepsy. The effects of vagus nerve stimulation therapy on patients with experimental seizures. Vagus nerve stimulation for patients in residential development of electrical amygdaloid kindling in the cat. Vagus nerve stimulation for medicationprolonged stimulation in cats: effects on epileptogenesis (amygdala electriresistant generalized epilepsy. Electrophysiological studies of ulation on adults with pharmacoresistant generalized epilepsy syndromes. Vagus nerve stimulation in response to corpus callosotomy and vagal nerve stimulation. Intraoperative methods for conlation on epileptiform activity recorded from hippocampal depth elecfirmation of correct placement of the vagus nerve stimulator. Deep wound infection after vagus nerve effects at high and low levels of stimulation. Strategies for reoperation after comprehensive tion of vagus nerve pacing in a patient with epilepsy. Tonsillar pain mimicking glosfailed cranial surgery for intractable epilepsy: results from the vagus nerve sopharyngeal neuralgia as a complication of vagus nerve stimulation: case stimulation therapy patient outcome registry. Vagus nerve stimulation: clinical sequent to treating epilepsy by vagus nerve stimulation. A case report of hypomania vagus nerve stimulation earlier in the course of pharmacoresistant epilepsy: following vagus nerve stimulation for refractory epilepsy. Misidentification of vagus nerve stimuon respiration during sleep: a pilot study. Surgical technique for implantation of the neurocybernetic prosside effects after 6 months of vagus nerve stimulation in epilepsy patients. Chronic stimulation of the left vical vagus nerve trunk stimulation for medically refractory epilepsy: vagus nerve in epilepsy: balance effects. Enhanced recognition memory nerve stimulation for the treatment of epilepsy: cardiac complications. Vagus nerve stimulation reduces costs before and 18 months after treatment with vagus nerve stimulation daytime sleepiness in epilepsy patients. Vagus nerve stimulation therapy for life in epileptic patients treated with vagus nerve stimulation. This chapter explores the issues surrounding an initial clinic visit to be uncertain whether a young patient is the definition of intractable epilepsy, with particular reference reporting generalized absence or short-lived complex partial to its relevance to selection of surgical candidacy.
Purchase 25 mg dipyridamole with mastercard
Therapy % School Private school private school home N = 108 N =61 N = 105 N = 53 N = 105 N = 65 Not at all satisfied 5 high blood pressure quiz buy cheap dipyridamole 25 mg on line. The remaining percents for each of the statements represent that parents had neutral feelings about the statements. It will also help to gather information on parent satisfaction with services received. Procedures: I understand that I will be asked to complete a survey about obtaining a diagnosis and treatment services for my child. I will be asked about my emotional reaction to the diagnosis and treatment received. Risks of participation: I understand that there are no known risks associated with this study. If I feel uncomfortable and wish to withdraw, I would be allowed to do so at any time during the participation. Benefits: this survey will be helpful in the development of better services for children with pervasive developmental disorders or autism. However, this survey may help me consolidate my ideas and give me an opportunity to reflect on my experiences. Results from the study will be shared with other professionals and thus will benefit the community. Confidentiality: I understand that the information collected from me during this study will be confidential. The consent form and the sheet containing my name, contact information and the code number will be stored separately in a locked cabinet in the lab that is only used by researchers and research assistants. The identifying information from the online survey will be stored in a separate secure database in the lab. If I wish to have the results of this survey for personal use, I can obtain those from the investigators. Contacts: I may contact the following persons if I wish to obtain further information regarding this study: 1. If I have questions about the research and my rights as a research volunteer, I may contact Dr. There is no penalty for refusal to participate, and I am free to withdraw my consent and participation in this study at any time without any penalty. Any additional information that you can provide in the comments section will be appreciated. If you feel you cannot answer a question or need any clarification, provide an answer that you think might best answer it. Your opinions whether positive or negative are crucial to this study and will be respected. Biological mother Biological father Stepmother Stepfather Foster parent Grandparent Sibling Any other: 3. Family doctor/ Primary care physician Pediatrician Teacher School psychologist Other school personnel. If yes, explain: Case worker/Health Department Case manager/Developmental disabilities specialist Day care personnel Any other: 6. When you noticed these concerns, what was/were your initial reaction/s as a parentfi If yes, explain: Case worker/Health Department Case manager/Developmental disabilities specialist Specialty clinic Any other: 10. What diagnostic evaluations were conducted this second time to make that diagnosisfi I thought that the doctor did not know the child well enough to make the correct diagnosis. I sought help from another doctor with the hope that Autism was the wrong diagnosis for my child. What size was the town (in terms of population) in which the diagnosis was receivedfi What were some ways in which you sought emotional support for you and your family after receiving a diagnosisfi I talked to family I talked to friends I sought spiritual support I sought psychological counseling. I joined autism support groups I took a vacation I isolated myself from my friends and family. I attended autism conferences I started looking for services (within a week of receiving the diagnosis) Any other: 29. Using the scale below, mark the level of difficulty you experienced in finding resources to get a diagnostic assessment. I talked to friends and asked if they knew anything about the disorder or services related to it. I thought he/she will outgrow the problem and so I did not try to seek any help at that time. Visited a Specialist Talked to school about getting services Were told not to worry and he will outgrow, so we were not worried about services at this point. After receiving the diagnosis, did the professional making the diagnosis, spend time with you to discuss the disorderfi How long did the professional spend on the initial discussions about the disorderfi After receiving the diagnosis, did the professional making the diagnosis, spend time with you to discuss your reactionsfi How long did the professional spend on the initial discussions about your reactionsfi After receiving the diagnosis, did the professional making the diagnosis, spend time with you to discuss the possibilities of seeking interventionsfi If yes, then how long did the professional spend on the initial discussions about the possibilities of seeking interventionsfi It would have been helpful if the professional making the diagnosis would have spent time discussing the prognosis and the future recommendations for my child. How old was your child when specific services related to the diagnosis were received for the first timefi Clinic based School based University based training clinic Home intervention State funded services. How many hours per week are being/ were services received in each type of therapy with each of the professionalsfi Speech Clinic based School based University based training clinic Home intervention State funded services. Special education Clinic based University based training clinic Home intervention State funded services. How much money was/is being spent per year approximately on early intervention for your childfi What was the size of the town (in terms of population) in which intervention services were receivedfi Using the scale below, circle the overall level of satisfaction of the current intervention services that are/were receivedfi If the previous services have not changed or no services are being received currently, then skip section 8. How many hours per week are being services received in each type of therapy with each of the professionalsfi Specify: Special education Clinic based University based training clinic Home intervention State funded services. How much money is being spent per year approximately on early intervention for your childfi What size is the town (in terms of population) in which most current intervention services are being receivedfi How many hours do you and your family spend on an average every week on interventionfi
Cheap dipyridamole
Regardless of Munoz 1985) blood pressure form 100 mg dipyridamole mastercard, mood changes are prominent and, although which pharmacologic strategy is employed, it should depressive features may occur, manic symptoms are much always be possible, given the natural course of this disormore common. Delusions may appear and often center on der, to eventually taper and discontinue treatment. Confusion and variable disorientation may also monitored until patients have recovered. Infanticide may occur in up to 4 percent of cases, Subsequent to recovery, patients should be counselled and suicide may also occur. If patients do become pregnant again, close monitoring is Course required post-partum, and a case may also be made for prophylactic use of lithium (Austin 1992; Stewart 1988) or In the natural course of events, symptoms undergo a gradwhichever other agent was effective during the earlier ual, spontaneous, and full remission after a matter of weeks episode, with treatment beginning either immediately or months. Close to one-third of patients will have another post-delivery or, in some highly selected cases, shortly episode should they have another child (Davidson and before anticipated delivery. In the past it was believed that patients presenting a picture similar to that of post-partum psywith what is now termed bipolar disorder and patients chosis. In most cases, however, one will find a history of with major depressive disorder actually suffered from the prior episodes of mania (or depression) occurring outside same illness, namely manic-depressive illness, which the post-partum time span. When manic symptoms are prominent, case reports suggest the usefulness of the onset of bipolar disorder is heralded by the appearance lithium, and divalproex may also be considered; they may of a first episode of illness, which may be manic, depressive, p20. In general, most patients have their first resist at least inwardly smiling when in the presence of a episode in their late teens or early twenties, and by the age euphoric manic. Irritable manics, by contrast, are irascible, of 50 years, over 90 percent of patients will have had their first fault-finding, and accusatory, and when their intemperate episode. The range of age of onset is, however, wide, from as demands are not immediately met, they may erupt into a young as 11 years (McHarg 1954) up to the eighth decade tirade of curses and threats, and indeed may become vio(Charron et al. Manic episodes are often preceded by a prodrome, lasting Although patients may, with great urging, be able momenfrom a few days to a few months, of mild and often indistarily to dam up their words, such respites, when an intertinct manic symptoms. At times, however, there may be litviewer may be able to get a few words in, are but transient tle or no prodrome and the episode may appear quite events before the dam bursts and the interviewer is again abruptly; when this occurs, patients often unaccountably inundated with a torrent of words. Pressure of activity impels patients to be ever on 1989; Bowman and Raymond 1931; Brockington et al. All often become involved in impetuous and ill-considered venpatients who enter a manic episode experience hypomania tures: there may be spending sprees, intense, injudicious, and most progress to acute mania; however, only a minorand often sexual, relationships, and ruinous business venity eventually reach delirious mania. Attempts to reason with such patients, and to bring patients whose manic episodes never pass beyond hypomathem back to some good judgment, are typically in vain. The mood becomes extraordinaronsets, patients may already have passed through hypomaily heightened and labile, and irritability may be quite pronia before being brought to medical attention. Energy of an entire manic episode varies from the extremes of only seems boundless, and the pressure of activity and speech a few days up to many years, or even a decade (Wertham may begin to fragment the overall behavior; patients may 1929). In general, once tion, making one demand, then an opposite one, and be the peak of the episode is reached, symptoms gradually subcompletely incapable of channelling themselves towards side and, after remission finally occurs, many patients, lookany one overall purpose. Delusions are typically either of ing back over what they did, often feel guilt and remorse. Euphoric patients may announce their divinity or dinal manic symptoms of heightened mood, increased lavish listeners with promises to share their great wealth; energy and decreased need for sleep, pressure of speech and irritable patients may accuse others of irrationally thwartflight of ideas, and pressure of activity (Abrams and Taylor ing and persecuting them. The cardinal symptoms of mania may fade, may be one of either euphoria or irritability, or a mixture of and speech and behavior may become profoundly fragthe two, and is often quite labile. Loosening of associations may great good cheer and wish to share their immense enjoyoccur, and patients are often confused; some may become ment with others; they are often full of jokes, puns, and wisemute. Hallucinations and delusions abound and, in addicracks, and their humor is often irresistibly infectious to tion to delusions of grandeur or persecution, one may also those around them. Indeed, it is the rare physician who can see bizarre delusions, including Schneiderian first rank p20. Catatonic stupor may the duration of the euthymic interval varies from as litappear, with immobility, waxy flexibility, and bizarre posturtle as a few hours or days (Bunney et al. Delusions and the total number of episodes experienced by a patient hallucinations may occur (Guze et al. Patients may believe On one extreme, the euthymic interval may be so long that themselves to be the worst of sinners and that they are to be patients have only a couple of episodes in their lifetimes; taken into imprisonment or to execution. Voices may indeed, in the natural course of events, some patients may accuse and condemn them, urging them on to suicide. Euphoric patients, singing and proclaiming their to find patients whose courses are characterized by regularly glory and beneficence, may suddenly be thrust into the alternating manic and depressive episodes. Most patients profoundest of despair, weeping, bereft of all hope and experience either a preponderance of manic or a preponderenergy, and intensely suicidal. Thus, to depressive symptoms may present a startling clinical piclook at two extremes, whereas one patient may have six ture: one patient strode through the ward, shouting episodes of depression and only one of mania throughout unstoppably that he was the greatest of sinners and would his life, another might have a dozen episodes of mania but die of unspeakable tortures; another, weeping uncontrolonly one of depression. Importantly, in cases in which the first episode is depressive, it appears that, in over 90 percent Course of cases, a manic episode will ensue within either 10 years or a total of five episodes of depression, whichever comes first As noted earlier, bipolar disorder is an episodic disorder (Dunner et al. These include serotoninergic consistent with the notion that bipolar disorder represents agents, such as tryptophan or 5-hydroxytryptophan; an inherited disturbance of the structure or function of noradrenergic or dopaminergic agents, such as cocaine, hypothalamic and brainstem nuclei. Most notably, antidepressants In considering a diagnosis of bipolar disorder, the first step may also precipitate mania; although this is more likely with is to ensure that the patient either has had a manic episode tricyclic antidepressants, it has also been noted with newer or is in the midst of one. Acute mania may disorder, and although most suicides tend to occur during be confused with the syndrome of psychosis, given the presa depressive episode, patients in the uncommon mixence of delusions and hallucinations; however, in acute edmanic episodes are actually at highest risk. In delirious mania, however, these cardinal sympEtiology toms, as noted above, may fade from the picture and, at this point, in addition to a syndromal diagnosis of psychosis, Bipolar disorder has a definite genetic component. The incione may also entertain syndromal diagnoses of catatonia or dence of bipolar disorder is higher among the first-degree delirium. It must be emphasized that the easiest and best relatives of probands than among the general population way to make a correct syndromal diagnosis of mania is to (Gershon et al. This may be laborious at times gotic concordance rate is higher than the dizygotic one as patients in acute mania or delirious mania are generally (Bertelsen et al. Furthermore, unable to provide a reliable history, and consequently one adoption studies have demonstrated that the prevalence of may have to contact friends, family members, or co-workers; bipolar disorder is several-fold higher among the biologic the best diagnostic strategy is to establish a typical clinical parents of patients with bipolar disorder than among their evolution of symptoms, from normalcy to hypomania and adoptive parents (Mendlewicz and Rainer 1977). Within the hypothalpathic ones, namely cyclothymia, schizoaffective disorder, amus, overall neuronal loss has been noted in the and post-partum psychosis, figure most prominently on the paraventricular nucleus (Manaye et al. Cyclothymia is in all likelihood merely a forme an increased number of corticotrophin-releasing hormone fruste of bipolar disorder (Akiskal et al. It also appears that there may be a disPost-partum psychosis is characterized by a psychosis, often turbance of cholinergic transmission in bipolar disorder: the with prominent manic symptoms, occurring in the postinfusion of physostigmine reliably precipitates depression in partum period, and is distinguished from bipolar disorder p20. In post-partum psychosis, symptoms occur Most manic patients require admission to a locked unit. Continuation treatment is designed to prevent the Treatment recurrence of symptoms once they have been brought under control during the acute phase of treatment.
Order dipyridamole now
Apical group: which drains all of the other groups arrhythmia kinds safe dipyridamole 25 mg, lies behind the clavicle at the apex of axilla. Level 1: any lymph node below pectoralis minor (first group involved in malignancy), account for 80% of lymph nodes. Typically, fi Pregnancy and lactation: the asymmetry is more noticeable during o Glandular tissue displaces connective tissue. T (hormonal replacement therapy) and late cancer of the breast: hard, nondate of menopause. All other stellates are presumed invasive carcinoma that requires work segmental and up and biopsy. Based on distribution fi fi Architectural distortion without massfi should be treated as stellate lesion. A majority of o Cannot always characterize lesions precisely cysts are found in o More operator-dependent than mammography asymptomatic women on their screening 2. Malignant lesions disturb that pattern but benign lesions follow that Benign mass: a simple pattern. Out of 543 probably benign lesions in 5514 screening mammograms, only 1 was malignant (0. Ductography is useful in fi Carcinoma detecting the location of fi Intra-ductal papilloma (most common cause) fi the lesion within the duct fi Fibrocystic changes and the extent of involvement. This fi Duct ectasia information can be fi Hypothyroid extremely helpful in prefi Pituitary adenoma (prolactin secreting adenoma, can present with surgical planning. Diagnosis: clinically or U/S Management: aspiration both therapeutic and diagnostic under full aseptic technique to prevent infection. If it appeared small on U/S therefis no need to aspirate just reassure the patient. If it accumulates again then aspirate again while reassuring the patient that itfill resolve after lactation period. It mastectomy, axillary can spread to other parts of the body through the lymphatic system nodes then radiotherapy and through the bloodstream. Infiltrating or invasive ductal carcinoma and chemotherapy accounts for about 80 percent of all breast cancers. About 10 to 15 Stage 4 fi no role of percent of invasive breast cancers are invasive lobular carcinomas. The prognosis for medullary carcinoma is better than that for invasive lobular or invasive ductal cancer fi Colloid Carcinoma o this rare type of invasive disease, also called mucinous carcinoma, is formed by mucus-producing cancer cells. Prognosis for colloid carcinoma is better than for invasive lobular or invasive ductal cancer. They have a better prognosis than invasive ductal or lobular carcinomas and are often detected through breast screening. Adenoid cystic carcinomas of the breast heterogeneous clustered have a better prognosis than invasive lobular or ductal carcinoma. It can increase survival for some women with breast cancer and reduce their risk of developing cancer in the opposite breast. Common side effects Uncommon side effects fi Hot flushes or sweats fi Light-headedness, dizziness, fi Irregular menstrual periods (in headache or tiredness women who have not gone through fi Rash the menopause) fi Nausea fi Vaginal irritation, including vaginal dryness or discharge fi Fluid retention and weight gain 5. Any tear may (retroperitoneal organs), which makes it difficult to cause severe hemorrhage. It emerges from the hilum and on the right back below 12th rib, side and opens into the inferior vena cava, and on the left side into the renal enter fascia surrounding adrenal gland > not vein. Arteries comes from: o Inferior phrenic > superior suprarenal artery o Abdominal aorta > middle suprarenal artery o Renal artery > inferior suprarenal artery 1. Primary hypertension + metabolic alkalosis + with or without hypokalemia fi primary hyperaldosteronism a. Secondary to any decrease in renal perfusion fi Causes secondary hyperaldosteronism a. Spironolactone: competitive aldosterone antagonist (corrects pathology caused by aldosterone by binding to its receptors) i. A 30-year-old primigravida complains of headaches, restlessness, sweating, small branches. Valves then close, to prevent the pressure from increasing again by preventing the blood from refluxing. Always exclude secondary causes by doing a thorough physical exam and history and investigations 2. Remove the problematic vein (provided that there is another functioning vein draining the same area) 3. Stocking: (figure 31) fi Physical principle applies pressure, is higher pressure down and lowers pressure up to make blood go up. Ablate vein: (figure 33) fi Chemically or thermally or laser o Denaturation of vein wall collagen > contraction > fibrous obliteration of the vein fi Provided that there is another functioning vein draining the same area. Sclerotherapy (figure 32) fi Sclerotherapy is the injection of a sclerosing agent into a vein, causing an inflammatory reaction in the endothelium of the vein wall. The vein walls adhere together under compression and form a scar (fibrotic tissue) that is absorbed by the body. The spectrum includes: o Cerebrovascular accidents o Coronary artery disease o Renal artery disease o Visceral artery disease (mesenteric) o Peripheral artery disease (Aorto-iliac & upper and lower limb is a marker for atherosclerosis) fi Intermittent claudications fi Limb ischemia 392 2 Atherosclerosis 1. But different arterial trees are fi this is a limb threatening condition affected so patients will fi Pain at rest present with different fi Tissue loss (Ulcer) symptoms. It is very important that you screen for a carotid bruit in all patients with risk factors or over 50. When testing: a) Record bilateral systolic brachial pressure & systolic Ankle pressure (dorslis pedis & post. Patient with acute ischemia 2) 15-year old girl presented with progressive painless unilateral leg swelling: a. Common treatment is lymphatic bypass surgery 3) 50year old male patient with swelling, pigmentation and ulceration around the ankle: a. Needs non-invasive assessment by Doppler and duplex for obstruction and valvular incompetence of the venous system d. Usually managed by amputation of limb 4) 30 year old female, 26 weeks pregnant has painful swollen and pale left lug and her pedal pulses are well felt: a. Heparin is contraindicated in this patient 5) 50 year old diabetic male smoker present with rest pain and gangrene of the 1st toe, the following statement are correct: a. Great saphenous vein starts posterior to the medial malleolus 8) A 32 year old woman presented to the clinic with thickening skin of her medial aspect of the leg, which was associated with dermatitis and hyperpigmentation. Pure motor nerve fi Saturday night palsy: o Very high injury of the radial nerve due to compression of the nerve in the axilla o Everything is affected (wrist, elbow, fingers, thumb and sensation) o Called like this because drunk people sleep with an arm behind the chair that causes the compression fi Summary: o Remember where the lesion happened o Injury to the radial nerve in the axilla: all motor and sensory functions are lost o Injury to the nerve in the spiral groove: triceps is spared and everything else is lost o Injury in the forearm to the posterior interossous nerve: elbow, wrist and sensation are normal. Patient presents with superficial radial nerve injury (cut in the mid forearm) will only have sensory lossfi Clinically, only two things are important when it comes to musclocutaneous nerve injury: biceps and lateral cutaneous nerve of the forearm. Lumps, Carpal tunnel syndrome and nerve compressions, arthritis fi Mechanism of injury and complaint o Trauma, Laceration, Swelling or lump, Arterial or Venous injury, Dislocation, Infection, Numbness 1. Palpation forearm and insert in the hand o Feel Tenderness, sensation, temperature, Capillary refill 3. Open o Closed: fi Completely flexed and then sudden severe hyperextension o Open fi Laceration: Knife being the most common tool for it fi Crush injury fi Degloving injury 4.
Generic dipyridamole 100 mg free shipping
Aphasia syndromes can be classified using three language parameters: fluency arteria japan best buy dipyridamole, repetition and understanding. In France, Henri Hecaen and Francois Lhermitte intensively analyzed language lateralization, childhood aphasia, reading and writing disturbances, and other aphasia related questions. In Canada, Andre Roch Lecours and colleagues published research studies on different aspects of brain organization of language. In Latin America, Fernando Dalmas (Uruguay), Archibaldo Donoso (Chile), and others developed influential research programs on language and speech disturbances associated with brain pathology. Frank Benson, Edith Kaplan, Harold Goodglass, and Arthur L Benton among others ure 1. Different classification and interpretations of aphasia have been proposed (Table 1. From left to right: Henri Hecaen (1912 -1983), Harold Goodglass (1920-2002), Andre Roch Lecours (1936-2005), Edith F. It has been observed that damage in some brain areas result in specific aphasia syndromes (from: For instance, the supplementary motor area frequently is found to be activated during the performance of diverse verbal tasks. A second major advance involves the progressively extended use of standardized procedures for aphasia assessment. Some aphasia tests and test batteries have become especially popular and widely used by speech language pathologists, neurologists, and neuropsychologists worldwide. These tests and protocols include the Boston Diagnostic Aphasia Examination (Goodglass & Kaplan, 1972, 1983, 2001), the Multilingual Aphasia Examination (Benton, Hamsher &, Sivan, 1994), the Western Aphasia Battery (Kertesz, 1982, 2006), the Boston Naming Test (Kaplan, Goodglass, & Weintraub, 1983, 2001), the Token Test (De Renzi & Vignolo, 1962, 1978) and many others. A third major advance in aphasia during the last few decades is the development and extension of diverse rehabilitation techniques and strategies (Basso, 2003; Paradis, 1993). Melodic Intonation Therapy is a good example of an aphasia rehabilitation technique that has become significantly extended and has proven to be successful in non-fluent aphasias (Sparks, Helm & Alberto, 1974). By the same token, some new interpretations and classifications of aphasia disorders have been recently proposed (Table 1. These classifications attempted to integrate contemporary knowledge about brain organization of language in normal and abnormal conditions. According to this proposal, two major dimensions for aphasia classification can be used: aphasia can be peri-Sylvian or ExtraSylvian; aphasia, on the other hand, can be pre-Rolandic or Post-Rolandic. Sub-types for some aphasia are distinguished, and aphasia syndromes are related to anatomical syndromes. Aphasia Handbook 26 Summary Initial reports of oral language disturbances associated with brain damage were presented during the Egyptian Empire. The first report of a disturbance in written language was found during the Roman Empire period. Hippocrates was the first to distinguish that there are two different types of language impairments associated with brain pathology. Later, Wernicke proposed a classification and interpretation of aphasia that has become the most influential framework on current thinking. With the advent of neuroimaging techniques, it has been possible to obtain more accurate clinical/anatomical correlation of diverse language impairments. Furthermore, it has been observed that the critical areas of the brain initially identified relative to their involvement in language processing are more extensive than previously assumed. During recent decades, progressively extended use of standardized procedures for aphasia assessment has been observed, with some test batteries becoming particularly popular in the evaluation of aphasia. Additionally, this has led to development of various rehabilitation techniques as well as extension of new and diverse therapeutic strategies. London: Kegal Paul Aphasia Handbook 29 Chapter 2 Aphasia etiologies Introduction Any abnormal condition affecting the brain areas involved in language ure 2. However, the specific symptoms of the language impairment depend upon the particular brain area that is affected. Damage in the surrounding areas is associated with so-called perisylvian (transcortical) aphasias in the anterior and posterior regions, respectively. Damage in the surrounding area (light grey area) is associated with so-called perisylvian (transcortical) aphasias. Some of them are frequently associated with aphasia, particularly vascular disorders and traumatic head injury; but there are other abnormal brain conditions also potentially associated with aphasia, such as neoplasms (tumors), infections, and degenerative conditions. Although other brain abnormalities (developmental, metabolic, and nutritional diseases; and disorders due to drugs Aphasia Handbook 30 and chemical agents) can be associated with speech and language abnormalities, they do not represent specific aphasia etiologies. Although the last four can be associated with speech and language abnormalities, they do not represent specific aphasia etiologies. In the acute stage of recovery, the most frequent aphasia is global aphasia; however, aphasia profile often changes during the stroke evolution with the most frequent aphasia subtype one year later being anomic aphasia (Table 2. As a matter of fact, anomia represents the most important aphasia symptom manifestation and long-term aphasia sequelae. Stroke can be caused either by a clot obstructing the flow of blood to the brain or by a blood vessel rupturing and preventing blood flow to the brain. Consequently, there are two major types of strokes: obstructive (ischemic) and hemorrhagic. Recovery is observed during the following hours, days, or weeks after the accident. As the results of decreases in edema (swelling) and diaschisis (extended impairment effect due to the broad connectivity of each brain area with the rest of the brain), symptomatology is progressively reduced to focal sequelae. The neurological or Aphasia Handbook 31 neuropsychological residual deficit typically reflects the site and the size of the lesion ure 2. Blood goes to the brain through two different systems: the carotid system and the vertebrobasilar system. The first one originates the anterior and middle cerebral arteries, while the second one originates the posterior cerebral artery. Incidence has been estimated as about 80150/100,000 and the prevalence in over 500/100,000. Stroke also is the leading cause of serious, longterm disability in many countries. About 75% of all strokes occur in people over the age of 65 and the risk of having a stroke more than doubles each decade after the age of 55. Percentage of respondents reporting a history of stroke (according to the Behavioral Risk Factor Surveillance System, United States, 2010). As a matter of fact, there is a significant correspondence between the territory of the middle cerebral artery and the surrounding brain area relative to language. Cortical territory irrigated by the anterior (blue), middle (red) and posterior (yellow) cerebral arteries. Furthermore, the specific aphasia subtype depends upon the particular branch of the middle cerebral artery that is involved (Table 2.