Septra
Buy septra toronto
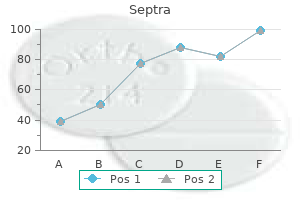
Generally 92507 treatment code buy septra without a prescription, the sexual response cycle in men slows down: the phase of response take longer to achieve, the intensity of sen sation may be reduced, and the genital organs become somewhat less sensitive. Erectile dysfunction is more common with aging due to changes in penile blood flow. The presence and/or treatment of these disorders can result directly or indirectly in urinary, erectile, or libido problems. The chart on the next page shows the range of typical age-related changes in male sexual response. Service providers and health care facilities are strongly encouraged to supplement this ma terial with appropriate medical reference books that present information about these and other conditions in greater depth. Chronic anal fissures may require sim ple surgical treatment to reduce the pressure in the anal canal and allow the fissures to heal. For ex ample, the consumption of refined carbohydrates and animal fats and proteins is much higher in the United States and Europe than in Africa and Asia. Generally, colon cancer is a disease of older individuals who have had little vegetable fiber in their diets or have familial polyposis or chronic ulcerative colitis. Al though the specific bleeding lesions may vary considerably, the initial therapeutic and diagnostic approach to a client remains largely the same. Hematemesis is caused by peptic ulcer, gastritis, esophageal varices or lesions, stomach cancer, benign tumors, traumatic postoperative bleeding, and swallowed blood from lesions in the nose, mouth, or throat. Meletemesis is vomiting of material with gastric juice for at least two hours, which changes the bright red blood present with hematemesis to a brownish color. If the amount and rate of blood loss cause hemodynamic instabil ity, resuscitative measures, including intravenous line and volume replacement, will be required. Thrombosis of external hemorrhoids (see below) is usually seen in young men and is often related to strenuous exercise. This type of exercise results in a temporary increase in intra-abdominal pressure, as well as more pressure on the dilated hemorrhoid veins, which makes them larger, with more stasis. If the pain does not subside within 48 hours, the thrombosed hemorrhoid should be excised under local anesthesia. Exter nal hemorrhoids rarely cause symptoms by themselves, but they may eventually be as sociated with pain, itch, and bleeding. External hemorrhoids increase in size when prolapsing internal hemorrhoids are present because of increased pressure from the in ternal hemorrhoids. In addition, the anal sphincter contracts and reduces blood flow back into the general circulation, which confines it to the hemorrhoids. If the con dition is not treated promptly, it can lead to bleeding, pelvic abscess, peritonitis, and death. Mortality rises dramatically if the injury is penetrative, especially above the lev ator ani, and causes infection. Management Refer the client to a surgeon for biopsy and possible removal of the mass. If the condition is not treated promptly, it can lead to ischemia of the penis and then to gangrene or necrosis of the glans and foreskin. It usually occurs after cleansing of the glans (which requires prior foreskin retraction, after which the foreskin fails to go back to its usual position and act as a hood for the glans) or catheter insertion (which also requires prior foreskin retrac tion). After foreskin retraction, the constricting phimotic ring causes progressive edema, impairs venous return, and threatens the viability of the glans. If the condition needs to be treated and is not managed promptly, it can lead to kidney damage, urinary tract ob struction, and death. As normal secretions accumulate and there is sloughing of the skin, smegma (see Photograph 5 in Appendix H on page H. In severe cases, the opening of the foreskin may be completely closed, inhibiting urination and leading to urinary tract obstruction. School-age boys sprinkle some of this fluid under the foreskin to make their penises bigger, which stay enlarged for a couple of days because of severe inflammation, especially of the foreskin. There is no need for concern if the foreskin is not completely retractable as long as the urethral meatus is visible and nothing is preventing urination. Gently dilate the opening of the foreskin with graduated sounds or dilators until the foreskin is sufficiently open and the risk of blockage is resolved. If the client continues to be unable to urinate, he may need to have a catheter inserted through the urethral meatus into the bladder to relieve the obstruction. Refer the client to a surgeon for circumcision (or a dorsal-slit procedure) if necessary. If the condition is not treated promptly, it can lead to necrosis of the tissue and then to permanent erectile dysfunction. It is also caused by such disorders as leukemia, pelvic tumors, pelvic infection, penile trauma, sickle-cell anemia (the most common cause of priapism in boys), and spinal cord trauma, and by the use of alcohol, antihypertension agents, and cocaine. Longstanding obstruction can lead to decompensation of the bladder, with bladder diverticula, residual urine, incontinence, urinary tract infection, hematuria, and, ultimately, renal failure. It usually is not asso ciated with a disease or illness, and is rarely, but sometimes, caused by prostate cancer. Prostatitis is usually caused by coliform bacteria, but can also be caused by gonococci, enterococci, and trichomonas. Acute bacterial prostatitis is more common in young men, and chronic bacterial prostatitis is more common in older men. Increased numbers of leukocytes are pres ent in prostatic secretions, but no etiologic organisms can be isolated. Dark or red fluid suggests either a scrotal mass, a testicular mass, or blood in the scrotum. Management Refer the client to a surgeon if he has no recent history of scrotal trauma. It also can be caused by an overproduction of fluid re lated to the inflammation of the testes or appendages or to testicular cancer (see page 1. If the condition is not treated promptly, it can lead to bowel necrosis resulting from impaired circulation, with bowel perforation, peritonitis, and death.
Buy septra overnight
Seroepidemiologia treatment of cattle infected with Leptospira borgpetersenii de la Diarrea Viral Bovina en Monteria (Cordoba treatment 4 letter word discount 480mg septra with mastercard, Colombia). Prevalencia de brucelosis bovina, equina y humana en caldas-Colombia Bielanski A. Infectious bovine rhinotracheitis virus infection in naturally infected bull-calves and breeding bulls. Venereal diseases of cattle: natural history, International Seminar on Brucellosis and Tuberculosis in diagnosis, and the role of vaccines in their control. Diarrea viral bovina en terneros y terneras procedentes embryo transfer procedure proposed by the International de Holanda. Tesis de pregrado, Facultad de Medicina Embryo Transfer Society as a method of controlling vertical Veterinaria Universidad Nacional de Colombia, Bogota, 1975. Manejo del problema reproductivo en ganado de Infecciosa Bovina de una explotacion de ganado de carne en el leche. Reactividad serologica y aspectos epidemiologicos Gongora A, Villamil L, Vera V, Ramirez G, Parra J. Neosporosis, Toxoplasmosis, and semen obtained after inoculation of seronegative postpubertal Sarcocystosis in Ruminants Vet. Reproductive losses caused by bovine viral virus 1 in the sperm of the bull from a herd with fertility diarrhea virus and leptospirosis. Tratamiento de semen de bovinos, de pequenos rumiantes y de the prevalence of chlamydiae of bulls from six bull studs in verracos, 2009. Informe Tecnico, Bogota, Subspecies paratuberculosis in Semen of a Breeding Bull D. Vet Clin North Am Food Anim (prophylaxie, traitement, hygiene de la collecte du sperme)11a Pract. Evaluation of reproductive tract and excretion of virus in semen during acute the quality and virological status of semen from bulls acutely and chronic infections. Am J Vet Res 1970; Identication of Tritrichomonas foetus pseudocysts in fresh 31:255-257. Predicao da fertilidade de touros empregados em Isolation of Mycobacterium avium subspecies paratuberculosis monta natural. Theriogenology 2008; 70:495 52 year old patient with chronic destructive pneumonia. Failure of antibiotics psittacosis agent Chlamydia) from semen and epididymis of gentamycin, tylosin, lincomycin and spectinomycin to eliminate bulls with seminal vesiculitis syndrome. SemenTests Presumptive: AcidPhosphatase Confirmatory: MicroscopicSearch SemenTests:AcidPhosphataseTest Presumptivetestforsemen Detectsacidphosphatase,anenzymefoundin largeamountsinsemen Two-stepreactiondevelopsadeeppurplecolorin thepresenceofsemen S Sample SemenTests:MicroscopicExam Humansperm at400xmagnification Size Head Mid-piece Tail Acrosomalcap Profilepearshape SalivaTests AmylaseRadialDiffusionAssay PresumptivetestforSaliva Agarplate(lookslikeJell-O)containingstarch Amylase,anenzymeinsaliva,breaksdownstarch Measuredwithiodinestaining Asofyet,noconfirmatorytest HairMicroscopicExamination Hairvs. ErEctiOnS arE unrEliaBlE spots and blackheads may grow on face, neck, chest and back these are some of the more obvious changes. Erections (hard-ons, boners, stiffies) occur in males of all ages, including babies and old men. The penis is a kind of sponge that fills with blood when a man is sexually excited. So can fear of pregnancy, being laughed at, or of coming too soon (premature ejaculation). While you are soaking in Pull it back and hold the bath, gently pull the it in a stretched foreskin away from you. In some cases, the foreskin can be so tight your doctor may advise using a special cream or having a small operation to loosen the foreskin. Complete removal of the foreskin is called circumciSiOn Some men are circumcised, often for religious reasons. The balls are connected to the penis by a long, thin tube called the vas deferens. Sperm are stored in the epididymis, then are passed along the vas deferens to the prostate gland. It hangs outside the body because sperm need to be kept cooler than your internal body temperature of 37C to be able to fertilise an egg. If you play a sport where a blow, boot, or ball could damage your testicles, wear a plastic protector, or box. This makes it different from most other cancers, which mainly affect older people. Stand in front of a mirror to look for Most lumps and bumps will not be any swelling or change in size. If you have ball (usually the left) may hang slightly any warning signs, talk to your doctor. Most young men ejaculate (come, have an orgasm) for the first time around the start of puberty. Sexual excitement causes muscles at the base of the penis to contract hard and semen to spurt out. Your body is yours to If you and your partner both feel share with whomever you choose. Condoms (male and female) can help Talk about it together, and get protect you and your partner against protection sorted before you have sex. Never use oil-based products, such as moisturising oils or body lotions, with a latex condom as they can damage it and make it more likely to split. To holding the teat go right down to leave a space at the end to catch the semen, or closed end, roll the base. Women can get emergency contraception from their doctor or a contraception or sexual health clinic, some guM clinics and pharmacies. An emergency Iud (intrauterine device) can be fitted in the uterus (womb) within five days of sex or ovulation (release of an egg). A pill with ulipristal acetate must be taken up to five days (120 hours) after sex. A pill Emergency with levonorgestrel must be taken up to three days (72 hours) after sex. Hepatitis B is a liver disease that can cause mild Infants should get their frst dose of hepatitis B illness lasting a few weeks, or it can lead to a serious, vaccine at birth and will usually complete the series lifelong illness.
Purchase septra 480mg line
Vasodilator therapy should not be initiated prior to rate control so as to avoid associated reflex tachy cardia that may increase aortic wall stress medicine on airplanes purchase septra now, leading to propagation or expansion of a thoracic aortic dis section. Urgent surgical consultation should be obtained for all patients diagnosed with thoracic aortic dis section regardless of the anatomic location (ascend ing versus descending) as soon as the diagnosis is made or highly suspected. Acute thoracic aortic dissection involving the ascending aorta should be urgently evaluated for emergent surgical repair because of the high risk of associated life-threatening complications such as rupture. Acute thoracic aortic dissection involving the descending aorta should be managed medically unless life-threatening complications develop (ie, malperfusion syndrome, progression of dissection, enlarging aneurysm, inability to control blood pressure or symptoms). Recommendation for Surgical Intervention for Acute Thoracic Aortic Dissection Class I 1. For patients with ascending thoracic aortic dissec tion, all aneurysmal aorta and the proximal extent of the dissection should be resected. A partially dissect ed aortic root may be repaired with aortic valve re suspension. Extensive dissection of the aortic root should be treated with aortic root replacement with a composite graft or with a valve sparing root replace ment. It is reasonable to treat intramural hematoma similar to aortic dissection in the corresponding seg ment of the aorta. Recommendation for History and Physical Examination for Thoracic Aortic Disease Class I 1. For patients presenting with a history of acute car diac and noncardiac symptoms associated with a sig nificant likelihood of thoracic aortic disease, the clini cian should perform a focused physical examination, including a careful and complete search for arterial perfusion differentials in both upper and lower ex tremities, evidence of visceral ischemia, focal neuro logic deficits, a murmur of aortic regurgitation, bruits, and findings compatible with possible cardiac tam ponade. Recommendation for Medical Treatment of Patients With Thoracic Aortic Diseases Class I 1. Stringent control of hypertension, lipid profile op timization, smoking cessation, and other atheroscle rosis risk-reduction measures should be instituted for patients with small aneurysms not requiring sur gery, as well as for patients who are not considered surgical or stent graft candidates. Antihypertensive therapy should be administered to hypertensive patients with thoracic aortic diseases to achieve a goal of less than 140/90 mm Hg (pa tients without diabetes) or less than 130/80 mm Hg (patients with diabetes or chronic renal disease) to reduce the risk of stroke, myocardial infarction, heart failure, and cardiovascular death. For patients with thoracic aortic aneurysm, it is reasonable to reduce blood pressure with beta block ers and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers to the lowest point pa tients can tolerate without adverse effects. An angiotensin receptor blocker (losartan) is reasonable for patients with Marfan syndrome, to reduce the rate of aortic dilatation unless contraindicated. Recommendations for Asymptomatic Patients With Ascending Aortic Aneurysm (see Figures 6 and 7) Class I 1. Asymptomatic patients with degenerative thoracic aneurysm, chronic aortic dissection, intramural he matoma, penetrating atherosclerotic ulcer, mycotic aneurysm, or pseudoaneurysm, who are otherwise suitable candidates and for whom the ascending aorta or aortic sinus diameter is 5. Patients with Marfan syndrome or other genetically mediated disorders (vascular Ehlers Danlos syndrome, Turner syndrome, bicuspid aortic valve, or familial thoracic aortic aneurysm and dissection) should undergo elective operation at smaller diameters (4. Patients undergoing aortic valve repair or replacement and who have an ascending aorta or aortic root of greater than 4. Patients with symptoms suggestive of expansion of a thoracic aneurysm should be evaluated for prompt surgical intervention unless life expectancy from comorbid conditions is limited or quality of life is substantially impaired. Separate valve and ascending aortic replacement are recommended in patients without significant aortic root dilatation, in elderly patients, or in young patients with minimal dilatation who have aortic valve disease. Patients with Marfan, Loeys-Dietz, and Ehlers Danlos syndromes and other patients with dilatation of the aortic root and sinuses of Valsalva should undergo excision of the sinuses in combination with a modified David reimplantation operation if technically feasible or, if not, root replacement with valved graft conduit. For thoracic aortic aneurysms also involving the proximal aortic arch, partial arch replacement to gether with ascending aorta repair using right sub clavian/axillary artery inflow and hypothermic cir culatory arrest is reasonable. Replacement of the entire aortic arch is reasonable for acute dissection when the arch is aneurysmal or there is extensive aortic arch destruction and leakage. Replacement of the entire aortic arch is reasonable for aneurysms of the entire arch, for chronic dissection when the arch is enlarged, and for distal arch aneurysms that also involve the proximal descending thoracic aorta, usually with the elephant trunk procedure. For patients with low operative risk in whom an isolated degenerative or atherosclerotic aneurysm of the aortic arch is present, operative treatment is reasonable for asymptomatic patients when the diameter of the arch exceeds 5. Recommendations for Descending Thoracic Aorta and Thoracoabdominal Aortic Aneurysms Class I 1. For patients with chronic dissection, particularly if associated with a connective tissue disorder, but without significant comorbid disease, and a de scending thoracic aortic diameter exceeding 5. For patients with degenerative or traumatic aneurysms of the descending thoracic aorta exceeding 5. For patients with thoracoabdominal aneurysms, in whom endovascular stent graft options are limited and surgical morbidity is elevated, elective surgery is recommended if the aortic diameter exceeds 6. For patients with thoracoabdominal aneurysms and with end-organ ischemia or significant stenosis from atherosclerotic visceral artery disease, an additional revascularization procedure is recommended. Expert consensus document on the treatment of descending thoracic aortic disease using endovascular stent-grafts. Recommendations for Counseling and Management of Chronic Aortic Diseases in Pregnancy Class I 1. Women with Marfan syndrome and aortic dilata tion, as well as patients without Marfan syndrome who have known aortic disease, should be coun seled about the risk of aortic dissection as well as the heritable nature of the disease prior to pregnan cy. For all pregnant women with known aortic root or ascending aortic dilatation, monthly or bimonthly echocardiographic measurements of the ascending aortic dimensions are recommended to detect aortic expansion until birth. For imaging of pregnant women with aortic arch, descending, or abdominal aortic dilatation, magnetic resonance imaging (without gadolinium) is recommended over computed tomographic imaging to avoid exposing both the mother and fetus to ionizing radiation. Pregnant women with aortic aneurysms should be delivered where cardiothoracic surgery is available. Fetal delivery via cesarean section is reasonable for patients with significant aortic enlargement, dis section, or severe aortic valve regurgitation. If progressive aortic dilatation and/or advancing aortic valve regurgitation are documented, prophy lactic surgery may be considered. Treatment with a statin is a reasonable option for patients with aortic arch atheroma to reduce the risk of stroke. Recommendations for Brain Protection During Ascending Aortic and Transverse Aortic Arch Surgery Class I 1. A brain protection strategy to prevent stroke and preserve cognitive function should be a key element of the surgical, anesthetic, and perfusion techniques used to accomplish repairs of the ascending aorta and transverse aortic arch. Deep hypothermic circulatory arrest, selective an tegrade brain perfusion, and retrograde brain perfu sion are techniques that alone or in combination are reasonable to minimize brain injury during surgical repairs of the ascending aorta and transverse aortic arch. Perioperative brain hyperthermia is not recom mended in repairs of the ascending aortic and trans verse aortic arch as it is probably injurious to the brain. Recommendations for Spinal Cord Protection During Descending Aortic Open Surgical and Endovascular Repairs Class I 1. Cerebrospinal fluid drainage is recommended as a spinal cord protective strategy in open and endovas cular thoracic aortic repair for patients at high risk of spinal cord ischemic injury. Spinal cord perfusion pressure optimization using techniques, such as proximal aortic pressure main tenance and distal aortic perfusion, is reasonable as an integral part of the surgical, anesthetic, and per fusion strategy in open and endovascular thoracic aortic repair patients at high risk of spinal cord isch emic injury. Moderate systemic hypothermia is reasonable for protection of the spinal cord during open repairs of the descending thoracic aorta. Adjunctive techniques to increase the tolerance of the spinal cord to impaired perfusion may be consid ered during open and endovascular thoracic aortic repair for patients at high risk of spinal cord injury. These include distal perfusion, epidural irrigation with hypothermic solutions, high-dose systemic glu cocorticoids, osmotic diuresis with mannitol, intra thecal papaverine, and cellular metabolic suppres sion with anesthetic agents. Neurophysiological monitoring of the spinal cord (somatosensory evoked potentials or motor evoked potentials) may be considered as a strategy to detect spinal cord ischemia and to guide reimplantation of intercostal arteries and/or hemodynamic optimization to prevent or treat spinal cord ischemia. Computed tomographic imaging or magnetic reso nance imaging of the thoracic aorta is reasonable after a Type A or B aortic dissection or after prophy lactic repair of the aortic root/ascending aorta. Computed tomographic imaging or magnetic resonance imaging of the aorta is reasonable at 1, 3, 6, and 12 months postdissection and, if stable, annually thereafter so that any threatening enlargement can be detected in a timely fashion. When following patients with imaging, utilization of the same modality at the same institution is reasonable, so that similar images of matching anatomic segments can be compared side by side. Surveillance imaging similar to classic aortic dissection is reasonable in patients with intramural hematoma. If there is concern about a leak, a predischarge study is recommended; however, the risk of renal injury should be borne in mind. All patients should be receiving beta blockers after surgery or medically managed aortic dissection, if tolerated.
Generic 480mg septra visa
Firefighters and on-duty deaths from coronary heart disease: a case control study medicine omeprazole 20mg buy septra 480mg otc. The impact of a nap opportunity during the night shift on the performance and alertness of 12-hour shift workers. The effects of training: Goal setting and knowledge of results on safe behavior: A component analysis. Comparing performance on a simulated 12 hour shift rotation in young and older subjects. Tiredness and sleepiness in bus drivers and road accidents in Peru: a quantitative study. The basis for a guidelines manual for the design of fatigue management programs for all transportation modes in Canada. Development of a Fatigue Management Program for Canadian Marine Pilots, Transport Canada, 2002. Roberts S, York J, Design, Development and Evaluation of Driver Wellness Programs, Technical Memorandum Number One: Wellness Literature and Programs Review, September 1997. Differential effects of chronic partial sleep deprivation and stress on serotonin-1A and muscarinic acetylcholine receptor sensitivity. Long workdays versus rest-days: Assessing fatigue and alertness with a portable performance battery. Managing fatigue in operational settings 1: Physiological considerations and countermeasures. Effects of cockpit rest on crew performance and alertness in long-haul operations. Water turnover and changes in body composition during arduous wildfire suppression. Sleep deficit and stress hormones in helicopter pilots on 7-day duty for emergency medical services. Proceedings of the Human Factors and Ergonomics Society 41st Annual Meeting, Albuquerque, New Mexico, September 22-26, 1997. Effects of sleep deprivation and exercise on cognitive, motor performance and mood. Trauma, coping resources, and family functioning in emergency services personnel: a comparative study. Change from slowly rotating 8-hour shifts to rapidly rotating 8-hour and 12-hour shifts using participative shift roster design. Improving alertness and performance in emergency department physicians and nurses: the use of planned naps. Postural balance changes in on-duty firefighters: effect of gear and long work shifts. Working hours as a risk factor for acute myocardial infarction in Japan: case-control study. Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Health and safety problems associated with long working hours: a review of the current position. Comparison of nurse, system and quality patient care outcomes in 8-hour and 12-hour shifts. Effects of sleep deprivation on cognitive ability and skills of pediatrics residents. University of North Carolina Highway Research Center and University of North Carolina School of Medicine. Long-term longitudinal study on the relationship between alternating shift work and the onset of diabetes mellitus in male Japanese workers. Psychosocial work characteristics as risk factors for being injured in an occupational accident. Work-related injuries among firefighter: Sites and circumstances of their occurrence. Effects of shift schedules on fatigue and physiological functions among firefighters during night duty. Effects fo the length and timing of nighttime naps on task performance and physiological function. Sleep and cognitive performance of flight nurses after 12-hour evening versus 18-hour shifts. Comparison of eight and 12 hour shifts: impacts on health, wellbeing, and alertness during the shift. The impact of early and late shift change overs on sleep, health, and well-being in 8 and 12-hour shift systems. Effects of direction of rotation in continuous and discontinuous 8 hour shift systems. Freight transport and non-driving work duties as predictors of falling asleep at the wheel on urban areas of Crete. Associations between overtime and psychological health in high and low reward jobs. Systematic interindividual differences in neurobehavioral impairment from sleep loss: evidence of trait-like differential vulnerability. Investigating systematic individual differences in sleep-deprived performance on a high-fidelity flight simulator. The cumulative cost of additional wakefulness: Doseresponse effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Adverse effects of modest sleep restriction on sleepiness, performance, and inflammatory cytokines. Overweight and obese patients in a primary care population report less sleep than patients with a normal body mass index. Physical, psychosocial, and organizational factors relative to sickness absence: a study based on Sweden Post. Single vehicle roadway departure crashes: Problem size assessment and statistical description. Disentangling the effects of psychological and physical work demands on sleep, recovery and maladaptive chronic stress outcomes within a large sample of Australian nurses. Alterations in the dynamics of circulating ghrelin, adiponectin, and leptin in human obesity. Bright light exposure at night and light attenuation in the morning improve adaptation of night shift workers. Consider the benefits and risk in patients for whom an increase in See full prescribing information for complete boxed warning. Assess the risk of abuse prior to prescribing, and monitor for signs of abuse and dependence while on therapy [see Warnings and Precautions (5. Assess the risk of abuse prior to prescribing, and monitor for signs of abuse and dependence while on therapy. Administer orally in divided doses 2 or 3 times daily, preferably 30 to 45 minutes before meals. Patients who are unable to sleep if medication is taken late in the day should take the last dose before 6 p. If improvement is not observed after appropriate dosage adjustment over a one-month period, the drug should be discontinued. Hypersensitivity reactions, such as angioedema and anaphylactic reactions, have been reported in patients treated with methylphenidate [see Adverse Reactions (6.
Cheap septra amex
These pathways act as a reminder that the patient is the constant in this journey and that the health system has a responsibility to deliver the care experience in an appropriate and coordinated manner medicine qhs septra 480mg. The optimal care pathways are based on a revision of the original patient management frameworks (Department of Health 2007a) which had, for the frst time, attempted to map the cancer pathway in an easily understandable form. The purpose of this work is to improve patient outcomes by facilitating consistent cancer care based on a standardised pathway of care. The pathways are applicable to care whether it is provided in a public or private service. The principles and the expected standards of good cancer care are not expected to differ, even though treatment regimens may vary from patient to patient for a whole variety of reasons. Victoria has undertaken this program of work as part of a national work plan aimed at improving cancer care. A wide range of clinicians, peak health organisations, consumers and carers were consulted and/or participated in their development and I want to thank all concerned for their generous contributions. I am sure that those providing cancer care will fnd the specifc pathways useful in deciding how best to organise service delivery to achieve the best outcomes for those we care for. Importantly, readers should note that these care pathways are not detailed clinical practice guidelines. Step 3 Diagnosis: the following sequence of Special considerations that need to be addressed preoperative investigations should be considered: at this stage may include issues around obesity, Diagnosis, diabetes, early menopause and hormonal changes. The lead clinician may change over time depending on the stage of the care pathway and where care is being provided. Palliative care: Early referral can improve quality of life and, in some cases, survival. Step 5 For premenopausal women, ongoing Follow-up care plan (provide a copy to the assessment of the effects of surgical menopause woman/carer and her general practitioner) outlining: Care after is required after surgery. Step 6 Detection of recurrent disease: Some cases Palliative care: Early referral can improve quality of recurrent disease will be detected by routine of life and, in some cases, survival. Step 7 Palliative care: Consider referral to palliative care if not already involved. The following recommended timeframes are based on expert advice from the Endometrial Cancer Working Group. Primary treatment in two to four weeks of a decision to treat with radiation therapy. The pathway aligns with key service improvement priorities, including providing access to coordinated multidisciplinary care and supportive care and reducing unwanted variation in practice. The optimal cancer care pathway can be used by health services and professionals as a tool to identify gaps in current cancer services and inform quality improvement initiatives across all aspects of the care pathway. The pathway can also be used by clinicians as an information resource and tool to promote discussion and collaboration between health professionals and people affected by cancer. Patient-centred care Patient or consumer-centred care is healthcare that is respectful of, and responsive to , the preferences, needs and values of patients and consumers. Safe and quality care this is provided by appropriately trained and credentialled clinicians, hospitals and clinics that have the equipment and staffng capacity to support safe and high-quality care. Services should routinely be collecting relevant minimum datasets to support benchmarking, quality care and service improvement. Multidisciplinary care this is an integrated team approach to healthcare in which medical and allied health professionals consider all relevant treatment options and collaboratively develop an individual treatment and care plan for each woman. There is increasing evidence that multidisciplinary care improves patient outcomes. Supportive care addresses a wide range of needs across the continuum of care and is increasingly seen as a core component of evidence-based clinical care. All members of the multidisciplinary team have a role in providing supportive care. In addition, support from family, friends, support groups, volunteers and other community-based organisations make an important contribution to supportive care. An important step in providing supportive care is to identify, by routine and systematic screening (using a validated screening tool) of the woman and family, views on issues they require help with for optimal health and quality-of-life outcomes. See the appendix for more information on supportive care and the specifc needs of women with endometrial cancer. This approach seeks to ensure that care is delivered in a logical, connected and timely manner so the medical and personal needs of the woman are met. In the context of cancer, care coordination encompasses multiple aspects of care delivery including multidisciplinary team meetings, supportive care screening/assessment, referral practices, data collection, development of common protocols, information provision and individual clinical treatment. Improving care coordination is the responsibility of all health professionals involved in the care of patients and should therefore be considered in their practice. Communication It is the responsibility of the healthcare system and all people within its employ to ensure the communication needs of patients, their families and carers are met. Every person with cancer will have different communication needs, including cultural and language differences. Research and clinical trials Where practical, patients should be offered the opportunity to participate in research and/or clinical trials at any stage of the care pathway. Research and clinical trials play an important role in establishing effcacy and safety for a range of treatment interventions, as well as establishing the role of psychological, supportive care and palliative care interventions (Sjoquist & Zalcberg 2013). While individual patients may or may not receive a personal beneft from the intervention, there is evidence that outcomes for participants in research and clinical trials are generally improved, perhaps due to the rigour of the process required by the trial. Leading cancer agencies often recommend participation in research and clinical trials as an important part of patient care. Even in the absence of measurable beneft to patients, participation in research and clinical trials will contribute to the care of cancer patients in the future (Peppercorn et al. The pathway describes the optimal cancer care that should be provided at each step for people with endometrial cancer. Step 1: Prevention and early detection Eating a healthy diet, avoiding or limiting alcohol intake, regular exercise and maintaining a healthy body weight may help reduce cancer risk.
Autumn Monkshood (Aconite). Septra.
- What is Aconite?
- How does Aconite work?
- Nerve pain, feeling of coldness, facial paralysis, joint pain, gout, inflammation, wounds, heart problems, and other conditions.
- Dosing considerations for Aconite.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96604
Buy septra 480 mg cheap
While increasing numbers of insurance companies are covering the cost of male chest reconstruction medicine 223 quality 480 mg septra, there are often arbitrary barriers to surgery citing that youth need to be at least 18 years of age prior to undergoing this procedure. Providers should participate in appeal processes so that patients can undergo chest surgery. There are currently no available data that report the positive impact of male chest reconstruction in minors, although a study is underway now. Despite advances in youth care that include the use of puberty blockers and hormones in adolescence, many transgender youth (particularly transfeminine youth) often experience genital dysphoria that results in significant anxiety and depression, and has been reported by June 17, 2016 197 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People many youth as a barrier to quality of life. The ability to develop skills and experience in social relationships is negatively impacted in those youth with genitals that do not correspond to their gender. For transgender adolescents, the very idea of sharing intimate space with a potential partner is often overwhelmingly terrifying, since their transgender status can be disclosed in an instant if their bodies are inadvertently exposed. For many transgender women, this disclosure has resulted in physical assault and all too often, death, at the hands of an angry partner. For many youth, social situations and dating are foregone, and the opportunity to learn necessary social skills during this stage of development is lost. As youth are transitioning at increasingly younger ages, genital surgery is being performed on a case-by-case basis more frequently in minors, in order to address the issues mentioned above. In the absence of solid evidence, providers often must rely on the expert opinions of innovators and thought leaders in the field; many of these expert opinions are expressed in this youth guideline. The four primary authors for this youth protocol represent many years of expertise in clinical care and research, in both academic and community practice settings, and within the disciplines of adolescent medicine, pediatric endocrinology, family medicine, and advanced practice nursing. Young adult psychological outcome after puberty suppression and gender reassignment. National estimates of the timing of sexual maturation and racial differences among U. Mental health of transgender youth in care at an adolescent urban community health center: a matched retrospective cohort study. Pubertal assessment method and baseline characteristics in a mixed longitudinal study of girls. June 17, 2016 198 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 8. Clinical management of gender identity disorder in adolescents: a protocol on psychological and paediatric endocrinology aspects. Puberty suppression in adolescents with gender identity disorder: a prospective follow-up study. Random unstimulated pediatric luteinizing hormone levels are not reliable in the assessment of pubertal suppression during histrelin implant therapy. Subcutaneous Testosterone: An Effective Delivery Mechanism for Masculinizing Young Transgender Men. Induction and Continuation of Puberty in Adolescent Boys with Transdermal Testosterone Gel [Internet]. Apply knowledge of the pathophysiology, etiology, endometrial, ovarian, and cervical cancers. Vaginal and presenting symptoms, and diagnostic evaluation of vulvar cancers are not discussed in this chapter; how each of the gynecologic cancers to care of patients. Evaluate the role and limitations of screening for of cervical cancer can generally be applied to vaginal or early detection of endometrial and ovarian cancers. Develop a treatment plan for a patient with a newly Overall, the etiology of gynecologic cancers is not diagnosed gynecologic cancer. With all three gynecologic malignancies, patients are Introduction generally asymptomatic in the early stage of disease, The gynecologic cancers remain a pharmacothera with symptoms appearing as the cancer progresses. In general, the primary and most efec Although the symptoms of ovarian cancer are nonspe tive treatment is surgery if the cancer is diagnosed in the cifc and have an insidious onset ofen leading to delay early stages. Both endometrial and cervical cancers are in diagnosis, postmenopausal bleeding associated with more likely to be diagnosed in the early stages because of endometrial cancer and postcoital bleeding and pain their symptoms and the availability of efective screen associated with cervical cancer result in women seek ing tools. Regretably, ovarian cancer is denoted the ing gynecologic care and obtaining an earlier diagnosis. Because most women Infertility undergo surgery as part of their primary treatment, the Late menopause (afer age 60 years) staging work-up is completed during surgery. It is rec gynecologic cancers are associated with inherent or ommended that a trained gynecologic oncology sur acquired drug resistance and have a poor prognosis geon complete the tumor-debulking surgery and stag (5-year survival of less than 20%). Another primary mechanism of metastasis the success of the primary surgery to achieve optimal is through the lymphatic system, typically involving tumor reduction (less than 1 cm of detectable disease) the pelvic and para-aortic lymph nodes, which may be is a signifcant prognostic factor, especially for ovarian enlarged upon palpation. Furthermore, treatment of advanced and recur seminate throughout the peritoneum through the peri rent disease is ofen associated with complications that toneal fuid. Finally, distant metastasis may occur from spread of cancer cells through the hematogenous route. Endometrial or uterine cancer is the most common When diagnosed in early stages, interventions are gynecologic cancer in the United States, with more ofen curative with a minimal impact on quality of life. Among the Similar to most cancers, a delay in diagnosis until a more gynecologic cancers, it has the best prognosis with only advanced stage of disease is associated with a much about 7950 (18. Women with a known hereditary risk should have Cervical Cancer annual screening afer age 35, but there is no standard Abnormal Papanicolaou smear ized algorithm, so screening should be based on clini Abnormal vaginal bleeding Abnormal vaginal discharge cal judgment. Women receiving tamoxifen who still Difcult bowel movements have a uterus are also at an increased risk of developing Flank pain endometrial cancer and should have annual screening Hematuria while on therapy and for at least 1 year afer completion Postcoital vaginal bleeding of therapy. Ovarian Cancer Weight change Abdominal discomfort/distention Diagnosis Abdominal fullness/bloating Although the diagnosis of endometrial cancer can be Early satiety confrmed from biopsy, staging for endometrial cancer Indigestion/refux is based on a combination of diagnostic tests and sur Nausea gical examination. When women present with irregular Change in bowel habits (fatulence, diarrhea, or vaginal bleeding and there is a suspicion of endometrial constipation) cancer, an endometrial biopsy is usually performed dur Ascites ing an ofce visit. If the biopsy is negative, then a dila Abdominal pain Urinary urgency/frequency tion and curetage is completed to gather beter sam Irregular vaginal bleeding pling and confrm clinical fndings. Hysteroscopy may also be included in the initial work-up to inspect the uter Etiology ine cavity for polyps and visualization of the endome The etiology of endometrial cancer has not been fully trium, and is ofen done in conjunction with dilation determined. Obesity is associated with a higher per Early stage endometrial cancer can be cured with timely and aggressive treatment involving surgery, centage of adipose tissue, which is where the conver chemotherapy, and/or radiation. T erapeutic goals in sion of androgens to estrogens occurs through several recurrent and metastatic cancer are to alleviate symp pathways including the aromatization of androstene toms and decrease disease progression. The net result is increased estrogen ment of stable disease is ofen considered a reasonable exposure that results in an increased risk of endometrial therapeutic goal for recurrent gynecologic cancers. The combina Surgery is the primary treatment for early stage endo tion of paclitaxel, doxorubicin, and cisplatin for frst-line metrial cancer. This should include a thorough patho treatment of advanced endometrial cancer did improve logic assessment of the depth of myometrial invasion in progression-free and overall survival, but the toxicity relation to the overall myometrial thickness, tumor size associated with this regimen has limited its clinical use. Single-agent regi Radiation alone is a treatment option to consider in mens include gemcitabine, doxorubicin, cisplatin, car patients who are medically inoperable because opera boplatin, topotecan, and paclitaxel (Table 1-1). Morbid obesity and severe cardiopul taxel/carboplatin, gemcitabine/cisplatin, and gem monary disease are the most common reasons a patient citabine/carboplatin have demonstrated an improve with endometrial carcinoma is deemed medically inop ment in progression-free survival. More ofen, radiation is an adjuvant to either cristine have moderate activity but also signifcant tox surgery or chemotherapy. Afer surgery, patients may icities, so these agents are used primarily for sarcoma receive internal radiation therapy (brachytherapy) in tous and endometrioid histologies. In recent based upon the hormone receptor expression of the clinical trials, the use of adjuvant radiation in patients tumor. Megestrol acetate or patients with high-grade tumor and increased depth of medroxyprogesterone can be used for recurrent endo tumor invasion in the myometrium, lymphovascular metrial cancer. Patients should receive the lowest efec space invasion, large tumor volume, and involvement of tive dosage of hormonal agent to limit toxicity. Although the addi of tamoxifen and aromatase inhibitors has been limited tion of radiation does not improve overall survival, it because of low response rates (9% to 14%) and an esti reduces the risk of recurrence by 50%. Finally, most recurrences of endometrial cancer tissue and have the ability to indirectly inhibit cancer are within the vaginal vault and may be treated estrogen pathway (negative feedback), but the overall with salvage external beam radiation with or without response rates have not been impressive (see Table 1-1).
Purchase septra master card
International Journal of Sports to risk of cancer of the right colon and rectum in men medicine urinary tract infection buy septra 480 mg cheap. A prospective study of Matsusaki M, Ikeda M, Tashiro E, Koga M, Miura S, exercise and incidence of diabetes among U. The psychological effects of of different training intensities on 24 hour blood aerobic fitness training: research and theory. Effect of Menotti A, Keys A, Blackburn H, Aravanis C, Dontas A, occupational and recreational activity on the risk of Fidanza F, et al. Twenty-year stroke mortality and colorectal cancer among males: a case-control study. Preschool physical activity level and change in disease and other causes of death. Physical overexercise, and lumbar bone density over age 50 activity, fitness, and health: international proceedings years. Psy Exercise tolerance and disease-related measures in chological effect of chronic physical activity. Coronary heart disease and infarction by heavy physical exertion: protection against physical activity of work: evidence of a national necropsy triggering by regular exertion. Endorphins and exercise: a puzzling relation Coronary heart disease and physical activity of work. Effect of exercise on reform for Americans with severe mental illnesses: depression. Department of Health and Human Services, National Heart, Lung, and Blood Institute Growth and Public Health Service, Centers for Disease Control and Health Study. American Journal of Clinical Nutrition Prevention, National Center for Health Statistics, 1994. The ease Control and Prevention, National Center for Health association between cardiorespiratory fitness and pros Statistics, 1996. The Fifth Report of the Joint ing-induced increase in coronary transport capacity. National Committee on Detection, Evaluation, and Treat Medicine and Science in Sports and Exercise 1994; ment of High Blood Pressure. Is running associated with degenera activity level and other lifestyle characteristics with tive joint disease Some interrelations of physical activity, physiologi a recommendation from the Centers for Disease Con cal fitness, health, and longevity. Journal of the American Medical cal activity and hypertension: an epidemiological view. Physical activity and control study of occupational and dietary factors in personal characteristics associated with depression colorectal cancer in young men by subsite. Physical fitness is a major determinant of femoral physical activity and cancer risk among Finnish female neck and lumbar spine bone mineral density. Inverse relationship between cardiorespi ratory fitness and carotid atherosclerosis. Physical activity Rubin K, Schirduan V, Gendreau P, Sarfarazi M, Mendola and health-related quality of life. Aerobic dance injuries: Journal of Developmental and Behavioral Pediatrics1988; a retrospective study of instructors and participants. Gymnasts exhibit higher bone mass than time and occupational physical activity: risk of death runners despite similar prevalence of amenorrhea and from ischemic heart disease. Effects of physical training on myocardial relation to meniscectomy in former soccer players. Studies on the mechanism of improved glucose vocational physical activity to risk and incidence of control during regular exercise in type 2 (non ischemic heart disease in volunteer male federal em insulin-dependent) diabetes. Low physical activity and worsening of Physical activity and risk of endometrial cancer. Quality of Schuler G, Hambrecht R, Schlierf G, Niebauer J, Hauer K, life assessments in clinical trials. Exercise, fitness, and health: ness, and mortality in a sample of middle-aged men a consensus of current knowledge. Associations of body fat and its distribution with dietary intake, physical activity, al Shimegi S, Yanagita M, Okano H, Yamada M, Fukui H, cohol, and smoking in blacks and whites. Exercise training, serum lipids, and lipopro tein particles: is there a change threshold Acute hyponatremia in ultra activity, fitness, and health: international proceedings endurance athletes. Caloric intake in relation to breast cancer and body mass: the American Health energy output of obese and nonobese adolescent boys.
Buy septra 480mg without prescription
Mild cognitive impairment can affect many areas of cognition such as memory symptoms 5 days before missed period generic septra 480mg without prescription, language, attention, reasoning, judgment, reading and/or writing. Mild cognitive impairment may be irritating but it does not typically change how a person lives their life. Open-label is the opposite of double-blind when neither the researcher nor the participant knows what treatment the participant is receiving. Open-label studies should be interpreted with caution because of the potential for biased conclusions. This benefit above and beyond any actual biological benefit is due instead to the belief that the treatment will work. There is an inability to aim the eyes properly, and persons often show alterations of mood and behavior, including depression and apathy as well as progressive mild dementia. Dosing Recommendations (Always establish a dosing plan with your physician or healthcare provider first! For the best overall result, it is strongly recommended that you adjust the morning jump start dose prior to adjusting the hourly doses. Accuracy of the dose and exact hourly timing between doses is critical for optimal benefit. If you score 10 or more on this test, you should consider whether you are obtaining adequate sleep, need to improve your sleep hygiene and/or need to see a sleep specialist. Use the following scale to choose the most appropriate number for each situation: 0 = would never doze or sleep. He completed his internship and residency in neurology at the Hospital of the University of Pennsylvania, followed by fellowship training in movement disorders at Pennsylvania Hospital in Philadelphia. Houghton began his clinical and academic pursuits at the University of Louisville as an assistant professor and clinical director of the Movement Disorder Surgical Program. He joined the Ochsner Health System in New Orleans, Louisiana, in 2012 as Chief of the Division of Movement and Memory Disorders. Lauren Hawthorne is project specialist at Keck School of Medicine of the University of Southern California. Michael Jakowec, PhD, is associate professor of research neurology at Keck School of Medicine of the University of Southern California. The reader should seek his or her own medical advice, which this publication is not intended to replace or supplement. The preferred agent is not acceptable due to concomitant clinical conditions, such as but not limited to the following: A. Other known disease state or medication contraindication which is not also associated with the requested non-preferred agent. Individual has experienced one of the following adverse effects on previous therapy: 1. Behavior or mood changes interfering with daily activities, including complaints of abdominal distress, sleep problems, or oppositional/rebellious/aggressive behavior. Dextroamphetamine (Dexedrine, Dexedrine Spansules, ProCentra solution (and generic), Zenzedi and generic products): A. Assess the risk of abuse prior to prescribing and monitor for signs of abuse and dependence while on therapy. Strattera (atomoxetine) has a black box warning for suicidal ideation in children and adolescents. Individuals who are started on therapy should be monitored closely for suicidality (suicidal thinking and behavior), clinical worsening, or unusual changes in behavior. Note that market specific restrictions or transition-of-care benefit limitations may apply. Attention Deficit Hyperactivity Disorder: Effectiveness of Treatment in At-Risk Preschoolers; Long-Term Effectiveness in All Ages; and Variability in Prevalence, Diagnosis, and Treatment. Diagnosis and Management of Attention Deficit Hyperactivity Disorder in Primary Care for School-Age Children and Adolescents. Every precaution is taken to ensure that the information provided by each employee is kept in the strictest confidence. One method for determining agency progress in fulfilling these requirements is through the production of reports at certain intervals showing, for example, the number of employees with disabilities who are hired, promoted, trained, or reassigned over a given time period; the percentage of employees with disabilities in the work force and in various grades and occupations; etc. The disability data collected on employees will be used only in the production of reports such as those previously mentioned and not for any purpose that will affect them individually. The only exception to this rule is that the records may be used for selective placement purposes and selecting special populations for mailing of voluntary personnel research surveys. Privacy Act Statement Collection of the requested information is authorized by the Rehabilitation Act of 1973, as amended (29 U.