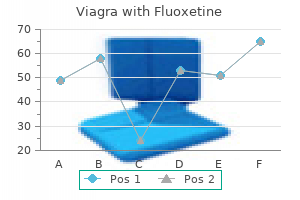
Viagra with Fluoxetine
Purchase viagra with fluoxetine with a mastercard
What action should I take if I Parvovirus infection is spread by infected think I have been exposed About advice should be sought if a person with 50% of non-immune people will become immunodeficiency or a blood disorder infected if there is a case in their suffers parvovirus infection erectile dysfunction at 25 order line viagra with fluoxetine. The incubation period of the contact with a case of parvovirus infection is one to two weeks. Cases are infection should consult the doctor infectious before the onset of the rash supervising her pregnancy even if she and are probably not infectious after the has no symptoms. Vomiting, with or without toxin-producing bacteria and longer for diarrhoea, abdominal cramps and fever others. In recent years the Control measures cholera and hepatitis A (refer to relevant detection of outbreaks of viral origin, Preventive measures sections). The blue book: Guidelines forthe control of infectious diseases 59 Outbreak measures Food and water-borne outbreaks are usually detected following the onset of illness in a group of people who have shared a common meal. International measures International outbreaks are increasingly being recognised, primarily due to the increased trade in food and agricultural products worldwide. Food and water borne pathogens and contaminants have been identified as potential biological terrorism agents. Infection School exclusion: exclude cases from day care centres in personal hygiene is detected more frequently in children child care and school until diarrhoea has such as the need for hand washing than adults. It is readily transmitted in ceased or until a medical certificate of before meals, after toilet use and institutions such as day care centres recovery is produced. The rate of asymptomatic contamination of public water supplies or clothing and other articles concurrently. Method of diagnosis School exclusion criteria apply until Stool microscopy for cysts or diarrhoea has ceased or until a medical Period of communicability trophozoites can be used for diagnosis of certificate of recovery is produced. Food It is communicable for the entire period Giardia however a negative test does not handlers should not attend work until of cyst excretion. Particular attention should be paid to potentially contaminated surfaces in child care centres. Outbreak measures Two or more related cases may indicate an outbreak and requires prompt reporting to the Department of Human Services. It is sometimes occurs, particularly in notified in writing within five days of frequently mild and passes unnoticed. To maintain may cause ectopic pregnancy, infertility Incubation period confidentiality, only the name code (first or chronic pelvic pain. It may cause blindness if Public health significance diagnosing doctor to collect additional not rapidly and adequately treated. Infections Method of diagnosis Medical practitioners have a statutory of the cervix, anus and throat usually Swabs taken from the urethra, cervix, obligation under the Children and Young cause no symptoms. Limited) and the National management Morbidity and Mortality Weekly Report, guidelines for sexually transmissible vol. Invasive Incubation period infections are commonly caused by the incubation period is uncertain. Identification Public health significance Mode of transmission Clinical features and occurrence Hib is transmitted person to person Meningitis Prior to the introduction of Hib vaccine to through respiratory droplet spread and the onset can be sub-acute or sudden the routine immunisation schedule in may also be rarely acquired through with fever, vomiting, lethargy and 1993, Hib disease was the most common contact with infected respiratory meningeal irritation with a bulging serious invasive bacterial infection in discharges. Patients are no longer presents with signs of upper respiratory neurological damage. Progression of disease and acquired it at a much Susceptibility and resistance the infection can lead to complete younger age than non-indigenous Sustained immunity is conferred through respiratory obstruction. Chemoprophylaxis does not eliminate splenectomy sepsis in adults and the need for surveillance and parents of Control of contacts children. For adverse effects and contra contacts develop symptoms consistent Control of case indications to rifampicin, see section on with Hib disease. The blue book: Guidelines forthe control of infectious diseases 69 Hand, foot and mouth disease Victorian statutory requirement Public health significance Control of case Notification is not required. The greatest incidence is in summer and blisters have dried Infectious agent early autumn. Hand foot and mouth disease is caused between three to seven days after being Children with hand, foot and mouth by a virus (usually coxsackie virus A16). Good the skin blisters of hand, foot and mouth persists, or if there are any other personal hygiene is important to prevent disease are infectious until they become worrying symptoms consult your local spread of the infection to others. The virus may also be shed in the faeces There is no connection between this for several weeks after the blisters disease and the foot and mouth disease Further information resolve. Notification is not required however any the incubation period varies from four No human or animal cases of Hendra or new case of these emerging infections to18 days and rarely up to three months Nipah viral disease have been detected should be discussed with the (Hendra virus). Horses are infection for Hendra virus although other viruses of the family Paramyxoviridae: the intermediary host most commonly species such as cats show serological Hendra virus which has so far only been associated with human infection. A Mode of transmission Both viral diseases may cause acute smaller outbreak occurred in 1995 the mode of transmission is unknown infection with a variety of symptoms involving two horses and a farmer from although a respiratory route is including fever, headache, shortness of the northern Queensland town of suspected. The Nipah virus (named after the Baru Sungai frequency of subclinical infections is Nipa village in Malaysia) is closely related Susceptibility and resistance unknown. Pigs are the diagnosis can be made by the the most common intermediary host Control measures detection of specific neutralising IgM and associated with human infection. In the event of a case being linked to exposure in Victoria or elsewhere in Australia, the Department would work closely with relevant animal health authorities and scientists to control possible sources of infection. In cases are not infectious after the first developing countries most people are week of jaundice. Immunity after infection is Illness due to hepatitis A typically causes Notifications have been declining probably lifelong. Inactivated hepatitis A vaccines are illness with few or no symptoms, with available for use in persons two years of jaundice often being absent. A second Method of diagnosis route from person to person or via dose is required for long term protection. Infectious food handlers may the vaccine is recommended for antibodies confirms recent infection. IgG Infection can also occur through workers and emergency services antibodies alone are evidence of past ingestion of contaminated food or water. In the acute stage of the illness, blood raised in contaminated waters may Control of case biochemistry shows elevated harbour the virus. The pattern of the precise timing and mode of Exclude from childcare, school or work liver function tests may be non-specific transmission are often difficult to define.
Sweet Scented Cactus (Cereus). Viagra with Fluoxetine.
- Chest pain, heart failure, heavy menstrual pain and bleeding, hemorrhage, arthritis-like pain, and other conditions.
- Are there any interactions with medications?
- How does Cereus work?
- Dosing considerations for Cereus.
- Are there safety concerns?
- What is Cereus?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96697
Generic viagra with fluoxetine 100/60mg on line
International measures Yellow fever must be notified to the World Health Organization under the International Health Regulations (1969) erectile dysfunction myths and facts discount viagra with fluoxetine 100/60mg on line. In some instances a single case animals from others in such places and will constitute such an unusual under such conditions as to prevent or communicable disease occurrence. Categories of from an infected person or species to a fomes (plural fomites) isolation include: susceptible host, either directly or An object such as a book, wooden indirectly. High level disinfection Disease or condition that is required by refers to the inactivation of all incubation period law to be notified to the State health microorganisms except some bacterial the time interval between initial contact department. Such reservoir of infectious agents precautions involve the use of safe work Any person, animal, or substance in practices and protective barriers, and the which an infectious agent normally lives safe disposal of body substances and and multiplies in such a manner that it soiled material. The blue book: Guidelines forthe control of infectious diseases 247 Appendix 3: Standard and additional precautions General Standard precautions should be Standard precautions for infection Infection control and prevention uses a implemented at all times particularly control in health care settings consist of risk management approach to minimise when patients are undergoing invasive the following work practices: or prevent the transmission of infection. They include good hygiene that should be applied in a health care chlorhexidine (0. Goggles/face-shields Protect face if splash likely Protect face if splash likely Protect face if splash likely Special handling of equipment As per standard precautions As per standard precautions Single use or reprocess before reuse on next patient (includes all equipment in contact with patient) Single room Yes Yes If possible, or cohort with patient or or with the same infection (eg Cohort patients with Cohort patients methicillin-resistant Staphylococcus same infection. Emergency Department at the nearest fluids the exposed person should have a hospital. The status of the source Evaluation and testing of the exposed necessary, unless there is reason to individual may be known at the time of person suspect the source person is the incident. All exposed people viruses, pregnancy testing should be should be assessed to determine the risk offered to women of child-bearing age of tetanus. Dry the public may feel more reassured that the area as wet areas attract contaminants. A scraper the items should then be cleaned and pan should be used to remove the following routine cleaning and absorbed material. Spills should be Cleaning is important particularly in work cleaned up as soon as practical. They should airborne counts as much as ordinary addition to the cleaning performed also be changed immediately following brooms and remove more dust from after each operating session. Single use cleaning items are should not be used in clinical areas delivery, when visibly soiled and at preferred where possible such as where there is a high risk of infection least daily. Microbiological aspects and containment infectious agents Single use sharps should be placed (by facilities. They should also be changed All waste should be stored in secure immediately following the cleaning of areas until collected. Disease or condition Exclusion of cases Exclusion of contacts Amoebiasis (Entamoeba histolytica) Exclude until diarrhoea has ceased Not excluded Campylobacter Exclude until diarrhoea has ceased Not excluded Chickenpox Exclude until fully recovered or for at least 5 days after the eruption Any child with an immune deficiency first appears. Sores on Not excluded exposed surfaces must be covered with a watertight dressing Influenza and influenza like illnesses Exclude until well Not excluded Leprosy Exclude until approval to return has been given by the Secretary Not excluded Measles Exclude until at least 4 days after the onset of rash Immunised contacts not excluded. Unimmunised contacts should be excluded until 14 days after the first day of appearance of rash in the last case. It provides a list of job-specific knowledge, skills, and professional development goals, and even helps you create your personal library of infection prevention-related resources. However, the way you prioritize proceeding through the roadmap will vary from facility to facility and program to program. It will also depend on your background, level of experience, and resources available to you within your infection prevention program. Over the course of four days, you will learn how to develop an effective infection prevention program to protect patients and comply with accrediting and regulatory requirements through evidenced-based best practices that reduce risk. The course introduces the various roles and responsibilities of the infection preventionist. Areas of emphasis include how to prepare surveillance and risk assessment plans, regulatory compliance, and preventing transmission of infectious diseases. Experienced faculty deliver lectures of complex concepts taught in everyday language, facilitate smaller group activities, and lead question/answer sessions along with the sharing of experiences at the individual level. Consider committee and chapter volunteerism, as well as taking action on issues that impact you. The Society and its members focus on building systems, energy efficiency, indoor air quality, refrigeration and sustainability within the industry. Therefore, sterility assurance measures should be used from the time that items are received into the health care facility until they are used. Clean or sterile items to be transported to central processing and storage areas within the facilit6y should be removed from their external shipping containers before they enter the storage areas of the department. Also, whipping cartons, especially those made of corrugated material, serve as generators of and reservoirs for dust. However, this certification exam is geared toward the infection prevention and control professional who has had a least 2 years of full-time experience in infection prevention and control. Infection with this disease leads to death usually within 1 year of onset of illness. Management of neurosurgical instruments and patients exposed to Creutzfeldt-Jakob Disease. Guideline for disinfection and sterilization of prion-contaminated medical instruments. The protocols outline steps hospitals and healthcare facilities can take to reduce the risk of infection and increase the safety of these medical devices. These steps are in addition to meticulously following manufacturer-reprocessing instructions. A new, sterile needle and syringe should always be used to access the medication in a multi-dose vial. The reuse of needles or syringes to access multi-dose vial medication can result in contamination of the medicine with microbes that can be spread to others when the medicine is used again. One recent study1 on head coverings (disposable bouffant or skullcap, cloth cap), identified that the commonly available disposable bouffant hat is the least effective barrier to transmission of particles. Hats Off: A Study of Different Operating Room Headgear Assessed by Environmental Quality Indicators. New disease variants have been included and some chapters have been fundamentally reworked. The 20th edition is a timely update to a milestone reference work that ensures the relevance and usefulness to every public health professional around the world.
Buy viagra with fluoxetine american express
Leukemia can present with vertebral plana but one would suspect diffuse marrow involvement not focal disease as seen in this case erectile dysfunction what is it order 100/60mg viagra with fluoxetine overnight delivery. Osteomyelitis would involve the disc space and two adjacent vertebral bodies not an isolated vertebral lesion seen here. Metastasis Key: A References: the Requisites, Neuroradiology; Third Edition, Mosby Elsevier 2010 560-561. The most common intrdural extramedullary lesion of the spine is a meningioma or schwannoma. Though leptomeningeal metastasis are seem in the intradural extramedullary space, meningiomas are more common. Meningioma Key: A References: the Requisites, Neuroradiology; Third Edition, Mosby Elsevier 2010 384,399-401. Astrocytomas are parenchymal lesions found in the intraxial compartment of the brain. Oligodendroglioma Key: A References: the Requisites, Neuroradiology; Third Edition, Mosby Elsevier 2010: p. Oligodendrigliomas are glial neoplasms that are not cystic and do not occur in the suprasellar region. Machiafava Bignami Disease is in the differential of collosal lesions but patients with this disease have a history of alcoholism. The disease affects the body of the corpus callosum first followed by the genu and then the splenium of the corpus callosum. It typically involves the subcortical U fibers of the anteroinferior temporal lobes, subinsular region, external capsule zones and inferior frontal lobes. The location of the lesions and the presentation are consistent with white matter shear injury as seen in Diffuse axonal Injury in the setting of trauma. Lupus Cerbritis should be considered in a female of reproductive age with a complicated neurologic presentation. Multifocal Cerebral Infarction would not be expected to resolve two weeks post therapy as stated in this case. Cerebral Amyloid Angiopathy is a disease of older patients that presents with foci of hypointensity on susceptibility weighted imaging and hemorrhage. Meningiomas are the most common extra axial neoplasms of the brain that arises from the dura and are associated with an enhancing dural tail which is seen in 72 percent of patients with meningiomas. Oligodendrigliomas are intraxial lesions that occur in the frontal lobes most commonly that are associated with calcification but do not involve the dura. Metastatic disease can involve the dura either via direct extension from the bone or via hematogenous spread. A dural tail in association with a dural metastasis can be seen though not considered characteristic of this entity. Key: A References: the Requisites, Neuroradiology; Third Edition, Mosby Elsevier 2010: p. Focal motor seizures are followed by progressive loss of ipsilateral motor function associated with cognitive decline. Glomus jugulare Key: A References: the Requisites, Neuroradiology; Third Edition, Mosby Elsevier 2010: p. The most common location of paragangliomas in the head and neck is at the level of the carotid body. Though a location of paragangliomas, the carotid body paraganglioma is the most common. Glomus Jugulare is a location/type of paraganglioma occurring at the level of the jugular foramen but the carotid body is the more common location. This is secondary to adjacent inflammation at the extensor pollicis brevis and abductor pollicis longus tendons (De Quervains tenosynovitis). The periosteal reaction of osteomyelitis is usually associated with abnormal underlying bone. The periosteal reaction of hypertrophic osteoarthropathy is more diffuse involving both the radius and ulna. Anterior cruciate ligament Key: D Rationale: There is a Segond fracture, an avulsion fracture at the lateral aspect of the proximal tibia at the site of capsular attachment with contributing oblique fibers from the lateral collateral ligament and iliotibial band, related to varus stress with an accompanying twisting injury. If the force generated is great enough, injury may result in dorsal dislocation of the capitate, with scapholunate dissociation or scaphoid fracture, a perilunate dislocation. You are shown an axial fat-suppressed fast spin echo T2-weighted image of a 16-year-old boy following knee trauma. Rationale: There is impaction at the medial patella and contusion at the lateral aspect of the lateral femoral condyle with thickening and abnormal signal of the medial patellar retinaculum/medial patellofemoral ligament. This is secondary to impaction following spontaneous reduction of a lateral patellofemoral dislocation. Posterior talofibular Key: B Rationale: Inversion injuries of the ankle tend to affect the anterior talofibular ligament first, followed by the calcaneofibular ligament. This is why we so commonly see isolated chronic sprain of the anterior talofibular ligament or chronic sprain of both the anterior talofibular and calcaneofibular ligaments. Parosteal Key: A Rationale: Osteosarcoma secondary to underlying pathology or radiation has the worst prognosis. The prognosis of telangiectatic osteosarcoma is similar to that of the more common subtype. Periosteal osteosarcoma and paraosteal osteosarcoma have a much better prognosis, both being lower grade tumors. Transient osteoporosis of the hip (a focal phenomenon secondary to underlying stress fracture) involves the head and neck only, with no clearly defined advancing edge. Key: B Rationale: the humeral head is dislocated inferiorly with the arm held in an abducted position. Luxatio erecta or inferior shoulder dislocation is the least common type of glenohumeral dislocation. What is one of the characteristic radiographic findings of erosive osteoarthritis Central erosion Key: D Rationale: the characteristic radiographic appearance of erosive osteoarthritis reflects osteoarthritis (joint space narrowing, osteophyte formation, subchondral sclerosis) and central erosion, all of which contributes to the "gull-wing" configuration. Scattered mitosis and hypercellularity D Diffuse high-signal intensity on T2W images Key: A Rationale: There is a soft tissue mass at the plantar aspect of the metatarsal heads at the third webspace. This is not a true peripheral nerve sheath tumor but rather a mass of inflammation, fibrosis and torn peripheral nerve, a sequela of a compression neuropathy. There is scintigraphic evidence of diffuse peritonitis Key: A References: nd Bennet P, Oza, U. Images of the abdomen and pelvis show free spillage of the tracer into the peritoneal catheter. These findings confirm a patent shunt from the reservoir to the peritoneal cavity. The activity courses normally through the efferent limb as shown on the anterior chest and abdomen images. The final image of the abdomen and pelvis shows dissipation of the tracer throughout the peritoneal cavity. This study is not used to diagnose peritonitis or other inflammatory/infectious process. Insensitivity of forearm bone density measurement secondary to preponderance of cortical bone C. Underestimation of the bone density in the spine and hip secondary to arthritic changes D. The forearm has more cortical bone than the spine and hip, which have more cancellous bone.
Order generic viagra with fluoxetine pills
Abdominal aortic aneurysm expansion: Risk factors and time intervals for surveillance erectile dysfunction drugs cialis cheap viagra with fluoxetine 100/60 mg online, Circulation, 2004; 90:16-21. Diabetic foot disorders: a clinical practice guideline (2006 revision), Journal of Foot and Ankle Surgery, 2006; 45(5):S1-S66. Complaints associated with abdominal or pelvic pain [One of the following] 112-118 A. Obstructive uropathy or hydronephrosis with negative ultrasound [One of the following] 1. Prior to colonoscopy (if requested by the physician who will be performing the endoscopy. Routine follow-up study after treatment, including evaluation for removal of drain Page 551 of 794 E. Appendicitis (In children and pregnant women, ultrasound is the initial study except for follow up of known appendicitis with suspected complications. Routine follow-up study after treatment, including evaluation for removal of drain d. Routine follow-up study after treatment, including evaluation for removal of drain G. Patient is a male age 65 to 75 who has smoked at least 100 cigarettes in his lifetime D. If no dilation for the aortic root or ascending thoracic aorta is found, there is no evidence-based data to support continued surveillance imaging 21-23 V. Pancreatitis with abdominal pain or pancreatic pseudocyst [One of the following] A. Initial scan at onset of abdominal pain but serum amylase and lipase are not >3 times normal but with severe abdominal pain and epigastric pain that increases rapidly in severity and persists without any relief 3. Suspected pancreatitis and ultrasound findings do not explain symptoms(gallstones, common duct, etc) 4. Evaluation of patients with suspicion of pancreatic ductal anomalies that may predispose patients to pancreatitis 7. Known pancreatitis with any of the following allows for repeat exams if present [One of the following] 1. Pancreatic lesions of any size with concerning features (mural nodules, dilated duct, pain, positive cytology, jaundice, worsening diabetes, etc. If enlarging on follow up imaging: Consider resection for possible primary adrenocortical carcinoma; biochemical evaluation to determine functional status and to exclude pheochromocytoma prior to resection. Biochemical assays to determine functional status to exclude pheochromocytoma prior to resection b. Biochemical evaluation to determine functional status and exclude pheochromocytoma prior to biopsy/resection. Biochemical evaluation to determine functional status and exclude pheochromocytoma prior to biopsy/resection 2. Consider biochemical assays to determine functional status and exclude pheochromocytoma prior to biopsy/resection X. Concomitant femur fracture (may indicate blunt abdominal trauma in patients struck by automobiles) 13. Known or suspected primary or recurrent Spigelian hernia (anterior abdominal wall hernia through the semilunar line), ventral hernia, umbilical, or incisional hernia 1. Evaluation of elevated liver function tests and non-diagnostic 99,100 ultrasound A. Unilateral leg edema with venous Doppler excluding venous insufficiency or varicose veins [One of the following] A. Monitoring response to treatment for locally advanced, unresectable or metastatic lung cancer Page 565 of 794 3. To establish a post-treatment baseline, after completion of chemotherapy, radiation therapy or surgery 6. New/worsening signs or symptoms related to the pelvis Primary Peritoneal Mesothelioma: C. To establish a post-treatment baseline, after completion of chemotherapy and/or radiation therapy and prior to surgical resection 3. Screening patients at high risk of pancreatic cancer (to begin at age 40 or 10 years younger than the youngest affected family member) with any one of the following risk factors: a. Familial pancreatic cancer ((two or more first degree relatives or any combination of 3 or more first/second degree relatives) Page 571 of 794 d. After completion of neoadjuvant chemotherapy or definitive chemotherapy and/or radiation therapy to establish a new post-treatment baseline 3. Monitoring response to treatment for locally advanced, unresectable or metastatic cancer a. After completion of chemotherapy and/or radiation therapy to establish a new post-treatment baseline 4. New signs or symptoms related to the abdomen and/or pelvis Chordoma Page 573 of 794 D. Sarcoma may present with any of the following histologies: Myxoid/round cell liposarcoma, epithelioid sarcoma, angiosarcoma, leiomyosarcoma, endometrial stromal sarcoma, rhabdomyosarcoma, clear cell sarcoma, hemangiopericytoma and undifferentiated sarcoma. Further imaging indicated to follow up on previously seen abnormalities or new signs/symptoms related to the abdomen/pelvis 2. Ocular/Orbital Melanoma Every 6 months for 2 years, then annually for 3 years L. Transitional cell cancer [arising from the bladder, ureters, prostate, urethra and renal pelvis] A. After completion of neoadjuvant chemotherapy and/or radiation therapy and prior to surgical resection 3. Initial staging of newly diagnosed Prostate cancer only for one of the following: a. At the completion of chemotherapy, radiation therapy or surgery to establish a new post-treatment baseline 3. Monitoring response to chemotherapy only for known metastatic disease every 2 cycles (6 to 8 weeks) 3. Restaging after completion of primary (upfront) radiation therapy and/or chemotherapy 3.
Purchase 100/60 mg viagra with fluoxetine with amex
Members of the health care team can help prepare you and your child for the test and help your child fnd positive ways to cope with the test erectile dysfunction endovascular treatment purchase generic viagra with fluoxetine line. Below is information on the different types of medicines available to help your child through their tests and procedures. This medicine may be in the form of a topical cream, patch, spray or other device placed on the skin. When necessary, after the medicine has numbed the surface of the skin, another numbing medicine can also be given using a small needle that is placed a little bit deeper into the tissue. This numbing medicine may burn a little bit at frst, but after one to two minutes, the tissue will feel numb all the way down to the bone. Whatever the level of sedation your child needs, the goal is the same: to keep your child comfortable and free from pain. Talk with your health care team to learn more about what type of sedation is best for your child and what sedation guidelines are followed by your hospital. This list includes many common tests, but your child may have tests that are not on this list. An open biopsy is when the skin is opened during surgery to get a sample of tissue. A closed biopsy is when a needle is put into the tissue without cutting open the skin. Some biopsies are done in the operating room under general anesthesia (completely asleep). The type of anesthesia used will depend on where the tumor is in the body and the condition of your child. Bone marrow is found in the center of bones and is made up of both spongy bone and liquid marrow. For this test, a needle is placed in a bone (usually the hipbone) and a small sample of liquid bone marrow is pulled into a syringe. Talk with your health care provider about the way your hospital manages pain with bone marrow aspirates. There is a small chance that your child could bleed under the skin or get an infection where the needle was placed. Bone marrow biopsies also help determine if the bone marrow cells are healthy and if there are cancer cells present. For this test, a needle is placed in a bone (usually the hipbone), and a small piece of the spongy bone marrow is removed and sent to the laboratory for testing. Talk with your health care provider about the way your hospital manages pain with bone marrow biopsies. There is a small chance that your child may bleed under the skin or get an infection where the needle was placed. Your child will be asked to lie on their side with the chin tucked to the chest and knees pulled up. In some cases children can sit up and curl the back by tucking the chin to the chest. When the back is in a curved position, a needle can be placed in between the bones of the spine (vertebrae). Fluid from the spinal canal can then be removed through the needle and dripped into a tube that is sent to the laboratory to be tested. For some types of cancer, chemotherapy may be given into the spinal canal through the same needle after the fuid is removed for testing. Talk with your health care provider about the way your hospital manages pain with lumbar punctures. After the test there is a small chance that your child may get an infection or bleed under the skin. This is done by injecting a small amount of radioactive isotope, or tracer, into a vein. Your child will hear and feel a rhythmic knocking sound, like a drumbeat, when the machine is scanning. You may not be able to stay in the same room with your child during this test; however, you and the staff can always hear and see your child. Before and after the scan, a special medicine is given to protect the thyroid gland from the radioactive substance in the tracer. For instance, there are special dietary instructions to follow, and there may be additional instructions if your child needs sedation. A small round probe (transducer) is then placed on the jelly and moved around to get a clear picture of the tissue or organ. For example, x-rays can show if a bone is broken or if there is an infection or fuid in the lungs. The tests also show if the levels of sodium, potassium, and many other elements in the blood are normal. One reason is to see how treatment is affecting the bone marrow, where blood cells are made. Other reasons are to see if your child needs a transfusion or is at increased risk for infection. The amounts of creatinine in the blood and in the urine are used together to measure kidney function. After the tracer is given, follow-up tests are done to determine how quickly the tracer passes through the kidneys and is removed from the body. Certain genes may be partly responsible for how medicines are processed by the body. By performing these blood tests, we hope to learn how to better use these medicines in children with cancer. In some childhood cancers, blood and/or body fuids can be tested for specifc tumor markers to help determine if cancer is present and monitor response to treatment. A small amount of urine is collected in a cup and sent to the laboratory to be tested. Your child may wear headphones and/or go into a soundproof booth for this testing. This probe sends sound waves to the heart, and the returning sound waves create a picture of the heart. Small stickers, called leads, are placed on the chest and sometimes on the arms and legs. When the rhythm needs to be measured over several hours or a day, the test equipment is called a Holter monitor. The test measures how much air the lungs can hold and how well your child can push air out of the lungs. Your child will be asked to blow into a plastic mouthpiece connected to a machine. The machine measures the amount of air breathed in and the force of the air breathed in and out. Your child will probably be asked to repeat the test a few times to get an accurate reading. The tremendous progress that has taken place in developing successful treatments for children with cancer has been made possible through clinical trials. For each new clinical trial, a group of doctors, nurses, and other experts plan how the treatment will be given. New clinical trials are planned based on the results of past trials, taking the best known therapy and asking what might make it better. The knowledge gained from clinical trials has improved treatment for children with cancer by increasing survival rates and reducing side effects and long-term effects of therapy. Each phase of a clinical trial builds on the previous phases, with the overall goal of developing better treatments.
Discount viagra with fluoxetine 100/60mg otc
When re-useable and appropriate for the type of donor and the type instruments are used impotence natural food cheap generic viagra with fluoxetine canada, a validated cleaning, disinfec of tissue or cells procured and must be standardised. Usually, this will quality(see Chapter 5); extend to being scrubbed as for surgery and involve e steps that minimise the risk of microbiological wearing a sterile gown, sterile gloves, glasses and a contamination during procurement (see this face shield or protective mask. Tese are described ling and transporting samples of donor blood more fully in Part B of this Guide (tissue-specifc or other samples to the laboratory for testing chapters), but generally include: (see this chapter, and Chapters 5 and 13); a Post mortem procurement time limits. It is j procedures that protect the health and safety recommended that tissue should be procured of the living donor (see Chapters 17 and 23-29). Alternative time limits for cerning (see Chapter 15): procurement should be validated by quality a knowledge of deviations from approved pro assessments and tests for microbiological con cedures that occurred or that are suspected to tamination. If the procurement is performed because of long warm ischaemia times; simultaneously with organ procurement, the se c Fewer equipment and consumables resources quence varies starting with the tissues from the cav needed. Timely and efective communication with d Organisation and co-ordination of the pro all parties involved can help to meet expectations in curement; regard to delays, as well as aesthetic considerations e Evaluation of abnormal procurement fndings; when tissues are procured from areas of the body f Review of tissue packaging and labelling; that may be visible. Processing at the procurement stage The sequence in which the various tissues are procured must be well defned to assure the quality of Microbiological safety during the procure each type of tissue. The recommended procurement ment of tissues or cells must always be considered; sequence, whether carried out by separate teams or but control of contamination and cross-contamina by a multi-tissue team, is: skin, eyes/corneas, cardio tion at the procurement site is typically less stringent vascular and musculoskeletal. Justifcations for this than the controls applied in a tissue establishment recommended procurement fow include: (see Chapters 2, 9 and 16-29). However, if processing, including shaping, provided by the presence of musculoskeletal cleaning, sizing and fnal packaging (for direct distri tissues (in particular, bones) facilitates the bution) at the procurement site is unavoidable, its du procedure. Some not possible, an in-process (active) environmental cardiovascular tissues. Sample cultures Where a tissue donor has already donated of the tissues or cells procured should also be taken organs, all surgical approaches to obtain the organs (see Chapter 9) and an appropriately validated culture must have been sutured to maintain as far as possible method must be used (see Chapter 2). Tese coded data should be eration of the immune status of the recipient, if entered in a registry maintained for this purpose. In summary, before the procurement of tissues and cells may proceed, an authorised person. Temporary storage and transportation to b that consent for the procurement has been ob the tissue establishment tained in accordance with local laws; c how and by whom the donor has been reliably Once the tissue is procured and until it arrives identifed. Records to demonstrate compliance organisation) must produce a report, recorded at with specifed storage conditions must be completed the time of procurement, which must be forwarded and maintained. Care should be taken to maintain donor con fdentiality if the procurement report is forwarded to 6. Terefore tissue depending on the type of donor, could contain the Pestablishments must have procedures in place following: that address the retention of procurement records, a donor identifcation data (frst name, family which include descriptive documentation of the steps name, date of birth and sex, as well as how and taken, the materials and equipment used, and iden by whom the donor was identifed, or donor tifcation of the personnel involved. This will be the dona throughout a specifed retention period, and in com tion identifcation sequence of the Single Euro pliance with data protection legislation. When ment facility (location or description of the tissues and cells are to be sent across national borders, physical area where procurement took place) potential language barriers should be addressed and (see Appendix 17); a common language agreed for all documentation d a list of observations during the physical ex related to donors, tissues and cells. Introduction Although it brings great benefts, processing can also introduce risks. For these reasons, all the necessary steps must The opportunity to process tissues and cells be carried out within a comprehensive quality man brings great advantages. However, if the that are not necessary for the success of the eye or whole knee was removed from the donor, and transplant and the inactivation of microbes or corneas and menisci were then excised at the pro even sterilisation in circumstances where cell curement site, this activity would be classifed as pro viability is not required. Processing in the procurement facility, either during or afer procurement, is not recommended Processing includes a range of activities such as because it is important to prevent microbial contam (but not limited to) cutting, grinding, centrifugation, ination, or cross-contamination of procured tissues. Acceptance criteria: receipt at The data that must be registered at the tissue the tissue establishment establishment include: ach tissue establishment must have a docu a consent/authorisation, including the pur Emented policy and specifcations against which pose(s) for which the tissues and cells may each consignment of tissues and cells (including be used and any specifc instructions for dis blood samples from donors) is verifed. Tese specif posal if the tissues or cells are not used for the cations must include the technical requirements and purpose for which consent was obtained; other criteria considered by the tissue establishment b all required records relating to the procure to be essential for the maintenance of acceptable ment and donor medical/behavioural history quality. Upon receipt of the documentation, the pro Review of the relevant donor/procurement in curement report and shipping record (if the donation formation, and thus acceptance of the donation, needs was transported by a third party) should be cross to be carried out by specifed/authorised persons. The tissue establishment must have docu The packaging, the tissues and cells received mented procedures for the management and segre and any accompanying samples should all be exam gation of non-conforming tissues or cells, or those ined to ensure that they have not been damaged or with incomplete test results for infectious diseases, to tampered with during transit. Such transport should be direct, without in port method has been used) and storage tem termediate stops where possible, to ensure the safety perature and time in transit; and maintenance of the temperature conditions of d identifcation of the donor (donation number); the tissues and cells and prevent unauthorised access. Upon receipt of the tissues and cells, the tissue in a defned, separated and adequate location and establishment should assign a unique identifcation under appropriate conditions until they, along with code to the material if this has not already been done 102 7. This code can then be extended to of medicinal allergies (such as to antibiotics) of the identify the diferent products and batches of tissues recipient. Whenever possible, reagents used for pro or cells obtained during processing and storage. Reagents that are not of appro guidance on labelling and Chapter 14 for further priate grade must undergo validation for the intended guidance on traceability). Reagents not approved for human use may least the following information: be used if an equivalent reagent of appropriate grade a unique identifcation; is not available, if the use has been authorised by na b identifcation of the tissue establishment; tional authorities or supported by extensive medical c type and characteristic of the product; literature. The origin, characteristic conditions for d batch number (if applicable); storage (physical, chemical, microbiological) and e recipient name (if applicable). Reagents should be used in a manner con The coded data must be entered in a register sistent with the instructions provided by the manu maintained for the purpose. Critical reagents and consumables should have written specifcations describing, if applicable: a description of the materials, including: 7. Each step of pro acceptance limits; cessing must be carried out under defned conditions d storage conditions and precautions; to guarantee the quality and safety of tissues and cells e the maximum period of storage before re-ex as well as the safety of tissue establishment personnel. If a tissue establishment entrusts one of the stages of processing to a third party, a written agree 7. Processing methods ment is needed between the tissue establishment and the third party. The tissue establishment must Processing methods must not render the tissues evaluate and select third parties on the basis of their or cells clinically inefective or harmful to the recip ability to meet the established standards. They should be designed to ensure the safety and The recommended time limits between pro biological functionality of prepared tissues and cells. Procurement, regular critical evaluation to ensure that they con processing and storage times must be documented in tinue to achieve the intended results. A written change-control procedure must The reagents used in preservation and pro be followed before any signifcant change is imple cessing should be of an appropriate grade for their mented in processing. A change-control procedure intended use, be sterile (if applicable) and comply ensures that the change is justifed, is documented with existing national regulations. Use of antibiotics and will not afect the quality of the product (see during procurement, processing and preservation Chapter 2). All relevant persons should be involved should be avoided if possible or at least be justifed in evaluation of the change. Pooling of diferent tissues and cells from Washing is performed as an initial step in pro two or more donors during processing is not rec cessing. Several types of washing solution may be The main processing procedures include, but used. Filtering procedure is used for collecting bone marrow into a collection bag, as well as for prepara Cleansing of procured material from sur tion procedures of various solutions using 0. Usually scalpels and scissors are helpful for that Lyophilisation or freeze drying is a dehydra procedure. It allows initial cleansing tissue to sublimate directly from the solid phase to of procured tissues for future shaping and formation the gas phase.
Syndromes
- About any allergies your child may have to medicine, latex, tape, or skin cleaner.
- The problem has not been occurring for a long time
- Improve control of your blood sugar.
- Diagnose arrhythmias
- Heart rhythm problems
- Amyotrophic lateral sclerosis, or ALS
Purchase viagra with fluoxetine 100/60mg line
Human infection was said to be common during the last century in the region of the Volga in the former Soviet Union impotence heart disease buy cheap viagra with fluoxetine on line, owing to the consumption of raw Melolontha bee tles; however, other studies have not confirmed human cases (Leng et al. Since 1970, human infection has necessitated emergency surgery on chil dren in three provinces in northern China and one in southern China. A study of hospi tal records demonstrated that in Liaoning province, more than 200 surgical interven tions were required for intestinal perforations, and that 115 cases of abdominal colic caused by macracanthorhynchosis were treated in another hospital (Leng et al. The Disease in Man: the pathologic effect and symptomatology of the human infection have not been well studied. The case histories recorded in China, which are the most numerous, refer to extreme cases with acute abdominal colic and perfora tion of the intestine. The two most recent cases in children required resection of a part of the jejunum, which had multiple perforations (Leng et al. The parasite produces an inflamma tory reaction that can progress to necrosis and the formation of small, sometimes caseous nodules. Clinical manifestations depend on the intensity of infection, the degree of penetration of the parasite into the intestinal wall, and, especially, the pres ence of a secondary bacterial infection. The most severe cases are due to perforation of the intestine, leading to peritonitis and death. Source of Infection and Mode of Transmission: the development of the para site requires an intermediate host. Swine are infected by ingesting scarabaeid coleopterans, which serve as intermediate hosts. In China, besides these scarabaeids, members of the family Carambycidae were found infected with the larvae of the last immature stage of the acanthocephalus (cystacanth) (Leng et al. Man becomes infected in a man ner similar to swine, by accidental or deliberate ingestion of coleopterans. Most infections occur in children from rural areas, who catch beetles for play, and some times eat them lightly toasted but insufficiently cooked to kill the larvae. In south ern China, some peasants believe that coleopterans are effective against nocturia and administer them to children for that reason. Diagnosis: Diagnosis can be made by confirming the presence in the feces of thick-shelled eggs containing the first larval stage (acanthor). The adult parasite can be examined after the patient is treated with piperazine citrate and expels it. Control: Human infection can be prevented by avoiding the ingestion of coleopterans. To control the parasitosis in swine, the animals should be kept under hygienic conditions and provided with abundant food to discourage rooting and ingestion of coleopterans. Human infection with Macracanthorhynchus hirudi naceus Travassos, 1916 in Guangdong Province, with notes on its prevalence in China. Gastrointestinal helminth parasites of the black rat (Rattus rattus) in Abeokuta, southwest Nigeria. Intestinal perforation due to Macracanthorhynchus hirudinaceus infection in Thailand. Etiology: the agents of this disease are the metastrongylid nematodes Angiostrongylus (Morerastrongylus) costaricensis, A. The first of these nematodes was recognized as a parasite of man in Taiwan in 1944; the second was described in Costa Rica in 1971, although the human disease had been known since 1952; the third was identified in Japan in 1990 and was subsequently diagnosed in aborigines in Malaysia. The first species is responsible for abdominal angiostrongyliasis; the second for eosinophilic meningitis or meningoencephalitis; and the third, A. Some 12 other rat species have been found to be infected; coatis (Nasua arica), monkeys (Saguinus mystax), and dogs can be exper imentally infected. The female lays eggs in those arteries; the eggs are then carried by the bloodstream and form emboli in the arterioles and capillaries of the intestinal wall. The eggs mature and form a first-stage larva which hatches, penetrates the intestinal wall to the lumen, and is carried with the fecal matter to the exterior, where it begins to appear around the twenty-fourth day of the prepatent period of the infec tion. In order to continue their development, the first-stage larvae have to actively penetrate the foot of a slug of the family Veronicellidae (particularly Vaginulus ple beius) or be ingested by it. In Brazil, four species of Veronicellidae slug were found to be infected: Phyllocaulis variegatus, Bradybaena similaris, Belocaulus angustipes, and Phyllocaulis soleiformis (Rambo et al. In the slug, the lar vae mature and change successively into second and third-stage larvae in approxi mately 18 days. When the definitive host ingests the infective larva in the free state or inside the mollusk, the larva migrates to the ileocecal region, penetrates the intestinal wall, and invades the lymphatic vessels. In this location the larvae undergo two molts before migrating to their final habitat: the mesenteric arteries of the cecal region. The parasite can complete the life cycle in man, an accidental host, reaching sexual maturity and producing eggs, but the eggs usually degenerate, caus ing a granulomatous reaction in the intestinal wall of the host. The intermediate hosts are various species of land, amphibian, or aquatic gastropods. The definitive hosts can become infected by ingesting the infective third-stage larvae, either with infected mollusks or with plants or water contaminated with the larvae that abandon the mollusk. In addition, infection can occur as a result of consuming transfer hosts (paratenic hosts), such as crustaceans, fish, amphibians, and reptiles, which in turn have eaten infected mol lusks or free larvae. When a definitive host ingests an infected mollusk or infective larvae, the larvae penetrate the intestine and are carried by the bloodstream to the brain, where they undergo two additional changes to become juvenile parasites 2 mm long. From the cerebral parenchyma, they migrate to the surface of the organ, where they remain for a time in the subarachnoid space and later migrate to the pul monary arteries, where they reach sexual maturity and begin oviposition. The eggs hatch in the pulmonary arterioles or their branches, releasing the first-stage larva, which penetrates the pulmonary alveoli and migrates through the airways to the pharynx; there it is swallowed and is eliminated with the feces starting six weeks after infection. Snails or slugs, which are the intermediate hosts, become infected when they ingest the feces of infected rodents. The third-stage infective larva forms in the mollusk in 17 or 18 days and can remain there for some time or be expelled and contaminate the envi ronment. A large number of paratenic or transport hosts, such as crustaceans, fish, amphibians, or reptiles, may become infected with these larvae and, in turn, infect rats or human beings. The adult parasite has been found in rats, and its larva infects the snail Biomphalaria glabrata, although not as easily as it infects A. It has been iden tified in children in Costa Rica since 1952, and more than 130 human cases had been diagnosed when Morera and Cespedes described the parasite in 1971. Morera (1991) indicated that about 300 cases a year were diagnosed in Costa Rica alone. In 1992, two cases were discovered in children on the French island of Guadeloupe in the Caribbean (Juminer et al. With respect to the animal definitive hosts, 15% of Rattus norvegicus and 6% of R. In Panama, the adult parasite was found in five species of rodents belonging to three different families. It is highly probable that the parasitosis is much more wide spread than is currently recognized. In 1992, 27 cases had been reported in Japan, the majority in the prefecture of Okinawa. It is believed that the parasite was introduced to the island some years ago by rats from a ship from Asia. Since 1950, cases have been identified in Indonesia (island of Sumatra), Philippines, Taiwan, and even Tahiti. It subsequently appeared in Australia, mainland China, India, and Japan (Okinawa). The Disease in Man: the clinical manifestations of abdominal angiostrongylia sis caused by A. Leukocytosis is characteristic (20,000 to 50,000 per mm3), with marked eosinophilia (11% to 82%).
Discount 100/60 mg viagra with fluoxetine free shipping
Know the pathophysiology of the genetic mutations that result in congenital hyperinsulinism 20 impotence grounds for divorce states discount viagra with fluoxetine 100/60mg. Understand the difference between focal and diffuse causes of congenital hyperinsulinism and know the diagnostic tests used to differentiate between them 21. Recognize that hypoglycemia secondary to hyperinsulinism may be due to exogenous insulin and sulfonylureas C. Know the biochemistry of glucagon biosynthesis and the factors that regulate glucagon release b. Understand mechanisms of action of glucagon on glycogenolysis and the role of glucagon in the regulation of the blood glucose concentration 2. Understand the use of glucagon as a diagnostic and therapeutic tool in hypoglycemia 2. Know that some extracellular calcium is bound to serum proteins, primarily albumin, while some extracellular calcium is ionized or free 2. Know that in hypoalbuminemia, the total serum calcium concentration is often low despite a normal ionized calcium 4. Know that acidosis decreases binding of calcium to serum proteins and thus, in acidosis, the total serum calcium is often low despite a normal ionized calcium 5. Recognize the preanalytical factors (eg, prolonged exposure to air, temperature, excess heparin) which may affect accurate laboratory measurement of ionized calcium b. Understand the difference between passive and active intestinal calcium absorption and identify the factors (calcium load, hormonal regulation) affecting each 2. Recognize that in hyperparathyroidism, hypercalciuria is due to the effect of increased extracellular calcium concentration on the kidney and is not due to increased parathyroid hormone concentration b. Know the effects of thiazide diuretics, corticosteroids, and furosemide on renal excretion of calcium 3. Know that calcium is important for neural function, particularly at the neuromuscular junction, and that decreased extracellular calcium concentration causes increased neuromuscular excitability, accounting for many of the symptoms of hypocalcemia 2. Recognize that phosphate shifts between extracellular and intracellular compartments and know which factors influence this movement 3. Understand that the kidney acts to conserve magnesium during magnesium depletion d. Know that hypocalcemia may be refractory to therapy when serum magnesium concentration is decreased 3. Recognize the suppressive effect of hypermagnesemia on parathyroid hormone secretion B. Be aware that congenital hypoparathyroidism may be inherited as an autosomal dominant, autosomal recessive, or X-linked recessive trait 2. Know that acquired hypoparathyroidism may be a complication of thyroid surgery or, rarely, radioactive iodine therapy 4. Know that hypocalcemia that occurs in hypoparathyroidism is partly due to decreased synthesis of calcitriol 6. Know the clinical features of hypoparathyroidism including ectopic (particularly intracranial) calcification 8. Know that functional hypoparathyroidism can result from activating mutations or antibody-mediated stimulation of the calcium-sensing receptor of the parathyroid cells 10. Know which medications are used to treat children with hypoparathyroidism and how to adjust doses b. Recognize the findings in patients with pseudohypoparathyroidism and in patients with progressive osseous heteroplasia 4. Recognize the laboratory findings, including gene analysis, in patients with pseudohypoparathyroidism 7. Be familiar with the diagnosis of familial hypocalciuric hypercalcemia and know how to distinguish it from other forms of hypercalcemia 2. Know the molecular cause and inheritance pattern for familial hypocalciuric hypercalcemia and its relationship to severe neonatal hyperparathyroidism c. Recognize the biochemical profile consistent with "hungry bone syndrome" after parathyroidectomy for severe hyperparathyroidism 2. Know that vitamin D is produced in the skin by the action of ultraviolet light on 7-dehydrocholesterol 2. Know that the photocatalyzed conversion of 7-dehydrocholesterol to vitamin D proceeds faster in light-skinned persons than dark-skinned persons 3. Know that ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3) can be derived from plant and animal dietary sources respectively and that the two molecules are metabolized similarly b. Understand the regulation of 1-alpha hydroxylase activity by phosphate, parathyroid hormone, and 1,25-dihydroxyvitamin D d. Know that 1-alpha hydroxylase activity exists in some neoplastic and inflammatory monocytes and in macrophages, particularly in sarcoidosis 2. Know that serum 25-hydroxyvitamin D concentrations primarily reflect vitamin D nutritional status b. Know that 1,25-dihydroxyvitamin D concentrations may be elevated in children with rickets due to phosphate or vitamin D deficiency c. Know that 1,25-diydroxyvitamin D binds to a cytoplasmic receptor that is a member of the steroid receptor superfamily and that the receptor binds to promoters to alter transcription of the target genes b. Recognize that 1,25-dihydroxyvitamin D is the primary stimulator of intestinal calcium transport c. Understand that nutritional vitamin D deficiency occurs only if there is both insufficient dietary intake of vitamin D and insufficient sun exposure 2. Recognize that nutritional vitamin D deficiency can cause rickets, and less commonly, hypocalcemia 3. Recognize that anticonvulsant therapy may be associated with vitamin D deficiency 4. Know the typical pattern of biochemical abnormalities in vitamin D deficiency rickets 5. Understand the importance of the intestinal mucosa, biliary tract, and pancreatic enzymes in the absorption of dietary vitamin D, and that vitamin D metabolites undergo enterohepatic circulation 2. Recognize the gastrointestinal causes of childhood vitamin D deficiency: short-bowel syndrome, celiac disease, biliary obstruction, and other causes of fat malabsorption 3. Understand the pathophysiology of the secondary hyperparathyroidism that accompanies renal insufficiency 2. Recognize that 1,25-dihydroxyvitamin D values are decreased in patients with chronic renal insufficiency and understand the pathophysiological basis for the decreased concentrations 3. Know that deficiency of calcidiol 1 alpha-hydroxylase results in rickets (previously termed Vitamin D-dependent rickets type 1) which is inherited in an autosomal recessive pattern 2. Know that vitamin D insensitivity is associated with mutations in the gene encoding the vitamin D receptor 2. Recognize that insensitivity to calcitriol causes vitamin D-dependent rickets type 2 (hereditary vitamin D-resistant rickets) and know the phenotype of that condition, which includes alopecia f. Recognize that early onset neonatal hypocalcemia frequently reflects intrauterine and postnatal insults such as type 1 diabetes, toxemia of pregnancy, or premature or traumatic delivery 3. Know that late onset neonatal hypocalcemia may be due to excessive phosphate intake, hypomagnesemia, or congenital hypoparathyroidism 4. Know that, in patients with hypomagnesemia, eucalcemia is achieved by administration of magnesium 5. Know that maternal hypercalcemia can cause neonatal hypocalcemia and the mechanism involved 6. Recognize that hypoparathyroidism in the newborn and early infancy periods may spontaneously abate, particularly when it is caused by maternal hypocalcemia b. Know that hypocalcemia can be due to inadequate calcium intake, particularly in infants c. Know the various causes of hypocalcemia and how to determine the etiology of hypocalcemia by clinical and laboratory evaluation 2. Know the available therapies for children with hypoparathyroidism and their potential adverse effects 3. Recognize the therapeutic usefulness of various forms of vitamin D (vitamin D, calcidiol, 1-alpha hydroxyvitamin D, calcitriol, and dihydrotachysterol), including vitamin D metabolites or analogs which do not raise serum calcium 4. Know the various mechanisms by which malignant diseases increase serum calcium concentrations 2. Know that Williams syndrome is associated with developmental delay, supravalvular aortic stenosis and a characteristic facies 2. Know that Williams syndrome is associated with infantile hypercalcemia that usually resolves spontaneously c. Know that immobilization can cause hypercalcemia because of increased bone resorption.
Buy 100/60 mg viagra with fluoxetine visa
Reporting may take place before the investigation is complete due to the lengthy investigations that can take place erectile dysfunction book 100/60mg viagra with fluoxetine amex. Other expert help may be required from reference laboratories and infectious disease experts. These donors typically would be deferred by proper eye evaluation prior to tissue collection. However, if malignancy transmission is reported, a proper investigation and reporting is appropriate. Aseptic Technique: Method by which contamination with microorganisms is prevented. Complaint: Any written or oral communication concerning dissatisfaction with the identity, quality, packaging, durability, reliability, safety, effectiveness, or performance of tissue. Consignee: Any eye bank, eye banking intermediary or transplanting surgeon (whether individual, agency, institution, or organization) that receives tissue and assumes responsibility for any step in the processing, storage, distribution and/or use of such tissue. Distributing Establishment: An entity that is reimbursed for or invoices for providing tissue to the end user. Shall be responsible for tracking recipient or consignee information, post-op follow-up and reporting any adverse reaction to the source establishment. End User: A hospital, surgeon, surgical center, research center or any entity that utilizes tissue provided by an eye bank. Processing Establishment: the entity that performs post-recovery tissue preparation. Processing: Any activity performed on the eye tissue, other than recovery, donor screening, donor testing, storage, labeling, packaging, or distribution, such as: testing for microorganisms; preparation; sterilization; steps to inactivate or remove adventitious agents; preservation for storage; manipulation/sizing; and removal from storage. Any manipulation of the ocular tissue intended for transplant that involves opening a previously sealed container after recovery. Quarantine: the identification of ocular tissue as not currently eligible for transplantation, including ocular tissue that has not yet been characterized as being eligible for transplantation. Quarantine includes the storage of such tissue in an area clearly identified for such use, or other procedures, such as automated designation, to prevent the premature release of such ocular tissue for transplantation. Source Establishment (or Facility): the entity that releases tissue following donor eligibility determination, and is responsible for maintaining donor records and evaluating adverse reaction reports. Storage Establishment: the entity that stores tissue at any time prior to distribution to the end user. Manifestations of infection include endophthalmitis, keratitis, or systemic infectious disease. Manifestations of biologic dysfunction include immediate endothelial failure (primary graft failure and early regraft), donor corneal dystrophy, malignancy, or evidence suggestive of prior refractive surgery. You may return to a previously completed step at any time but may not jump ahead to incomplete steps. Changes will not be saved unless you click on the Save and Continue>> button at the bottom of the page. Clicking on any other link or button on the page will cause your changes to be discarded. Once you have entered the information, click the "Save and Continue >> " button at the bottom of the page. Below are screen shots of all eleven of the reporting sections, including: Introduction; Contact; Adverse Reaction; Surgery; Recipient; Microbiology Records; Tissue Mate Status; Donor; Tissue Source; Tissue Return; Comments. If you need to change an item, use the links to the left or click one of the [change] links. Committee Reports: Policy & Position Research Subcommittee Committee Reports: Accreditation Board Committee Reports: Certification Board Eye Bank Association of America, Certification Board To: Medical Advisory Board, Eye Bank Association of America From: Patrick Gore, Chair Date: 5/21/2014 Re: Certification Board Report the Certification Board met on May 14, 2014. Here are the results from the Fall and Spring Exams: Spring Exam Results: the Spring Exam took place April 5-19, 2014. There was no new business brought up before the Certification Board for this meeting. Committee Reports: Technician Education Committee Committee Reports: Technical Procedures Manual Tony Bavuso From: Mike Tramber <mtramber@nceyebank. The inclusion of both documents was approved during the November 2013 meeting; however, the section is new. Residual ethanol content of donor sclera after storage in 95% ethanol and saline rinse of various durations. Sclera must be preserved using aseptic the hood, biosafety cabinet, or on the work technique, the same as when preserving corneal surface of an open container processing room. Preserve sclera at time of corneal preservation or refrigerate remaining ocular tissue following removal of corneas and preserve sclera later within time frame determined by the eye bank medical director. If sclera is stored for later preservation, wipe down the work surface of the hood, cabinet, or open container processing room with a disinfectant solution immediately after use and allow it to air dry. Perform surgical hand antisepsis and don sterile gloves and sterile gown or sleeves. Note any abnormalities of the globe such as forceps and place onto the center of the sterile discoloration, tumors, or thinning. Perform a careful inspection of the information regarding ocular history noted on the remaining ocular tissue. Since conjunctival tissue is an excellent medium fascia, or connective tissue that remains for bacterial growth, it is important to rid the adhered to the whole globe. Carefully excise any sclera of as much excess conjunctiva as attachments using iris scissors and tissue possible. Running scissors between the sclera and iris scissors between the sclera and choroid choroid layers helps to gently separate the layer of the globe. Using forceps, iris scissors, choroid layer from the scleral wall and facilities a sterile gauze or cotton tipped applicators, clean dissection of the intraocular material. Facilitates complete removal of all tissue or gauze, clean the inside of the globe to remove particulate material. Gauze, remaining tissue fragments and reduces the applicator, or entire globe may be soaked in microbial flora. Scleral tissue should reshaping becomes difficult, even after soaking be as smooth and round as possible prior to in sterile normal saline prior to surgery. If sclera is to be segmented, section the sclera into desired sizes prior to placing in storage medium. Using sterile cotton-tipped applicator or forceps gently place clean sclera into prepared sterile jars containing selected storage medium. Prevents contamination of ocular tissue by lids with shrink-wrap, or other sealing material. All ocular tissue must be labeled with a unique identification as follows: eye bank identification record number for proper quality control assurance. Preservation method: Glycerin, concen tration of alcohol used, or frozen tissue D. Statement that ocular tissue is for single patient use and culturing is recommended. Accomplishes complete dehydration of the applicator, clean sclera is placed in either scleral tissue. Retards microbial growth and is ophthalmic broad-spectrum antibiotic bacteriocidal. Aseptically remove the sclera from the antibiotic solution and place in sterile container that will withstand ultra low freezing temperatures. Instructions in the form of a package insert for reconstituting or re-hydrating the sclera and preoperative handling must be provided with the 7 tissue to the receiving surgeon. Additionally, positive serological results would be reported back to other associated agencies. Eye banks sharing donors with affiliated organizations should establish a protocol to receive positive serology results from those affiliated organizations. Follow up with specific recipients will be at the discretion of the transplanting surgeon. Any tissue in stock from donors with conflicting serology results will be quarantined and discarded. References 22 Page 3 of 23 the Associations recognize the efforts of the following individuals who generously donated their time and expertise to creating this updated document. Interviews may be conducted face to face, often in a hospital setting for a potential organ/tissue donor, but, more often, the interview is conducted by telephone for a potential tissue donor.
Purchase viagra with fluoxetine 100/60mg with visa
There are no findings that would allow di erentiation of a metastatic tumor from a primary neoplasm on clinical grounds erectile dysfunction drugs non prescription effective 100/60mg viagra with fluoxetine. Sm all-cell carcin om a m et ast at ic t o t h e brain is m ost likely from t h e lu n g. Di erential diagnoses include: primary brain tumor (glio blastoma, low grade astrocytoma), abscess, and nonspecific inflammatory reaction. This improvement is not permanent, and prolonged steroid administration may produce side e ects; see Possible deleterious side e ects of steroids (p. If m u lt ip le le sion s of kn ow n small-cell Ca are detected on cerebral imaging, treatment of choice is radiation plus chemotherapy. In p at ien t s n ot con sid e red for su rger y, st eroid s an d rad iat ion m ay be p alliat ive. H/A are u su ally 46 reduced, and in 50%of cases symptoms improve or completely resolve. Th is d o e s n o t r e su lt in local control for the m ajority of these patients and they frequently succum b from progressive brain disease. W it h t h is d o se, 1 1 % o f 1 yr su r vivor s and 50%of 2-yr survivors develop severe dementia. Th is is a cce p t a b le in p at ie n t s n o t e x p e ct e d t o live lo n g e n o u g h t o get long-term radiation e ects. Th e se low d o se s a r e a lso a sso cia t e d w it h a h igh e r r a t e o f r e cu r r e n t b r a in metastases. Does n ot obtain t issu e for h istological an alysis, an d gen erally can n ot be used for lesions >3 cm. Also, in n e w ly d ia gn o se d ca n ce r p a t ie n t s, cr a n iot o m y m ay d e lay s ys t e m ic treatment for weeks and the ramifications of this need to be considered. Mult iple lesions Patients w ith m ultiple m etastases generally have m uch worse survival than those w ith solitary 50 lesions. However, if total exci sion of all mets is feasible, then even multiple mets may be removed with survival similar to those 32 having a single met removed (also see Ta b le 5 2. The mortality of remov ing > 1 m et at a single sitting is not statistically significantly higher than rem oving a single m et. This is palliative treatm ent to reduce the symptom/threat from that particular lesion 2. Includes cases with no definite diagnosis and: a) deep lesions b) multiple small lesions 2. For lesions not visi ble on the surface nor palpable immediately beneath the surface, intra-operative ultrasound or ster eotactic techniques may be used to localize the lesion. Metastases usually have a well defined border, thus a plane of separation from normal brain may be exploited, often allowing gross total removal. Patients with solitary mets and no 46,55 evidence of active systemic tumor have the best prognosis. However, a prospective (non-random ized, 54 retrospectively matched) study fou n d a m ed ian su r vival of 7. Most frequent symptoms: H/ A, m e n t a l st a t u s ch a n ges, le t h a r g y, se izu r e, a t a x ia. The Role of Radiation Following Surgical [17] Slotman B, Faivre-Finn C, Kramer G, Rankin E, Snee Excision. The Single Prophylactic cranial irradiation in extensive small-cell Supraten torial Lesion: An Evaluation of Preopera lung cancer. Th e Risks of Me t ast ase s fr om Sh u n t in g in Ch ild r e n Dem ographics, Prognosis, and Therapy in 702 with Primary Central Nervous System Tumors. Brain metastases: epidemi tomography for metastatic detection in melanoma ology and pathophysiology. P o s t o p e r a t i v e r a d i o t h e r a p y i n t h e t r e a t approves Keytruda for advanced melanoma. A of Postoperative Radiotherapy After Resection of Ran d om ized Trial of Su rger y in th e Treat m en t of Single Brain Metastases. De t e r m in a n t s o f o u t co m e in m e la n o m a p a t ie n t s in the Treatment of Brain Metastasis. Resection for Solitary Brain Metastasis: Role of K, Bo st r o e m A, He e se O, Ko e lb l O, Ga r b e C, Sch a d e n Adju van t Rad iat ion an d Progn ost ic Var iab les in 2 29 dorf D. Successful Laser prognostic factors in patients with brain metastases assisted Excision of a Metastatic Midbrain Tumor. Less commonly m ay initially m etastasize to lateral or posterior aspect of canal. Th e m ajo r it y a r e co m m o n p r im a r ie s that tend to metastasize to bone (lung, breast, prostate, renal-cell and thyroid). Rare tumors that 4 may go to bone include the myxoid subtype of liposarcoma (17% of these patients develop bone mets,5-year median survival is 16%). Bladder dysfunction (urinary urgency, hesitancy or retention) is the most com mon autonom ic manifestation; others include constipation or im potence. Sen sor y d ysfu n ct ion: an est h esia, h yp est h esia, or p arest h esias u su ally occu r w it h m otor d ysfu n c tion. Th e gr e a t e r t h e n e u r o lo gic d e ficit w h e n t r e a t m e n t is in it iat e d, t h e w o r s e t h e ch a n ce s fo r r e cove r y 1 of lost function. Th e y t yp ica lly p r e se n t in i tially with suboccipital and posterior cervical pain, and as the lesion progresses patients develop a characteristic pain that m akes it di cult to sit up (some will hold their heads in their hands to stabi lize it). An t e r io r a p p r o a ch e s fo r st a b iliza t io n a t t h is lo ca t io n a r e d i cult. For others, good pain relief and stabilization m ay be achieved w ith radiation fol lowed by posterior fusion. Features that help distinguish conus lesions from cauda equina are shown in Ta b le 5 3. By i t s e l f, h a s l o w s e n s i t i v i t y fo r s p i n a l cord compression by tum or. Patients m ay be categorized into one of the three groups that follow s which outlines the subsequent steps. In a pa tient with suspected spine mets, the goals of management are: Asse ssm e n t o f n e u r o lo gic in vo lve m e n t a n d t im elin e o f n e u r o lo gic ch a n ge s. These patients have a high risk of rapid deterioration and require immediate evaluation. St e r o id s m ay t e m p o r a r ily m a s k lym p h o m a (o n im a gin g a n d a t s u r ge r y), h ow e ve r, in t h is gr o u p the benefit of giving steroids usually outweighs this pitfall 2. Ca n b e e va lu a t e d a s o u t p a t ie n t o ve r s e ve r a l d a ys (m o d if y based on ability of patient to travel, reliability, etc. Treatm ent goals are palliative: pain control, preser vation of spinal stability, and m aintenance of sphincter control and ability to am bulate. Th e m o st im p o r t a n t fact o r a ecting prognosis, regardless of treatment modality, is ability to walk at the time of initiation of therapy. Ve r t e b r o p l a s t y / k y p h o p l a s t y Ve r t e b r o p l a s t y / k y p h o p l a s t y (p.